Assessment of noninferiority of oral vs subcutaneous semaglutide: a systematic review and meta-analysis
1 ,
Key words: adverse events, glycemic control, semaglutide, type 2 diabetes, weight loss
,
Key words: adverse events, glycemic control, semaglutide, type 2 diabetes, weight loss

 CC BY 4.0
CC BY 4.0
Assessment of noninferiority of oral vs subcutaneous semaglutide: a systematic review and meta-analysis
Introduction: This systematic review and meta‑analysis is the first to comprehensively compare oral and subcutaneous semaglutide for type 2 diabetes (T2D) management.
Objectives: Our aim was to determine whether oral semaglutide is noninferior to the subcutaneous preparation, assess potential superiority, and provide evidence‑based guidance for clinical decisions.
Patients and methods: We searched clinical trial registries and bibliographic databases through April 30, 2025. Twelve randomized controlled trials involving 6253 adults with T2D were analyzed. Following the PRISMA and Cochrane guidelines (PROSPERO, CRD420251017953), the data were extracted on efficacy, safety, and clinical outcomes. Noninferiority was assessed using predefined margins, and post hoc superiority analyses examined secondary end points. Evidence certainty was evaluated using the Grading of Recommendations Assessment, Development, and Evaluation criteria.
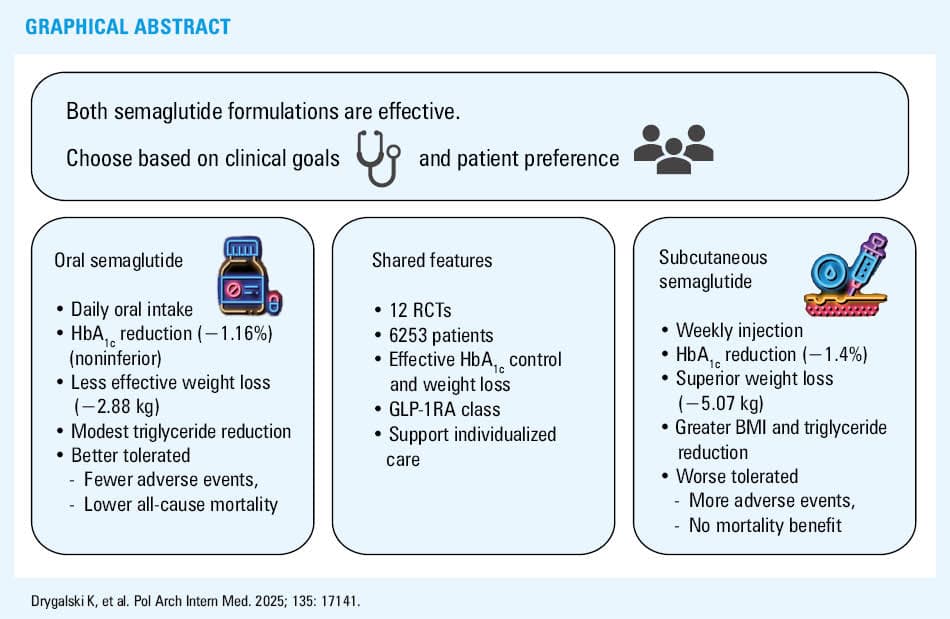
Results: Both formulations of semaglutide significantly reduced the level of glycated hemoglobin (HbA1c), that is, oral by 1.16 percentage points (95% CI, –1.22 to –1.09) and subcutaneous by 1.4 percentage points (95% CI, –1.47 to –1.33). Oral semaglutide met the noninferiority margin at 50% of the subcutaneous effect. Subcutaneous semaglutide was superior for weight loss (2.19 kg; 95% CI, –3.57 to –0.81; P <0.002), body mass index (BMI) reduction (0.88 kg/m2; 95% CI, –1.55 to –0.21; P <0.011), and triglyceride level lowering (0.09 mmol/l; 95% CI, –0.14 to –0.04; P <0.001).
Conclusions: Both forms of semaglutide effectively improve glycemic control in T2D. Oral semaglutide is noninferior to subcutanous semaglutide in lowering HbA1c level, while subcutaneous semaglutide is superior in weight, BMI, and triglyceride reduction. Given similar safety profiles and modest differences in other outcomes, treatment selection should be guided by clinical goals and patient preferences.
What's new?
This study is the first to systematically compare the effectiveness of oral and injectable semaglutide in lowering blood sugar level in patients with type 2 diabetes. While both forms control glucose levels effectively, the injectable one offers additional benefits in weight and triglyceride level reduction. Our findings suggest that patients and clinicians can consider the oral option without compromising glycemic control, potentially improving treatment adherence in individuals reluctant to use injections. The subcutaneous form may be favored in patients seeking additional benefits in weight management or triglyceride level reduction. Ultimately, formulation choice should be tailored to individual patient preferences, clinical goals, and comorbidities.
Introduction
Glucagon‑like peptide‑1 receptor agonists (GLP‑1RAs) have become a cornerstone of type 2 diabetes (T2D) and obesity management thanks to their pleiotropic metabolic effects extending beyond glycemic control and lowering the level of glycated hemoglobin (HbA1c). These effects include direct body weight regulation and cardiovascular protection.1 Semaglutide, a long‑acting GLP‑1RA, is unique in being available in both subcutaneous and oral formulations, offering flexibility in treatment options.2,3
The subcutaneous formulation of semaglutide, given once weekly, has significantly reduced HbA1c level and body weight in various clinical settings, as evidenced by the SUSTAIN (Semaglutide Unabated Sustainability in Treatment of Type 2 Diabetes) clinical trial program. Research trials demonstrated that subcutaneous semaglutide is superior to several other antidiabetic agents, including sitagliptin, liraglutide, and insulin glargine, in maintaining glycemic control and supporting weight reduction.2,4
Oral semaglutide, taken once daily, offers an option for patients who prefer to avoid injections. The PIONEER (Peptide Innovation for the Early Diabetes Treatment) clinical trial program has established the efficacy of oral semaglutide in reducing HbA1c level and body weight as comparable to its subcutaneous counterpart and superior to other oral antidiabetic agents, such as sitagliptin and empagliflozin.2,3,5
However, no clear evidence exists to determine whether subcutaneous or oral semaglutide is superior for managing T2D or obesity. To address the frequent patient concern regarding a possibility to avoid injections, we conducted a meta‑analysis of randomized controlled trials (RCTs), followed by a formal noninferiority assessment of oral vs subcutaneous semaglutide in individuals with T2D.
The preference for oral medications over injectables, observed in many patients, holds the potential for better compliance and improved clinical outcomes.3,6 That is why, when introducing a long‑lasting treatment, such as for T2D, a physician should consider patient preferences, particularly their aversion to injections, which can significantly impact adherence and overall treatment satisfaction. The current body of evidence is not sufficient to make a definitive recommendation on the superior route of administration, as both formulations have shown comparable efficacy and safety profiles. Our study aimed to guide clinical decision making, serving as a roadmap for personalized therapy, a critical goal in modern diabetes care.
Patients and methods
Study design and registration
We conducted a systematic review and meta‑analysis of the RCTs assessing the effect of subcutaneous and oral semaglutide in patients with T2D. A total of 12 RCTs involving 6253 patients with T2D were included. Of these, 2141 received oral semaglutide, 854 subcutaneous semaglutide, and the remaining were assigned to placebo comparators (1972 and 829, respectively, for oral and subcutaneous groups). The meta‑analysis was followed by a noninferiority evaluation of oral administration. The study was conducted following the Cochrane Collaboration guidelines and registered in the PROSPERO database (CRD420251017953).7 Its full protocol is available in Supplementary material.
Search strategy and eligibility criteria
The studies were searched and screened independently by 2 reviewers (KD and BM), with any doubts resolved by consensus with a third reviewer (KP). The Cochrane Library, PubMed, ClinicalTrials.gov, and ClinicalTrialsRegister.eu databases were searched for eligible RCTs up to April 2025. The search covered both published and unpublished studies without any language or date restrictions.8 The search terms included “semaglutide,” “subcutaneous,” “oral,” “SC,” “p.o.,” and “type 2 diabetes.”
The exact search strategy for PubMed was: ((semaglutide[Title/Abstract] OR semaglutide[MeSH Terms]) AND (subcutaneous[Title/Abstract] OR oral[Title/Abstract] OR SC[Title/Abstract] OR p.o.[Title/Abstract])) AND (type 2 diabetes[Title/Abstract] OR diabetes mellitus, type 2[MeSH Terms] OR T2DM[Title/Abstract]) AND (randomized controlled trial[Publication Type] OR RCT[Title/Abstract] OR placebo[Title/Abstract]). Filters were applied for humans and adults. For the Cochrane Library, the number 1 MeSH descriptor: (Diabetes Mellitus, Type 2) exploded all trees; number 2 semaglutide; number 3 (oral or subcutaneous or SC or p.o.); number 4 (numbers 1, 2, and 3). For ClinicalTrials.gov and ClinicalTrialsRegister.eu we searched for “semaglutide” AND (“oral” OR “subcutaneous”) AND “type 2 diabetes” AND “randomized” AND “placebo.”
We also checked the references of key reviews and meta‑analyses using a snowballing technique to identify additional studies. Any trial meeting the inclusion criteria was included in the analysis, if only publicly available results were provided.
RCTs on adult patients with T2D treated with semaglutide administered either subcutaneously or orally, compared to one another or placebo, were found eligible. Dietary interventions, physical exercises, and / or oral antidiabetic drugs were found to be eligible supplementary elements of both placebo and experimental groups.
Non‑RCT studies, nonadult populations, and studies comparing semaglutide with other antidiabetic drugs instead of placebo were excluded. Similarly, to increase transitivity, studies on patients requiring chronic use of insulin were found ineligible. We excluded RCTs involving patients with unstable or severe diseases / comorbidities, such as unstable angina, myocardial infarction, stroke, heart failure (New York Heart Association class IV), renal insufficiency (estimated glomerular filtration rate [eGFR] <30 ml/min/1.73 m2), liver failure (alanine aminotransferase 2.5 times above the upper limit of normal), and pregnancy.
Data extraction
Study details were extracted using a standardized form. The extracted data included study characteristics (eg, author, year, design, sample size), population details (eg, age, sex, baseline HbA1c level, comorbidities), intervention details (eg, dose, duration, formulation), and primary and secondary outcomes (eg, change in HbA1c level, body weight, blood pressure [BP], lipid profile, adverse events [AEs]).
The primary outcome of this review was a change in HbA1c level. Secondary outcomes included changes in body weight, BMI, waist circumference, systolic BP (SBP) and diastolic BP (DBP), lipid profile (total cholesterol, low‑density lipoprotein cholesterol [LDL‑C], high‑density lipoprotein cholesterol [HDL‑C], triglycerides), frequency of AEs, and all‑cause mortality.
Risk of bias assessment
The risk of bias for each study was evaluated using the Cochrane Risk of Bias 2 (RoB2) tool, assessing domains such as randomization, allocation concealment, blinding, incomplete outcome data, and selective reporting (Supplementary material, Table S1).8,9 Any disagreements between the reviewers were resolved through consensus or with the involvement of the third reviewer. If multiple treatment times were provided, data from the longest treatment arm were extracted. If multiple dosage regimens were provided, data from the group closest to 2.4 mg for subcutaneous and 14 mg for oral semaglutide were extracted.
To assess clinical significance, the results of the meta‑analysis of oral and subcutaneous semaglutide were compared with the preset thresholds. Changes in HbA1c level by 0.3%, in SBP by 5 mm Hg, DBP by 2 mm Hg, lipid profile parameters by 5%, weight loss of 5%, and BMI loss by 1 unit [kg/m2] were considered as clinically meaningful differences. Following the meta‑analysis, noninferiority of oral semaglutide was evaluated.
Certainty of evidence
Certainty of evidence for both the primary and secondary outcomes was assessed independently by 2 reviewers using the Grading of Recommendations Assessment, Development, and Evaluation criteria (Supplementary material, Table S2).8,10
Statistical analysis
Meta‑analysis approach
Clinical heterogeneity among the included studies was qualitatively assessed. Statistical heterogeneity was quantified using the τ² and I² statistics. A fixed‑effects model was employed if heterogeneity was low (I² <50%), while a random‑effects model was used for substantial heterogeneity (I² ≥50%). Initial data extraction and preliminary assessments were performed using Review Manager software, version 5.4 or later (The Cochrane Collaboration, Copenhagen, Denmark). All subsequent statistical analyses, noninferiority testing, and graphical visualizations were conducted using R software, version 4.3.0 (R Foundation for Statistical Computing, Vienna, Austria).
Measures of treatment effect
Continuous outcomes (HbA1c level, weight, BMI, waist circumference, lipid profiles, and BP) were summarized using mean differences (MDs) with corresponding 95% CIs. AEs and mortality were summarized as odds ratios (ORs) with 95% CI, analyzed using log‑transformed data.
Noninferiority analysis
Noninferiority was evaluated using prespecified margins corresponding to 50%, 70%, and 90% of the effect observed with subcutaneous semaglutide. The primary analysis focused on the 50% margin. Noninferiority was concluded if the upper bound of the 95% CI of the difference between the oral and subcutaneous formulations did not exceed the chosen noninferiority margin.
Exploratory superiority analysis
Superiority of subcutaneous over oral semaglutide was evaluated without a prespecified margin. Superiority was concluded if the 95% CI of the difference (subcutaneous minus oral) excluded 0 in the direction favoring the subcutaneous formulation (ie, CI entirely positive for the end points where higher is better, or entirely negative for the end points where lower is better). No false discovery rate correction was applied at this stage.
Handling of missing data
The primary analysis followed the intention‑to‑treat principle using the complete‑case data.
Results
Study population
A total of 12 RCTs involving 6253 patients with T2D were included in this meta‑analysis (see Supplementary material, Table S3 for detailed study characteristics). For the primary outcome, 2141 patients received oral semaglutide, 854 the subcutaneous form, and the remaining 1972 and 829 patients were assigned to respective placebos. Overall, the majority of participants were men (62.1%), at a mean (SD) age of 60.7 (9.51) years, and a mean (SD) initial HbA1c level of 7.99% (0.77%). The majority of the patient population was white (64.4%), 21.8% were Asian, 5.6% black, and 8.2% of another or unreported ethnicity. Comparing baseline characteristics of the patients with both administration routes, we found that the patients in the trials with oral semaglutide were slightly older (mean [SD] 62.9 [8.1] vs 55.4 [10.6] y), more often men (65.1% vs 54.5%), white (68.3% vs 54.7%), and had slightly higher completion rate (97% vs 94.3%) than the ones in the subcutaneous semaglutide trials. Detailed characteristics of the patient populations are shown in Table 1.
Parameter | Oral semaglutide (n = 2298) | Placebo (n = 2163) | Subcutaneous semaglutide (n = 904) | Placebo (n = 888) |
Data are presented as number (percentage) unless indicated otherwise.
Abbreviations: BMI, body mass index; HbA1c, glycated hemoglobin | ||||
Age, y, mean (SD) | 62.7 (8.1) | 63.1 (8.1) | 55.5 (10.65) | 55.4 (10.6) |
Women | 815 (35.5) | 740 (34.2) | 412 (45.6) | 404 (45.5) |
HbA1c, %, mean (SD) | 7.97 (0.7) | 8 (0.81) | 7.97 (0.76) | 8.02 (0.8) |
Weight, kg, mean (SD) | 89.9 (21.4) | 89.8 (21) | 31.9 (6.5) | 31.9 (6.4) |
BMI, kg/m2, mean (SD) | 89.3 (22.4) | 93.9 (21.8) | 31.9 (6.8) | 33.3 (6.8) |
Treatment completed | 2241 (97.5) | 2086 (96.4) | 851 (94.1) | 838 (94.4) |
Treatment not completed | ||||
Withdrawal by patient | 20 (0.9) | 15 (0.7) | 13 (1.4) | 21 (2.4) |
Lost to follow‑up | 9 (0.4) | 13 (0.6) | 17 (1.9) | 20 (2.3) |
Other | 1 (0.04) | 3 (0.1) | 22 (2.4) | 8 (0.9) |
Death | 27 (1.2) | 46 (2.13) | 1 (0.1) | 1 (0.1) |
Ethnicity | ||||
White | 1576 (68.6) | 1473 (68.1) | 489 (54.1) | 491 (55.3) |
Black | 118 (5.1) | 127 (5.9) | 54 (6) | 51 (5.7) |
Asian | 541 (23.5) | 510 (23.6) | 159 (17.6) | 151 (17) |
Other / unknown | 63 (2.7) | 53 (2.5) | 202 (22.3) | 195 (22) |
Primary outcomes
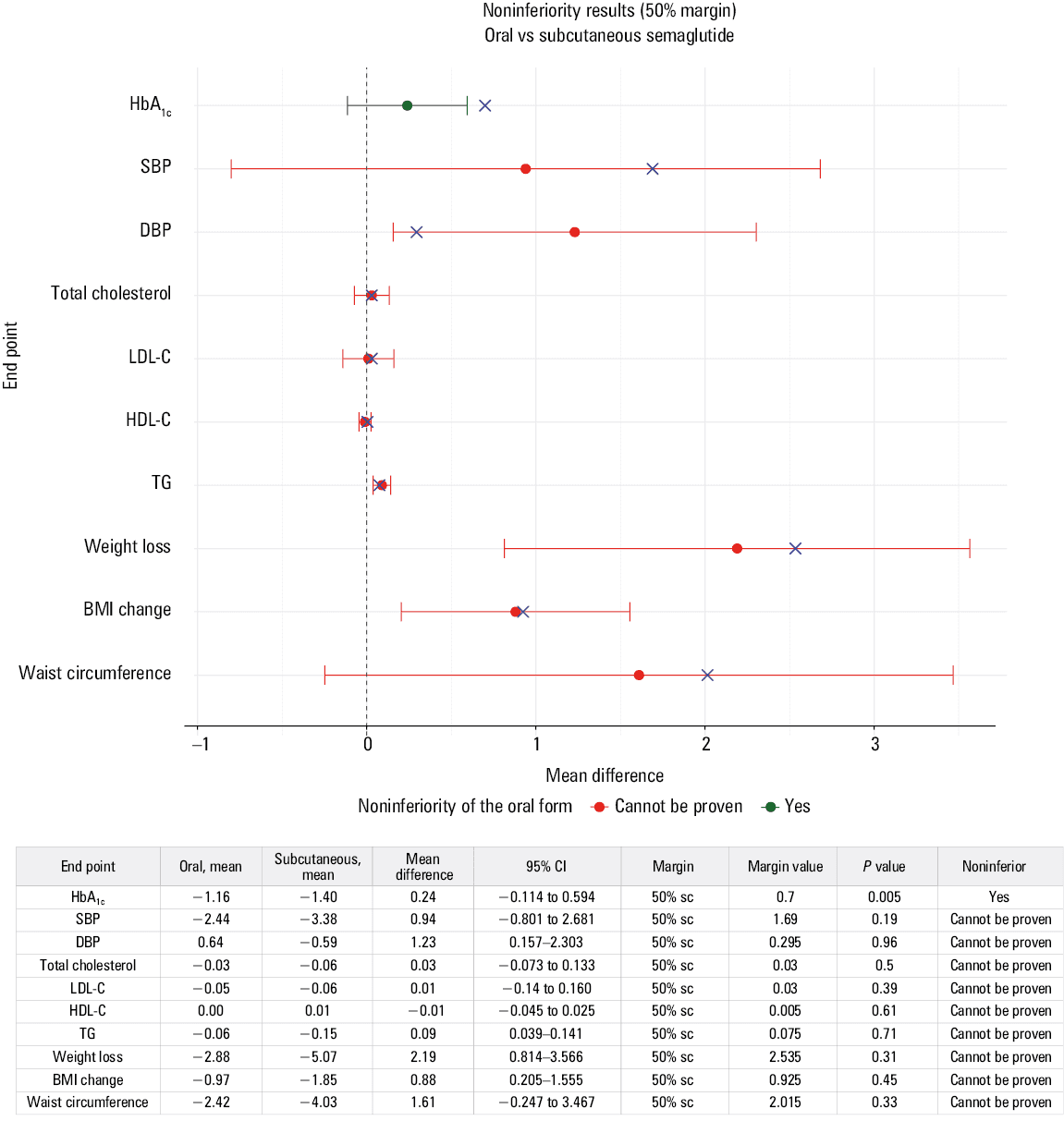
Given that semaglutide is approved as an antidiabetic medication, it was expected that both oral and subcutaneous formulations would achieve clinical and statistical significance in reducing HbA1c levels from baseline. Both formulations significantly reduced HbA1c level from baseline, oral by 1.16 percentage points (95% CI, –1.39 to –0.92), and subcutaneous by 1.4 percentage points (95% CI, –1.66 to –1.33; Table 2; Supplementary material, Figure S1). Subsequent noninferiority testing confirmed that oral semaglutide was not inferior to the injectable form using a 50% margin of the subcutaneous effect, although the results were inconclusive at higher margins (Figure 1; Supplementary material, Figure S2).
Outcome (mean change from baseline) | Oral semaglutide | Subcutaneous semaglutide | Mean difference subcutaneous vs oral semaglutide | P value |
Values represent mean changes from baseline with 95% CIs. Lipid outcomes represent a change in lipid profiles as ratio to baseline.
a Clinical significance; b Statistical significance; c Nonsignificant
Abbreviations: DBP, diastolic blood pressure; HDL‑C, high‑density lipoprotein cholesterol; LDL‑C, low‑density lipoprotein cholesterol; SBP, systolic blood pressure; others, see Table 1 | ||||
HbA1c, % | –1.16 (–1.39 to –0.92)a | –1.40 (–1.66 to –1.13)a | –0.24 (–0.59 to 0.11) | 0.18 |
SBP, mm Hg | –2.44 (–3.47 to –1.4)b | –3.38 (–4.78 to –1.98)b | –0.94 (–2.68 to 0.8) | 0.29 |
DBP, mm Hg | 0.64 (0–1.27)c | –0.59 (–1.45 to 0.28)c | –1.23 (–2.3 to –0.16)b | 0.024b |
Total cholesterol, ratio | –0.03 (–0.06 to –0.01)b | –0.06 (–0.16 to 0.04)c | –0.03 (–0.13 to 0.07) | 0.57 |
HDL‑C, ratio | 0 (–0.02 to 0.03)c | 0.01 (–0.04 to 0.06)c | 0.01 (–0.03 to 0.05) | 0.58 |
LDL‑C, ratio | –0.05 (–0.09 to –0.01)b | –0.03 (–0.21 to 0.08)c | –0.01 (–0.16 to 0.14) | 0.9 |
Triglyceride, ratio | –0.06 (–0.08 to –0.03)b | –0.15 (–0.19 to –0.1)a | –0.09 (–0.14 to –0.04)b | <0.001b |
Weight loss, kg | –2.88 (–3.47 to –2.3)b | –5.07 (–6.32 to –3.83)b | –2.19 (–3.57 to –0.81)b | 0.002b |
Weight loss ≥5%, odds ratio | 5.05 (3.62–7.07)b | 7.56 (3.6–15.87)b | – | – |
BMI, kg/m2 | –0.97 (–1.2 to –0.74)b | –1.85 (–2.49 to –1.22)a | –0.88 (–1.55 to –0.21)b | 0.01b |
Waist circumference, cm | –2.42 (–3.19 to –1.65)b | –4.03 (–5.72 to –2.34)b | –1.16 (–3.47 to –0.09) | 0.09 |
Abbreviations: TG, total triglyceride; sc, subcutaneous; others, see Tables 1 and 2
Secondary outcomes
The meta‑analysis indicated that both oral and subcutaneous semaglutide lowered SBP but did not achieve the clinical significance of a 5‑mm Hg change. For DBP, neither form reached statistical or clinical significance of a 2‑mm Hg change (Table 2; Supplementary material, Figure S1).
Regarding lipid profiles, oral semaglutide significantly reduced total cholesterol, LDL‑C, and triglyceride levels, presumably due to the relatively large sample size; however, these changes were not clinically meaningful. Subcutaneous semaglutide reached both clinical and statistical significance in lowering the levels of triglycerides but no other lipid profile parameters (Table 2; Supplementary material, Figure S3). Unfortunately, not all studies provided lipid profiles.
We could not consistently evaluate 5% weight loss due to inconsistent reporting across the analyzed RCTs. The noninferiority of oral semaglutide could not be proven for weight management parameters, BP, or lipid profile (Figure 1; Supplementary material, Figures S2 and S4). Instead, in a post hoc analysis, subcutaneous semaglutide showed superiority for weight loss (–2.19 kg; 95% CI, –3.57 to –0.81; P = 0.002), BMI change (–0.88 kg/m2; 95% CI, –1.55 to –0.21; P = 0.01), and lowering triglyceride level (change in triglycerides as a ratio to baseline, –0.09; 95% CI, –0.14 to –0.04; P <0.001; Table 2; Supplementary material, Figure S5).
Safety monitoring
In Figure 2, we present details on AEs and all‑cause mortality. Due to inconsistencies in AE reporting across the analyzed RCTs, safety monitoring was categorized into 3 groups: serious AEs (SAEs), all AEs, and all‑cause mortality. The PIONEER 6 study raised concerns, as it classified all AEs as SAEs, even relatively mild ones, such as iron deficiency anemia, abdominal pain, or nausea, with no nonserious AEs reported.11

Considering these discrepancies, the meta‑analysis of oral semaglutide RCTs showed no effect of the treatment on total AEs (OR, 1.5; 95% CI, 0.89–2.52) but a significant reduction in SAEs (OR, 0.81; 95% CI, 0.68–0.95) and all‑cause mortality (OR, 0.55; 95% CI, 0.34–0.9) in comparison with placebo. On the other hand, subcutaneous administration showed no difference from placebo in the odds of all‑cause mortality (OR, 1; 95% CI, 0.06–16) and SAEs (OR, 1.45; 95% CI, 0.53–3.92) but significantly increased the OR of AEs (OR, 3.22; 95% CI, 1.55–6.72; Figure 2).
Discussion
Combining the results of available RCTs, our meta‑analysis supports the use of both semaglutide formulations for effective glycemic control in the patients with T2D. Even though the noninferiority was confirmed at the relatively low margin of effect (50%), we could not prove any significant difference between the 2 formulations. The efficacy of once‑weekly subcutaneous semaglutide and once‑daily oral semaglutide has been investigated mostly in the SUSTAIN and PIONEER phase 3 clinical trial programs.6,11-31 Notably, most of these studies compared semaglutide with other antidiabetic agents, often in combination with additional therapies or in populations with varying degrees of the disease severity. Given that our primary objective was to determine whether one administration route is superior to another, and to assess whether possible differences in clinical effectiveness should influence the choice of the formulation, we aimed to ensure maximal comparability across the included studies. Therefore, we included only the trials conducted in similar conditions—specifically, the studies involving patients without severe comorbidities, comparing semaglutide with placebo, and excluding patients requiring insulin therapy. Overall, both formulations significantly reduced HbA1c levels, with subcutaneous semaglutide showing a reduction of 1.4 percentage points and oral semaglutide of 1.16 percentage points from baseline. Our findings suggest that both forms are similarly effective at improving glycemic control in the patients with T2D, offering flexibility without compromising outcomes. Although our study focused on comparing different formulations of semaglutide, Zhong et al4 demonstrated the superiority of semaglutide over other oral antidiabetic drugs in terms of glycemic control and weight loss. Their analysis did not statistically assess the difference between oral and subcutaneous semaglutide, nevertheless, they showed a reduction in HbA1c level similar to that observed in our analysis (1.37 percentage points for subcutaneous vs 1.02 percentage points for oral semaglutide). Notably, their meta‑analysis did not include more recent and large‑scale trials, such as PIONEER 6,24 PIONEER 11,26 or STEP 2 (Research Study Investigating How Well Semaglutide Works in People With Type 2 Diabetes Suffering From Overweight or Obesity),29 but included trials with active comparators and analyzed a more heterogeneous patient population. In contrast, a recent meta‑analysis by Karedath et al32 reported a numerically greater HbA1c level reduction with subcutaneous semaglutide (standardized MD, 0.21; 95% CI, 0.04–0.38), consistent with our finding that the injectable formulation had an insignificantly stronger effect on HbA1c level reduction (1.4% vs 1.16% for oral formulation). However, their analysis was limited by vague inclusion criteria, reliance on only 4 studies, most of which were retrospective, and the absence of a formal noninferiority assessment.
Since T2D is associated with significant morbidity and mortality, primarily due to its complications, including cardiovascular diseases or diabetic kidney disease, applying a treatment that also affects comorbidities seems to be especially important in managing diabetic patients.33,34 From this perspective, GLP‑1RAs and sodium‑glucose cotransporter‑2 (SGLT‑2) inhibitors emerged as recommended treatment options by the American Diabetes Association (ADA) Standards of Care and the ADA / European Association for the Study of Diabetes.35,36
The DAPA‑CKD (Dapagliflozin and Prevention of Adverse Outcomes in Chronic Kidney Disease) trial37 demonstrated that dapagliflozin significantly reduced the risk of kidney failure, death from cardiovascular causes, and hospitalization for heart failure in patients with chronic kidney disease (CKD), both with and without diabetes.37 A pooled analysis of SUSTAIN 6 and LEADER (Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results) trials indicated that semaglutide and liraglutide significantly reduced albuminuria and slowed the decline in eGFR in patients with T2D, suggesting nephroprotective effects.38 Similar results were observed in a recent FLOW study (A Research Study to See How Semaglutide Works Compared to Placebo in People with Type 2 Diabetes and Chronic Kidney Disease), where semaglutide had renoprotective effects in people without diabetes but suffering from CKD, showing a 24% lower hazard ratio for major kidney disease events, as compared with placebo.39
While both SGLT‑2 and GLP‑1RAs provide nephroprotection, the latter also lead to significant weight loss, which further reduces cardiovascular risk. In terms of weight management, subcutaneous semaglutide was superior, achieving greater weight loss and BMI reduction than the oral form. However, the ORs for achieving at least 5% of initial body weight loss did not differ between the formulations. Subcutaneous semaglutide reduced body weight by on average 5.07 kg, while oral semaglutide showed a weight reduction of 2.88 kg. This observation is further supported by the findings of Shi et al,40 who reported greater weight loss with injectable semaglutide in a comprehensive network meta‑analysis of contemporary T2D treatment. However, for other outcomes, their analysis treated all GLP‑1 RAs as a single group, limiting conclusions specific to semaglutide formulations. Additionally, Formichi et al41 found superior outcomes in weight and BMI reduction, as well as waist circumference, with subcutaneous semaglutide in comparison with the oral form in a retrospective cohort. Yet, significant baseline differences between the groups, such as higher initial body weight and shorter diabetes duration in the subcutaneous group, may have influenced these results. It is worth noting, however, that our study included only trials on the patients with T2D. The analyzed trials rarely reported initial body weight, but we may assume that the majority of patients had normal weight or overweight. In contrast, most trials of the STEP program involved obese or overweight patients without diabetes. Most of the published RCTs with subcutaneous semaglutide were done for weight management purposes. In such a population, the effect of semaglutide was far more pronounced in comparison with a diabetic population.
The OASIS 1 trial42 (Research Study to Investigate How Well Semaglutide Tablets Taken Once Daily Work in People Who Are Overweight or Living With Obesity) evaluated the effects of oral semaglutide 50 mg daily in adults with overweight or obesity without T2D. The study found that semaglutide led to a significant mean body weight reduction of 15.1%, as compared with 2.4% on placebo over 68 weeks. Additionally, 85% of the participants in the semaglutide group and 26% in the placebo group achieved at least 5% weight loss. The STEP 3 trial43 assessed the impact of once‑weekly subcutaneous semaglutide at 2.4 mg combined with intensive behavioral therapy in adults with overweight or obesity. The results showed a mean weight reduction of 16% on semaglutide vs 5.7% on placebo over 68 weeks. Furthermore, 86.6% of the participants on semaglutide achieved at least 5% weight loss, as compared with 47.6% in the placebo group.43 A recent systematic review and meta‑analysis of RCTs, including the STEP trials, confirmed that semaglutide at 2.4 mg once weekly resulted in a mean weight loss of 12.1% relative to placebo, with 33.4% of the participants achieving at least 20% weight loss.44 The SELECT trial45 (Semaglutide Effects on Heart Disease and Stroke in Patients With Overweight or Obesity) also demonstrated long‑term weight loss benefits with semaglutide, showing a mean weight reduction of 10.2% sustained over 208 weeks in patients with obesity and preexisting cardiovascular disease. Higher effectiveness in those trials, however, may arise from higher initial body weight in the studies in the obese / overweight population without T2D, which is a known confounding factor for weight loss.
Discussing the cardiovascular risk, the effect of semaglutide on BP and lipid profile needs to be mentioned. In our analysis, both oral and subcutaneous semaglutide significantly reduced SBP, but neither formulation achieved a clinically significant reduction. In terms of lipid profiles, oral semaglutide significantly lowered total cholesterol, LDL‑C, and triglyceride levels, but these changes were not clinically meaningful. On the other hand, subcutaneous semaglutide significantly reduced triglyceride levels, reaching both clinical and statistical significance, while showing no impact on other lipid parameters. Our results seem to be in line with STEP 1 and STEP 4 trials on obese / overweight patients without diabetes.41 As shown in the meta‑analysis of their results, subcutaneous semaglutide at 2.4 mg once weekly led to reductions in SBP and DBP, as compared with placebo. Specifically, a mean reduction was approximately 4.78 mm Hg for SBP and 2.56 mm Hg for DBP. These reductions varied in different weight loss categories, and were maintained with continued treatment but deteriorated upon discontinuation. Similarly, semaglutide improved the lipid profile, but the results were strongly related to the percentage of weight lost, reaching clinical significance only in the subgroups with the greatest effect (≥15% total weight loss).46
Regarding safety, oral semaglutide seems to be a better‑tolerated formulation. It showed no significant influence on total AE rate but significantly reduced serious AEs and all‑cause mortality in comparison with placebo. Subcutaneous semaglutide, however, increased the number of total AEs but showed no difference in all‑cause mortality and SAEs in comparison with placebo. Nevertheless, it has to be pointed out that for both formulations the total number of death cases was small, and all‑cause mortality reduction on oral semaglutide results from a single study, PIONEER 6.24
Considering the persistent nature of the disease, patient adherence to the therapy is especially important in managing T2D. Thus, patient preferences should also be considered in treatment selection. Clinically, both formulations of semaglutide are comparably effective in glycemic control, with subcutaneous semaglutide offering additional benefits in weight management. Oral semaglutide may be preferred by patients who are averse to injections, potentially improving adherence. However, for those needing stronger weight loss effects, the subcutaneous form may be preferable.41,47 That is why physicians should consider the specific clinical needs of each patient when selecting the appropriate formulation of semaglutide.
Limitations
This analysis has several limitations that should be considered when interpreting the results. First, the included randomized trials varied in follow‑up duration and completeness of secondary outcome reporting (not all trials reported lipid profiles or AE subtypes), which introduced clinical and reporting heterogeneity that constrained some subgroup and sensitivity analyses. Second, the chosen noninferiority margins and the focus on adult populations limit generalizability in pediatric patients, people with severe comorbidities, or those on chronic insulin therapy, who were excluded by our eligibility criteria. Despite these limitations, the systematic methods, robust primary end point, and prespecified analysis plan support the main finding that oral semaglutide provides comparable glycemic control to the subcutaneous form in the studied adult populations.
Conclusions
We found out that both oral and subcutaneous semaglutide offer strong glycemic control, with the injectable form providing additional weight‑loss benefits—an important factor for many patients with T2D. The subcutaneous formulation demonstrates superior efficacy in reducing body weight, BMI, and triglyceride levels, whereas both formulations exert modest beneficial effects on BP and lipid profiles. Consequently, the choice between oral and subcutaneous semaglutide should reflect patient preferences, clinical needs, and likelihood of staying on treatment.
- Tirandi A, Montecucco F, Carbone F, Liberale L. Role of glucagon‑like peptide‑1 receptor agonists in the treatment of obesity, cardiovascular disease, and cerebrovascular disease. Pol Arch Intern Med. 2024; 134: 16658. | Crossref
- Meier JJ. Efficacy of semaglutide in a subcutaneous and an oral formulation. Front Endocrinol (Lausanne). 2021; 12: 645617. | Crossref
- Clements JN, Isaacs D, Hartman RE, Gambill K. Pharmacokinetics and clinical implications of oral semaglutide for type 2 diabetes mellitus. Clin Pharmacokinet. 2021; 60: 153‑163. | Crossref
- Zhong P, Zeng H, Huang M, et al. Efficacy and safety of subcutaneous and oral semaglutide administration in patients with type 2 diabetes: a meta‑analysis. Front Pharmacol. 2021; 12: 695182. | Crossref
- Aroda VR, Erhan U, Jelnes P, et al. Safety and tolerability of semaglutide across the SUSTAIN and PIONEER phase III: a clinical trial programmes. Diabetes Obes Metab. 2023; 25: 1385‑1397. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION