Lower urinary tract symptoms in older adults as a manifestation of underlying geriatric conditions: results of a national population-based study PolSenior2
1 ,
Key words: elderly, geriatric problems, lower urinary tract symptoms, nocturia, urinary incontinence
,
Key words: elderly, geriatric problems, lower urinary tract symptoms, nocturia, urinary incontinence

 CC BY 4.0
CC BY 4.0
Lower urinary tract symptoms in older adults as a manifestation of underlying geriatric conditions: results of a national population-based study PolSenior2
Introduction: Lower urinary tract symptoms (LUTS) are a common problem among older patients in primary and general care.
Objective: We aimed to estimate the prevalence of LUTS and their association with issues related to health status, other geriatric problems, lifestyle factors, and social conditions in a population of Polish citizens aged over 60 years.
Patients and methods: The analysis was part of a national cross‑sectional study PolSenior2, conducted in the years 2018 and 2019 in a cohort of 5698 community‑dwelling older adults. Data on LUTS, health status, and socioeconomic situation were obtained based on a detailed questionnaire, International Prostate Symptom Score (IPSS), Comprehensive Geriatric Assessment, and laboratory analyses.
Results: The prevalence of LUTS in the Polish population aged over 60 years was estimated at 60.5%; it was significantly higher in women (67.8%; 95% CI, 64.3–71.2) than men (50.3%; 95% CI, 47.2–53.5). The most frequent symptom was nocturia (46.7%), followed by stress urinary incontinence (28.7%) and urgency (21.5%). Univariable analysis showed associations between LUTS and age, obesity, reduced functional capacity, mobility problems, a history of falls, depressive symptoms, cognitive dysfunction, multimorbidity, heart failure, diuretic use, and polypharmacy. In a multivariable regression model, age of 75 years or above, obesity, functional disability, falls, depression, cognitive impairment, multimorbidity, and polypharmacy were independently associated with the occurrence of LUTS.
Conclusions: LUTS affect the majority of older adults. They are associated with numerous sociodemographic and health‑related factors, including typical geriatric problems. Therefore, it is recommended that elderly patients who present with LUTS be investigated for other common age‑related conditions and referred to a geriatrician.
What's new?
Lower urinary tract symptoms (LUTS) are prevalent complaints in older age. The most common ones include increased frequency of urination, nocturia, urinary incontinence, and urgency. Often overlooked in a medical interview, these symptoms significantly impair the quality of life in the elderly, and can lead to increased mortality related to falls. Together with frailty, cognitive impairment, falls, and malnutrition, they belong to the spectrum of typical geriatric conditions, and have a significant impact on overall health status and prognosis for elderly patients. The current study demonstrates the prevalence of LUTS in the older Polish population, and presents their associations with other characteristic geriatric conditions, such as falls, disability, dementia, depression, and multimorbidity. The results stress the need for active screening for LUTS in older adults. Once detected, they should prompt the search for other geriatric problems in primary medical care and patient referral for geriatric care.

Introduction
Demographic changes in the global population affect the profile of patients receiving care from specialists in internal medicine and other closely related specialties. The population of older patients has increased, and many of them present with multiple comorbidities and geriatric issues.1,2 Typical geriatric conditions have a substantial impact on the overall health status and prognosis of older patients. However, in routine clinical practice, health care professionals frequently tend to prioritize the management of the leading disease (eg, heart failure [HF], chronic obstructive pulmonary disease, diabetes). At the same time, concomitant geriatric issues remain unnoticed and undertreated.3 This is largely due to fragmentation of the care system, deficits in human and time resources in the health care system, and an inadequate number of geriatricians. Another critical factor is the aforementioned disease‑based approach to care, which is still prevalent in internal medicine specialties, and seems to require change given the increasing number of elderly people with multiple geriatric syndromes and multimorbidity.3-5 The most prevalent geriatric conditions include frailty syndrome, cognitive impairment, falls, malnutrition, functional disability, and lower urinary tract symptoms (LUTS). The prevalence of LUTS in elderly patients is estimated to be as high as 70%, depending on the study population, age, research methodology, the used definition of LUTS, and cultural and ethnic conditions.6,7 LUTS can be categorized into voiding and irritative symptoms, as well as urine storage and urinary tract obstruction.8 The most common ones are increased frequency and urgency of urination, excessive passage of urine at night (nocturia), and urinary incontinence. The presence of LUTS significantly reduces life quality, affecting mood and increasing anxiety, social isolation, sleep disorders, and sexual problems. It also elevates the risk of urinary tract infections, as well as dermatitis, soreness, and bedsores.6,9-11 LUTS have been previously associated with numerous chronic diseases that are prevalent among the elderly (eg, diabetes, chronic kidney disease, HF). It has been estimated that up to 50% of patients with HF present with LUTS.12 Similarly, studies by Papaefstathiou et al13 and Tam et al14 highlighted a high prevalence of LUTS in patients with diabetes mellitus. The severity of these symptoms may also be influenced by various groups of medications commonly prescribed for elderly individuals, including diuretics, sodium‑glucose cotransporter 2 inhibitors, and β-blockers.12,15,16 Several studies have demonstrated a relationship between LUTS and other common geriatric problems.17,18 In routine clinical practice, LUTS are among the more prevalent complaints, and are often indicative of other age‑related health issues that necessitate clinical attention.
This study aimed to estimate the prevalence of LUTS in a Polish population of individuals aged 60 years and above, and to analyze their associations with selected social, geriatric, and lifestyle factors, stratified by sex.
Patients and methods
This analysis is based on the PolSenior2 study, conducted in Poland in the years 2018 and 2019 on 5987 elderly citizens residing throughout the country, with an equal number of women and men in each age category. The research methodology employed a 3‑stage stratified and clustered sampling procedure. The initial stage involved the selection of urban, rural, and urban–rural municipalities (strata) from each of the 16 regions of Poland. The number of respondents was proportional to the population size of the stratum and was based on the population structure. In the subsequent stage of the process, a random selection of villages and cities was made from each stratum. In the final stage, participants were drawn from the population of the previously selected villages and cities using the national registry.
The study was conducted at the participants’ homes by trained nurses. During 3 visits, a detailed medical history and information on the socioeconomic situation were collected, and several tests and scales included in the Comprehensive Geriatric Assessment were applied.19
Data on the occurrence of LUTS were obtained from 98.5% of the study population (women, 51.2%), based on a medical questionnaire. A total of 143 people with chronic urinary bladder catheterization and 580 with significant cognitive impairments (Mini‑Mental State Examination [MMSE] score ≤19 points) were excluded. The final analysis included 5174 individuals.
The medical questionnaire featured 3 questions regarding the occurrence of LUTS: 1) “Do you ever lose urine when exercising, coughing, sneezing, or while performing daily activities?”, which indicated the presence of symptoms related to stress urinary incontinence; 2) “Are there situations in which you have an uncontrollable need to urinate?”, which pertained to the presence of symptoms characteristic of urgency, suggesting the possibility of an overreactive bladder; and 3) “Do you get up at night to go to the toilet at least twice to urinate?”, which indicated a diagnosis of nocturia.
Data analysis
The prevalence of LUTS was assessed against the backdrop of selected socioeconomic factors (sex, age, level of education, a history of physical work, place of residence, self‑assessment of the economic situation, necessity of systematic help), body mass index (BMI), and typical geriatric problems (multimorbidity, polypharmacy, functional disability, mobility problems, depressive symptoms, cognitive impairment, a history of falls). Functional capacity was assessed using 2 scales: Activities of Daily Living (ADL) and Instrumental Activities of Daily Living (IADL).20,21 The participants who obtained 5 or 6 points on the ADL scale were classified as independent, those who scored 3 or 4 points, as partially independent, and the ones with 0 to 2 points, as dependent. On the IADL scale, the ranges were as follows: 24 points corresponded to highly functional individuals, 23 to 19 points, to partially disabled, and 18 or less, to disabled. The respondents reported falls occurring in the last 12 months. The presence of depressive symptoms was assessed using the Geriatric Depression Scale (>5 points).22 Cognitive impairment was identified using the MMSE score after adjustment for age and education level, in accordance with Mungas et al.23,24 Multimorbidity was defined as coexistence of 2 or more chronic comorbidities. Polypharmacy referred to regular intake of at least 5 drugs daily.
In women, a relationship between LUTS and past deliveries was assessed, whereas in men, we evaluated the association of LUTS with treatment of benign prostatic hyperplasia (BPH). The presence and intensity of symptoms associated with BPH were assessed using the International Prostate Symptom Score (IPSS) , with 0–7 points indicating mild, 8–19, moderate, and 20–35, severe and very severe symptoms associated with prostate diseases. A previous diagnosis of BPH was based on the intake of typical medications used for this condition (5α-reductase inhibitors and / or α1 antagonists and / or antimuscarinics).
Ethics
This study was conducted in accordance with the principles outlined in the Declaration of Helsinki. The Independent Bioethics Commission of the Medical University of Gdansk (NKBBN/257/2017) approved the study protocol. Written informed consent was obtained from all participants.
Statistical analysis
Statistical analysis included complex sampling schemes, where multistage sampling was taken into account, and weights for individual respondents were calculated. The poststratification method was used to determine the weights correcting the age and sex structure of the sample to the Polish population. Intergroup differences were tested using the weighted unpaired t test for numeric variables and the weighted χ2 test for categorical data. Both univariable and multivariable logistic regression models were built on unweighted data. Univariable logistic regression analysis was used to assess the relationship between the occurrence of LUTS and the set of risk factors. A multivariable logistic regression model was built using a backward factor selection algorithm and the Bayesian information criterion. Regression results are expressed as odds ratios (ORs) with 95% CIs. Two‑tailed tests were performed at a significance level of P below 0.05. Statistical analysis was performed using the R statistical package (R Core Team, version 3.6.3; the R Foundation for Statistical Computing, Vienna, Austria) and SAS 9.4 (SAS Institute, Inc., Cary, North Carolina, United States).
Results
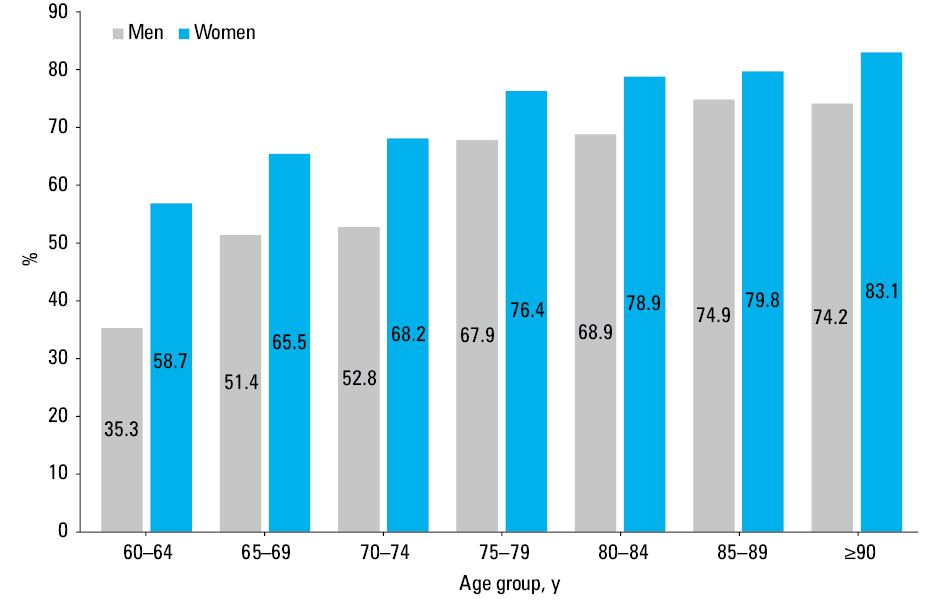
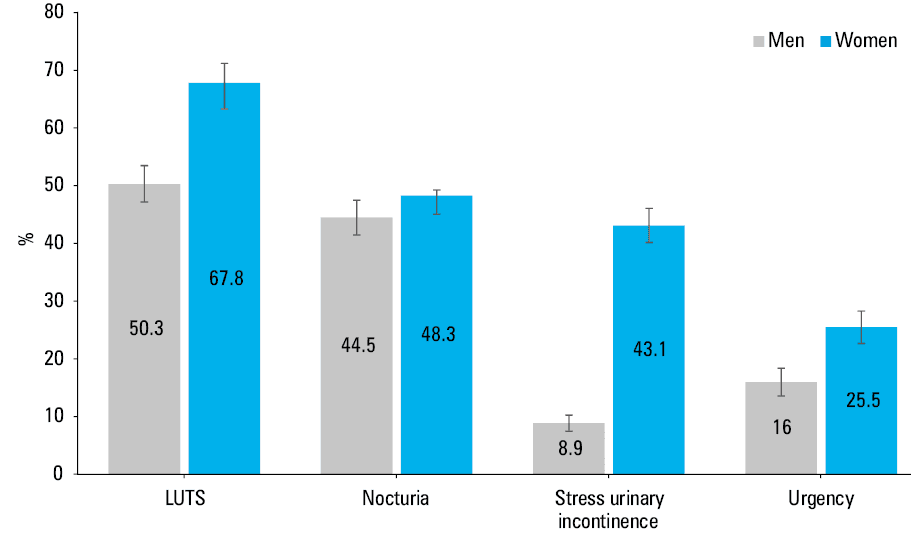
The prevalence of LUTS among Polish citizens aged over 60 years, based on the PolSenior2 study, was estimated at 60.5% (95% CI, 57.7%–63.2%). The symptoms were significantly more frequent among women (67.8%; 95% CI, 64.3%–71.2%) than men (50.3%; 95% CI, 47.2%–53.5%). The prevalence of LUTS in different age groups is illustrated in Figure 1. The most prevalent symptom was nocturia (46.7%), with a similar frequency among women and men. The second most common symptoms were those indicative of stress urinary incontinence (28.7%; 95% CI, 26.9%–30.5%), with women experiencing this issue nearly 5 times more often than men (43.1%; 95% CI, 40.2%–46.1% vs 8.9%; 95% CI, 7.5%–10.3%). The prevalence of urgency was estimated at 21.5% (95% CI, 19.3%–23.7%), with a higher percentage observed in women than men (25.5%; 95% CI, 22.7%–28.3% vs 16%; 95% CI, 13.6%–18.4%, respectively; Figure 2).
Sociodemographic and clinical characteristics of groups with and without symptoms (LUTS‑positive and LUTS‑negative, respectively), stratified by sex, are presented in Table 1.
Characteristics | Women | P value | Men | P value | |||
LUTS (+) | LUTS (–) | LUTS (+) | LUTS (–) | ||||
Results are presented as percentages with 95% CI unless indicated otherwise.
Abbreviations: ADL, activities of daily living; BMI, body mass index; IADL, instrumental activities of daily living, IPSS, international prostate symptom score, MMSE, Mini‑Mental State Examination | |||||||
Age, y, mean (95% CI) | 72 (71.7–72.3) | 69 (68.4–69.5) | <0.001 | 71.3 (70.9–71.7) | 67.5 (67.1–67.8) | <0.001 | |
Age group, y | 60–74 | 64.9 (63.5–66.4) | 79.2 (76.4–82) | <0.001 | 68.8 (66.6–71) | 86.7 (85.2–88.3) | <0.001 |
≥75 | 35.1 (33.6–36.5) | 20.8 (18–23.6) | 31.2 (29–33.4) | 13.3 (11.7–14.8) | |||
BMI, kg/m2 | <25 | 19.4 (16.5–22.3) | 30.2 (24.5–35.8) | <0.001 | 18.4 (15.3–21.5) | 22.6 (19.1–26.1) | 0.04 |
25–30 | 32.7 (29.8–35.7) | 36.9 (33.4–40.5) | 43.9 (40.3–47.5) | 46.4 (42.4–50.5) | |||
>30 | 47.9 (43.6–52.1) | 32.9 (27.6–38.1) | 37.7 (33.6–41.7) | 31 (26.6–35.4) | |||
Place of residence | Rural | 39.3 (30.5–48.1) | 36.1 (28–44.3) | 0.41 | 38.7 (31.3–46.2) | 41.4 (34.4–48.4) | 0.43 |
Urban | 60.7 (51.9–69.5) | 63.9 (55.7–72) | 61.3 (53.8–68.7) | 58.6 (51.6–65.6) | |||
Level of education | Primary or incomplete primary | 30.6 (25.3–35.9) | 20.3 (15.9–24.8) | 0.001 | 21.2 (17.3–25.1) | 16.7 (13.2–20.2) | 0.11 |
Vocational | 18.2 (15.4–21) | 25.5 (19.7–31.2) | 34.1 (30.4–37.8) | 39.8 (35.6–44.1) | |||
Secondary or postsecondary | 37.4 (33.4–41.5) | 40.3 (35.1–45.4) | 30.9 (27.5–34.3) | 29.2 (25–33.3) | |||
Higher | 13.8 (9.5–18.1) | 13.9 (9.7–18.1) | 13.8 (10.6–17.1) | 14.3 (11.6–16.9) | |||
Economic status | Enough for all needs | 15.1 (12.2–18) | 20.6 (15.9–25.3) | 0.03 | 22.4 (18.8–26.1) | 26.4 (21.8–30.9) | 0.22 |
Enough for everyday basic needs | 75.8 (72.8–78.8) | 73 (67.6–78.4) | 71.1 (67.1–75.1) | 68.9 (64.2–73.6) | |||
Not enough for everyday basic needs | 9.1 (7.3–11) | 6.4 (4–8.8) | 6.4 (4.1–8.7) | 4.7 (3–6.4) | |||
History of physical work | 48.2 (42.8–53.6) | 40.9 (34.4–47.4) | 0.052 | 65.9 (61.6–70.2) | 67.8 (62.8–72.7) | 0.56 | |
Physical activity, h/wk | <2.5 | 19.1 (16.5–21.7) | 13 (9.5–16.6) | 0.004 | 20.8 (16.8–24.8) | 15.8 (12.1–19.4) | 0.04 |
≥2.5 | 80.9 (78.3–83.5) | 87 (83.4–90.5) | 79.2 (75.2–83.2) | 84.2 (80.6–87.9) | |||
Necessity of systematic help | 25.1 (22.7–27.4) | 11.5 (8.5–14.6) | <0.001 | 17.5 (14.3–20.7) | 9 (6–12) | <0.001 | |
Need for assistance with mobility | 5.9 (4.6–7.2) | 1.4 (0.7–2.2) | <0.001 | 4.7 (3.2–6.3) | 2.1 (0.8–3.4) | <0.001 | |
Falls | 21.9 (19.1–24.7) | 12.6 (9.6–15.6) | <0.001 | 14.7 (12–17.4) | 5.2 (3.5–6.8) | <0.001 | |
ADL | Independent (5–6 points) | 96.4 (95.3–97.6) | 99 (98.5–99.6) | <0.001 | 97.4 (96.4–98.4) | 98.6 (97.6–99.7) | 0.048 |
Partially dependent (3–4 points) | 2.2 (1.6–2.9) | 0.7 (0.2–1.1) | 2.1 (1.2–3) | 0.7 (0–1.4) | |||
Dependent (0–2 points) | 1.4 (0.6–2.2) | 0.3 (0–0.6) | 0.5 (0.2–0.8) | 0.7 (0–1.5) | |||
IADL | Highly functional (24 points) | 72.9 (70.4–75.3) | 87.6 (84.4–90.7) | <0.001 | 75.3 (72–78.7) | 84.1 (80.6–87.7) | <0.001 |
Partially disabled (23–19 points) | 16.4 (14.4–18.4) | 8.3 (5.5–11.1) | 14.8 (12.1–17.5) | 10.9 (7.8–14) | |||
Disabled (≤18 points) | 10.7 (9.1–12.4) | 4.1 (2.7–5.6) | 9.8 (7.8–11.9) | 5 (3.1–6.8) | |||
Depression | 29.9 (27.3–32.5) | 18.4 (13.9–22.9) | <0.001 | 26 (22.5–29.6) | 10.4 (7.8–13) | <0.001 | |
Mild dementia (MMSE 20–23 points) | 12.6 (10.6–14.7) | 8.5 (6–11.1) | <0.001 | 16 (13.2–18.8) | 7.7 (5.5–9.9) | <0.001 | |
Multimorbidity | 87.3 (85.3–89.3) | 73.7 (67.3–80.1) | <0.001 | 83.2 (80.2–86.3) | 66.7 (61.6–71.7) | <0.001 | |
Heart failure | 13.2 (11.1–15.4) | 8.1 (5.8–10.3) | <0.001 | 22.6 (19.6–25.6) | 11.5 (8.7–14.3) | <0.001 | |
Polypharmacy | 55 (51.5–58.5) | 35.1 (30.6–39.5) | <0.001 | 54.8 (50.9–58.8) | 33 (28.3–37.6) | <0.001 | |
Use of diuretics | 39.1 (36.2–42.1) | 28.1 (24–32.2) | <0.001 | 35.7 (31.9–39.5) | 21.1 (17.5–24.6) | <0.001 | |
Deliveries | 1–2 | 50.1 (45.2–55.1) | 55.3 (50.6–60) | 0.12 | – | – | – |
≥3 | 44.3 (38–50.7) | 38.3 (33.4–43.2) | – | – | – | ||
IPSS scale, points | 0–7 | – | – | 52.1 (48.1–56.1) | 83.8 (80.7–86.9) | <0.001 | |
8–19 | – | – | 33.4 (29.6–37.2) | 13.8 (10.9–16.8) | |||
20–35 | – | – | 14.5 (12.2–16.8) | 2.4 (1–3.8) | |||
Women with lower urinary tract symptoms
The LUTS‑positive women were significantly older than those without LUTS. Among social factors, a significant relationship was found between the occurrence of LUTS and the level of education, but not the type of work (physical work), place of residence (urban or rural), or self‑assessed economic situation. The necessity of systematic help was estimated to occur in over a quarter of the women with LUTS, while among those without LUTS, the rate was only 11.5%. This observation seems to be closely related to the functional status. In terms of complex activities of daily living (the IADL scale), twice as many LUTS‑positive women were disabled, as compared with the LUTS‑negative group. The women with LUTS were 4 times more likely to require mobility assistance, and a significantly higher incidence of falls was found in this group. With respect to other conditions, a considerably higher prevalence of depression, mild dementia, HF, multimorbidity, polypharmacy, diuretics use, and obesity was noted in the LUTS‑positive group. The presence of LUTS was not found to be related to the number of deliveries.
Men with lower urinary tract symptoms
A similar pattern was observed in the men with LUTS, who were also older than those without such symptoms. There were no significant differences between the LUTS‑positive and LUTS‑negative men in terms of education level, type of work, place of residence, or financial situation. There were no significant differences in ADL; however, disability assessed with IADL and the need for assistance were more common in the men reporting LUTS. Additionally, falls were almost 3 times more frequent, whereas depression and cognitive decline were twice as frequent among the men with LUTS, as compared with those without such symptoms. Furthermore, HF, multimorbidity, diuretic use, and polypharmacy were more prevalent in the LUTS‑positive group. A higher proportion of LUTS‑positive men were treated pharmacologically for BPH and presented moderate or severe symptoms related to BPH.
Factors associated with lower urinary tract symptoms in univariable regression analysis
The influence of the numerous abovementioned factors on the risk of LUTS among women was confirmed by univariable regression analysis (Table 2). Age above 75 years, obesity, severe and partial IADL‑assessed disability, need for assistance, multimorbidity, HF, polypharmacy, use of diuretics, and a history of falls were the most significant LUTS correlates. Of the remaining typical geriatric problems, mild dementia and depression also significantly correlated with the presence of LUTS in women.
Parameter | Univariable model | Multivariable model | |||
OR (95% CI) | P value | OR (95% CI) | P value | ||
Abbreviations: see Table 1 | |||||
Age group, y | 60–74 | Ref. | Ref. | ||
≥75 | 2.05 (1.66–2.55) | <0.001 | 1.37 (1.09–1.73) | 0.008 | |
BMI, kg/m2 | <25 | Ref. | Ref. | ||
25–30 | 1.38 (1–1.91) | 0.052 | 1.20 (0.94–1.54) | 0.15 | |
>30 | 2.26 (1.51–3.4) | <0.001 | 2.01 (1.55–2.6) | <0.001 | |
Necessity of systematic help | No / rather no | Ref. | Ref. | ||
Yes / rather yes | 2.57 (1.91–3.46) | <0.001 | 1.56 (1.13–2.18) | 0.008 | |
IADL, points | 24 | Ref. | Ref. | ||
19–23 | 2.37 (1.58–3.56) | <0.001 | 1.43 (1.03–2.01) | 0.04 | |
0–18 | 3.14 (2.17–4.55) | <0.001 | 1.43 (0.86–2.42) | 0.17 | |
Falls | No | Ref. | Ref. | ||
Yes | 1.95 (1.4–2.71) | <0.001 | 1.55 (1.14–1.99) | 0.004 | |
Depression | No | Ref. | Ref. | ||
Yes | 1.89 (1.37–2.61) | <0.001 | 1.54 (1.20–1.98) | 0.001 | |
Cognitive function (MMSE, points) | 27–30 | Ref. | Ref. | ||
24–26 | 1.28 (0.92–1.79) | 0.14 | 0.92 (0.71–1.18) | 0.5 | |
20–23 | 1.63 (1.06–2.52) | <0.001 | 1.53 (1.07–2.23) | 0.02 | |
Multimorbidity | No | Ref. | Ref. | ||
Yes | 2.46 (1.75–3.4) | <0.001 | 1.55 (1.18–2.03) | 0.002 | |
Heart failure | No | Ref. | Ref. | ||
Yes | 1.86 (1.43–2.42) | <0.001 | 0.94 (0.68–1.28) | 0.68 | |
Polypharmacy | No | Ref. | Ref. | ||
Yes | 2.26 (1.77–2.9) | <0.001 | 1.33 (1.05–1.62) | 0.02 | |
Use of diuretics | No | Ref. | Ref. | ||
Yes | 1.71 (1.43–2.04) | <0.001 | 0.98 (0.78–1.23) | 0.88 | |
Among men (Table 3) there was also a significant relationship between the occurrence of LUTS and the presence of cognitive impairment, HF, use of diuretics, as well as the severity of symptoms associated with BPH (IPSS scores >19 points increased the risk of LUTS almost 10‑fold) and typical pharmacological BPH treatment. The risk of LUTS was found to be 2‑fold lower in men than in women (OR, 0.48; 95% CI, 0.41–0.57).
Parameter | Univariable model | Multivariable model | |||
OR (95% CI) | P value | OR (95% CI) | P value | ||
Abbreviations: see Table 1 | |||||
Age group, y | 60–74 | Ref. | Ref. | ||
≥75 | 2.92 (2.37–3.69) | <0.001 | 1.7 (1.38–2.09) | <0.001 | |
BMI, kg/m2 | <25 | Ref. | Ref. | ||
25–30 | 1.16 (0.89–1.52) | 0.27 | 1.31 (1.02–1.69) | 0.03 | |
>30 | 1.49 (1.05–2.11) | 0.03 | 1.55 (1.18–2.03) | 0.002 | |
Necessity of systematic help | No / rather no | Ref. | Ref. | ||
Yes / rather yes | 2.15 (1.45–3.19) | <0.001 | 0.69 (0.65–1.27) | 0.56 | |
IADL, points | 24 | Ref. | Ref. | ||
19–23 | 1.52 (1.07–2.16) | 0.02 | 0.88 (0.66–1.17) | 0.38 | |
0–18 | 2.22 (1.44–3.42) | 0.001 | 0.88 (0.56–1.36) | 0.56 | |
Falls | No | Ref. | Ref. | ||
Yes | 3.16 (2.13–4.68) | <0.001 | 1.48 (1.07–2.06) | 0.02 | |
Depression | No | Ref. | Ref. | ||
Yes | 3.02 (2.11–4.33) | <0.001 | 1.4 (1.08–1.82) | 0.01 | |
Cognitive function (MMSE, points) | 27–30 | Ref. | Ref. | ||
24–26 | 1.55 (1.15–2.1) | 0.005 | 1.1 (0.85–1.41) | 0.47 | |
20–23 | 2.48 (1.62–3.8) | <0.001 | 1.4 (1.01–1.95) | 0.046 | |
Multimorbidity | No | Ref. | Ref. | ||
Yes | 2.48 (1.85–3.33) | <0.001 | 1.6 (1.24–2.08) | <0.001 | |
Heart failure | No | Ref. | Ref. | ||
Yes | 2.16 (1.75–2.67) | <0.001 | 1.11 (0.85–1.45) | 0.44 | |
Polypharmacy | No | Ref. | Ref. | ||
Yes | 2.47 (1.85–3.3) | <0.001 | 1.34 (1.08–1.67) | 0.008 | |
Use of diuretics | No | Ref. | Ref. | ||
Yes | 1.97 (1.66–2.35) | <0.001 | 1.2 (0.95–1.52) | 0.13 | |
IPSS, points | 0–7 | Ref. | Ref. | ||
8–19 | 3.88 (2.84–5.29) | <0.001 | 3.29 (2.6–4.17) | <0.001 | |
20–35 | 9.87 (5.27–18.46) | <0.001 | 6.51 (4.2–10.48) | <0.001 | |
Use of α1 antagonists and / or 5α-reductase inhibitors | No | Ref. | Ref. | ||
Yes | 2.45 (1.88–3.2) | <0.001 | 1.38 (1.09–1.73) | 0.007 | |
Factors associated with lower urinary tract symptom in multivariable regression analysis
Among the factors significantly impacting the occurrence of LUTS in women, the following were identified (Table 2): age equal to or greater than 75 years, obesity, partial disability assessed using the IADL scale, necessity of systematic help, falls, presence of depressive symptoms, mild dementia, multimorbidity, and polypharmacy.
In men (Table 3), among the typical geriatric problems, a history of falls, depressive symptoms, mild dementia, multimorbidity, and polypharmacy were identified as significant factors associated with LUTS presence. Furthermore, LUTS were found to correlate with the severity of symptoms associated with BPH and the need for pharmacological treatment. Additionally, older age (≥75 y), overweight, and obesity were identified as significant factors contributing to LUTS incidence.
Discussion
LUTS are a significant and recognized problem in the health care of older people.9,17 In this study, we demonstrated their prevalence in a representative population‑based cohort of individuals aged 60 years and older, living in Poland. We showed that LUTS affect most older adults, with a higher prevalence in women. Additionally, we identified the principal risk factors and parameters associated with the occurrence of LUTS. The value of our study is enhanced by the fact that there was an overrepresentation of very old individuals and men in the study group relative to the demographic structure, resulting in greater data accuracy for these specific subgroups.
Our study is consistent with previous research conducted in other countries. In a large EPIC study, including over 19 000 adults from 5 countries, 3300 participants were over 60 years old. In this age group, LUTS occurred in 62.5% of men and 58.7% of women, when nocturia was defined as 2 or more episodes per night of waking up to urinate.25 In a Polish study including individuals aged over 40 years, the frequency of LUTS increased with age in both sexes, and ranged from 50.4% to 69.8%, with a higher prevalence in women than men, up to the age of 80 years, when the proportion reversed.26,27 The most common symptoms were associated with urine storage, and nocturia was the dominant one. The prevalence of LUTS in this survey was higher than in the PolSenior2 study, despite the study group being younger. In our opinion, this is due to differences in methodology. In our research, questions concerning LUTS offered only a dichotomous answer (yes / no), and there were only 3 such questions. The methodology of the study by Przydacz et al26 was based on a Likert scale. This may have resulted in LUTS presence being recorded even when the severity of the symptoms was not very high. LUTS were also frequently reported in another epidemiological study conducted among patients aged 40 years and older who self‑referred to primary care physicians in Belgium for any reason. Among men, urgency and incontinence were reported by 63% and 32%, respectively, of the participants at the age of 60 to 69 years; in the older groups, this percentage exceeded 70% for urgency and 50% for incontinence. Nocturia was reported by 2% of younger seniors, and its prevalence increased with age, exceeding 61% among men aged 80 years and over.28 Among women, nocturia was the most frequent symptom, with prevalence ranging from 71.5% among younger seniors to almost 80% among those older than 80 years. In contrast, more than 60% of older women experienced stress urinary incontinence (42.5% of women aged 60–69 y and more than 56% of those over 80 y).29 Not all data are consistent with those described above. As pointed out by Coyne et al,6 differences stem from the study population, its age, methodology, data collection methods, the LUTS definition, and cultural and ethnic conditions.
Age is one of the most important risk factors for LUTS, as reported before.9,18,30 The PolSenior2 study confirmed that advanced age is a risk factor for the occurrence of LUTS. Another significant risk factor for LUTS in our research was female sex, which has been previously demonstrated to impact the prevalence and perception of LUTS. In a study by Apostolidis et al,31 involving 415 hospitalized patients over 18 years of age from 13 departments of a general hospital, it was found that women tended to report the presence of LUTS later, when more troublesome symptoms occured (with LUTS prevalence of 85.5% in women vs 75.2% in men; P = 0.01). This is one of the reasons why studies on LUTS are often conducted separately for both sexes, and this assumption was also adopted in our study, where the factors coexisting with LUTS were separately analyzed.
Among other sociodemographic factors, a significant relationship between LUTS presence and a low level of education was demonstrated only in women. Among men, none of the sociodemographic factors (level of education, physical work, place of residence, or economic status) was found to be significant. In a study by Smith et al,30 which included over 100 000 men with moderate‑to‑severe LUTS, a low level of education correlated with the severity of symptoms. In a Brazilian questionnaire study examining the frequency of urinary incontinence among individuals over 60 years old, a low level of education was associated with the frequency of urinary incontinence in both sexes.32 Similarly, in a large cohort comprising over 8000 respondents from China, Korea, and Taiwan, of whom 34% were over 60 years of age, a low level of education was associated with a higher frequency of overactive bladder.33 The causes of these relationships are difficult to determine. They may be related to worse general health status in many societies, particularly among those with lower education levels, but this has not been evaluated in the present study.
Our study showed that among the individuals reporting LUTS in the Polish population, those with a lower level of functional ability significantly prevailed. Among men, this issue concerned only advanced activities of daily living, whereas among women, it also concerned the basic ones. Interestingly, in the multivariable analysis, LUTS were only associated with poorer IADL performance in both sexes. Presumably, when asked about basic activities (ADL scale), the interviewees reported better performance, indicating they were not willing to be considered disabled. Furthermore, in the ADL scale, the question regarding urinary (and bowel) control could have been interpreted as being too explicit and not considering the varying intensity of LUTS. After all, many individuals presenting with these symptoms belive they are generally in control of their urination, so they would find a negative answer discriminatory against them.
In comparison with the LUTS‑negative women, the women with LUTS more often had mobility problems and declared the need for help, while falls were more frequent in the LUTS‑positive patients of both sexes. The relationship between the occurrence of LUTS and typical geriatric syndromes, such as falls or disability, was also demonstrated in other studies.34 As indicated by Gibson et al,35 the significant relationship between falls and the occurrence of LUTS is, at least partly, due to low levels of physical activity and deterioration of physical and functional fitness. Elderly individuals with urinary incontinence not only face urgency and the need to reach the toilet quickly, which can lead to falls, but also limit their physical activity. This reduction in physical activity can decrease their physical capacity, thereby increasing their risk of falling. In our study, a lower level of physical activity was also observed in the women with LUTS.
Cognitive impairment, especially deterioration of executive functions, also contributes to the association between LUTS and the risk of falls. The increased risk of falls in patients with LUTS results from the involvement of areas of the brain responsible for both central control of urination perception and urethral sphincter control, as well as many components of executive functions that have a significant impact on gait control and efficient movement. Similarly, cognitive impairment, particularly dementia, contributes to LUTS through several mechanisms, including the function of the central, autonomic, and peripheral nervous systems.36 In addition, among individuals with LUTS, central nervous system imaging shows degenerative changes in the white matter and cerebral microcirculation,37 and these symptoms may occur already at the early stage of dementia, somehow preceding significant cognitive deficits.38 In the PolSenior2 cohort, the participants who reported LUTS were more likely to have cognitive dysfunction. A similar association was found for depressive disorders, both in the PolSenior2 and other studies.30 A review of studies on the occurrence of LUTS in patients with depression and anxiety showed that these conditions negatively affect the experience, development, and persistence of LUTS, and that LUTS play a vital role in the onset of depression and anxiety therapy.39 Other important geriatric issues are multimorbidity with associated polypharmacy, which have been shown to increase the risk of LUTS.40 Such relationships have also been observed in the present study and other similarly designed studies conducted in various regions worldwide.41
Among chronic diseases, we analyzed HF due to its specific relationship with LUTS. As noted before,12,42 LUTS (particularly nocturia, urinary incontinence, urgency, and frequent urination) are reported by 35%–50% of patients with HF. There are several factors contributing to this association, including the impact of medications used in HF treatment (primarily diuretics), increased levels of endogenous natriuretic peptides, which also promote diuresis, as well as the mobilization of edema during night‑time rest in a horizontal position. Further factors that can contribute to LUTS in individuals with HF include comorbidities, such as diabetes and chronic kidney disease, as well as chronic ischemia in the lower pelvic organs (including the bladder) resulting from atherosclerosis, a condition that is also frequently the cause of HF. In our study, we observed a higher incidence of HF and diuretic use in the LUTS‑positive group. However, multivariable regression analysis did not show a direct relationship.
Among women, an additional potential risk factor for stress urinary incontinence is the weakening of the pelvic diaphragm after numerous pregnancies and childbirths, and during menopause.43 The Boston Area Community Health (BACH) survey of over 2500 women also showed that the risk of LUTS increased with the number of deliveries.44 An increase was already observed with a history of 2 or more vaginal deliveries. In our analysis, such a relationship was not demonstrated. However, our study population included only older women, in whom the symptoms were rather triggered by other factors, while three‑quarters of the women included in the BACH study were under 60 years old.
BPH is an important risk factor for LUTS in men, which is confirmed in other studies.45 In the PolSenior2 study, declarations regarding prior diagnosis of BPH were not obtained. However, among the LUTS‑positive men there were significantly more users of α1 antagonists or 5α-reductase inhibitors, drugs almost exclusively prescribed for symptomatic BPH.
Finally, obesity has to be mentioned as another recognized risk factor for LUTS.9 Obesity has been shown to increase the incidence of nocturia in both sexes, as well as to elevate the risk of stress and urge urinary incontinence in women and urinary frequency in men.46 A meta‑analysis of 12 studies showed that both increased BMI and waist circumference were associated with LUTS.47 In the Polish population, based on the PolSenior2 results, the association between obesity and LUTS was also observed in both sexes. In men, overweight was also a risk factor. It has to be stressed that the usefulness and accuracy of BMI in diagnosing obesity in the older population raises some doubts due to a shift in body composition associated with advancing age, among other factors.
Limitations
Our study has several limitations. The questions used in the PolSenior2 survey to diagnose LUTS were not a structured diagnostic tool for LUTS and lacked detail. There were 2 reasons for using such methodology. Firstly, at the time of developing the survey for the PolSenior2 study, there were not many validated diagnostic scales available. Secondly, the objective of identifying as many geriatric problems as possible using a lengthy and complex questionnaire was compromised, as the respondents’ ability to participate in a long interview was limited. Another limitation was a lack of information on past endourological procedures for the prostatic gland and bladder (transurethral resection of bladder tumor or prostate) and urogenital surgery, which could be a cause for LUTS development.
Conclusions
LUTS are a prevalent clinical problem affecting older individuals, often accompanying other characteristic geriatric conditions, such as depression, dementia, disability, falls, and multimorbidity. Consequently, their presence may serve as an indication to actively screen for other geriatric problems in daily medical practice and refer the patient for geriatric care.
- Nobili A, Garattini S, Mannucci PM. Multiple diseases and polypharmacy in the elderly: challenges for the internist of the third millennium. J Comorb. 2011; 1: 28‑44. | Crossref
- Chlebus K, Zdrojewski T, Jagiełło K, et al. Prevalence of hypercholesterolemia in the elderly and very elderly members of the Polish population: results of a national cross‑sectional representative survey. Pol Arch Intern Med. 2024; 134: 16882. | Crossref
- Mannucci PM, Nobili A. Internal and geriatric medicine: an alliance for the challenges of the elderly. Eur J Intern Med. 2012; 23: 479‑482. | Crossref
- Maroto IV, Romano PC, Nogueroles MM et al. Recommendations on the comprehensive, multidimensional assessment of hospitalized elderly people. Position of the Spanish Society of Internal Medicine. Rev Clín Esp (Barc). 2021; 221: 347‑358. | Crossref
- Gómez‑Huelgas R, Dalekos GN, Dicker D, et al. Internal medicine in the 21st century: back to the future. Eur J Intern Med. 2024; 128: 26‑29. | Crossref
ARTICLE INFORMATION