Sarcoid-like reaction induced by aspirin treatment following aspirin desensitization in a patient with aspirin-exacerbated respiratory disease



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Sarcoid-like reaction induced by aspirin treatment following aspirin desensitization in a patient with aspirin-exacerbated respiratory disease
Aspirin‑exacerbated respiratory disease (AERD) is a chronic inflammatory condition characterized by asthma, chronic rhinosinusitis with nasal polyps, and hypersensitivity to aspirin and other cyclooxygenase‑1 inhibitors.1 We report a case of a 27‑year‑old woman with AERD, who developed cutaneous and pulmonary manifestations suggestive of a drug‑induced sarcoid‑like reaction during long‑term high‑dose aspirin therapy after aspirin desensitization.
Following desensitization in 2017, the patient was maintained on high‑dose aspirin therapy. Initially, she received 325 mg twice daily. Due to limited availability of 325‑mg Tablets, the dose was adjusted to 300 mg twice daily. At that time, biologic therapies were not yet widely available, and aspirin desensitization remained a standard approach for AERD. On this regimen (600 mg/day), the patient maintained good disease control, and no adverse effects occurred. She also received inhaled and intranasal corticosteroids and a long‑acting β2‑agonist.
In September 2021, the patient presented with persistent, erythematous, and pruritic skin lesions on her arms, and erythema nodosum‑like lesions with bruising on her legs (Figure 1A and 1B), along with recurrent urticaria episodes. Laboratory tests showed mild eosinophilia (eosinophils, 440/mm3; reference range [RR], 50–400/mm3), elevated serum immunoglobulin E (142 IU/ml; RR <100 IU/ml), and a positive circulating antinuclear antibody titer of 1:320 (RR <1:160)—evidence of autoimmune disease. Serum and urinary calcium levels were normal.
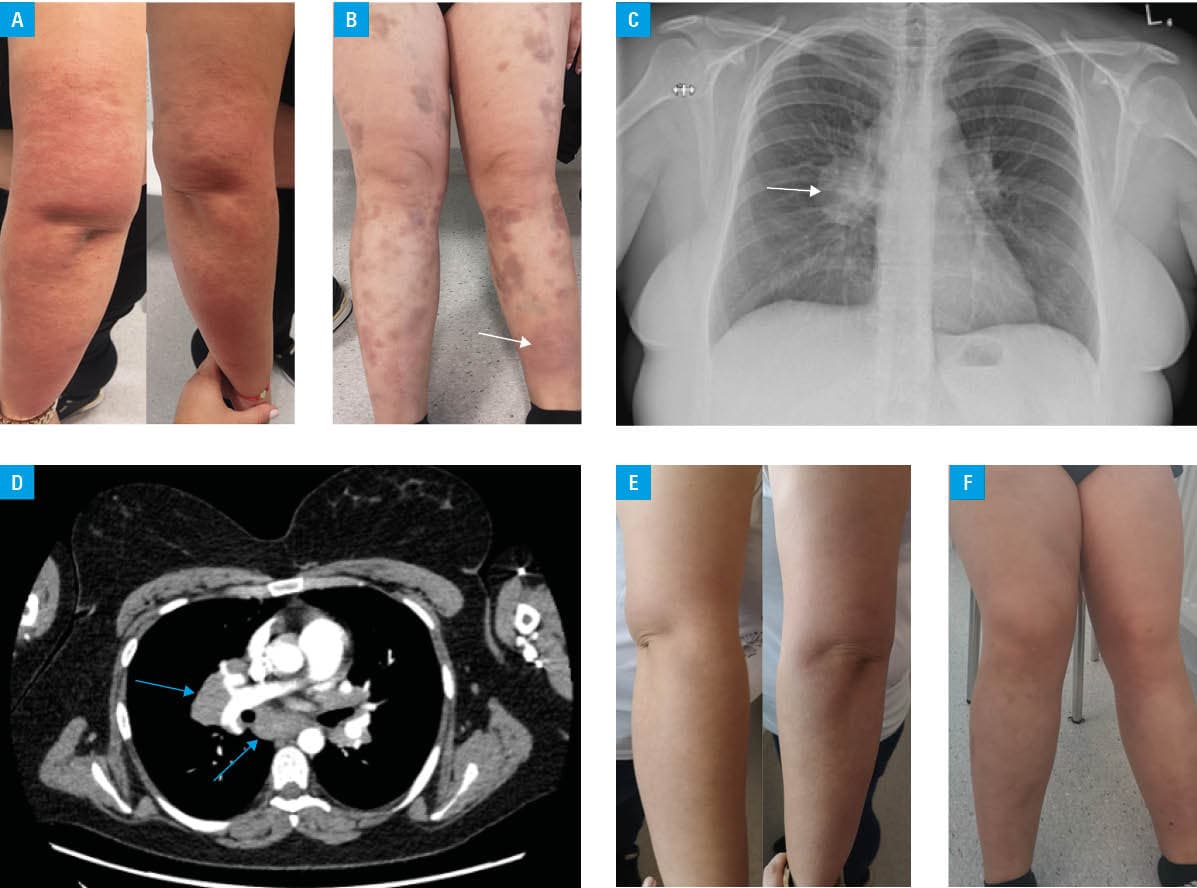
Chest X‑ray showed enlargement of the right hilum (Figure 1C). Contrast‑enhanced computed tomography demonstrated enlarged lymph nodes (Figure 1D). These findings raised a suspicion of sarcoidosis, with a differential diagnosis including lymphoma.2
Bronchoscopy with endobronchial ultrasound and transbronchial lymph node biopsy demonstrated non‑necrotizing granulomas with fibrosis. Bronchial biopsy identified chronic inflammation and focal eosinophilia. Bronchoalveolar lavage (BAL) fluid analysis showed macrophages (77%) and lymphocytes (20%) with eosinophils (2%) and neutrophils (1%). Neither cytology nor BAL findings were typical of sarcoidosis.
Skin biopsy from the shin showed features of sarcoidosis, consistent with a drug‑induced reaction or eczematous dermatitis. Aspirin therapy was discontinued due to suspected drug‑induced etiology. One month after aspirin cessation and topical corticosteroid treatment, the skin lesions regressed (Figure 1E and 1F). Follow‑up chest X‑ray in February 2022 was normal.
This case highlights a rare, likely drug‑induced sarcoid‑like reaction mimicking sarcoidosis, characterized by non‑necrotizing granulomas in the lungs and lymph nodes, triggered by external factors, such as medications, infections, and environmental exposures.3,4 During the diagnostic process, sarcoidosis, drug‑induced sarcoid‑like reaction, and lymphoma were considered. Lymphoma was initially suspected due to mediastinal lymphadenopathy; however, the histopathologic findings and clinical course did not support this diagnosis. The presence of granulomas without typical bronchial sarcoid features, eosinophilic infiltration, mildly elevated BAL lymphocytes (20%, as compared with over 40% in typical sarcoidosis; RR, 5%–15%), and slight eosinophilia (2%, as compared with normal values <1%) supported a drug‑induced mechanism.5 The lack of granulomas on skin biopsy indicated pulmonary‑limited involvement. Resolution of symptoms after aspirin withdrawal supported causality.
To our knowledge, this is the first reported case linking long‑term aspirin therapy in AERD to sarcoid‑like pulmonary and cutaneous manifestations. Clinicians should consider this potential adverse effect in patients receiving chronic high‑dose aspirin therapy.
- Imam KH, Woessner KM. Nonsteroidal anti‑inflammatory drug‑exacerbated respiratory disease: diagnosis and current management. Pol Arch Intern Med. 2023; 133: 16544. | Crossref
- Miedema J, Cinetto F, Smed‑Sörensen A, Spagnolo P. The immunopathogenesis of sarcoidosis. J Autoimmun. 2024; 10: 103 247. | Crossref
- Chopra A, Nautiyal A, Kalkanis A, Judson MA. Drug‑induced sarcoidosis‑like reactions. Chest. 2018; 154: 664‑677. | Crossref
- Cohen Aubart F, Lhote R, Amoura A, et al. Drug‑induced sarcoidosis: an overview of the WHO pharmacovigilance database. J Intern Med. 2020; 288: 356‑362. | Crossref
- Frye BC, Schupp JC, Rothe ME, et al. The value of bronchoalveolar lavage for discrimination between healthy and diseased individuals. J Intern Med. 2020; 287: 54‑65. | Crossref
ARTICLE INFORMATION