Granulomatous mycosis fungoides transformation in a patient with systemic lupus erythematosus

 CC BY 4.0
CC BY 4.0
Granulomatous mycosis fungoides transformation in a patient with systemic lupus erythematosus
Patients with atopic dermatitis (AD) are at an increased risk of developing autoimmune diseases, including systemic lupus erythematosus (SLE).1 SLE can lead to the development of malignant tumors, including B‑cell lymphomas.2 Cutaneous T‑cell lymphomas, such as mycosis fungoides (MF), are extremely rare in patients with SLE.3
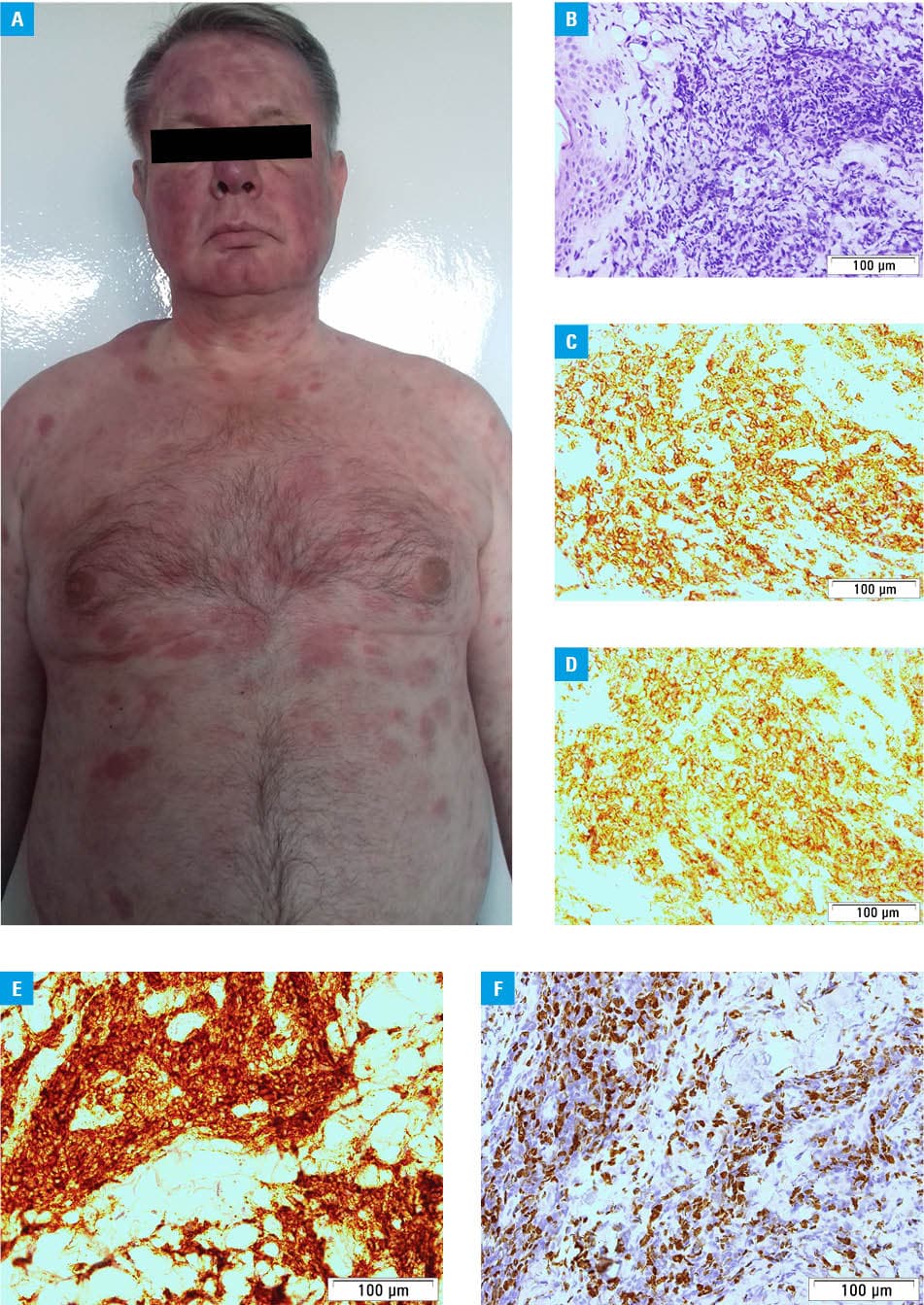
A 58‑year‑old patient with a long‑standing history of AD presented with nodular, erythematous, and edematous skin lesions on his face in April 2017. SLE was diagnosed based on the clinical presentation, positive antinuclear and anti‑double‑stranded DNA (anti‑dsDNA) antibody results, leukopenia (leukocytes, 1.6 × 10⁹/l; reference range [RR], 4–11 × 109/l), and the presence of fluorescent immunoglobulin G / immunoglobulin M deposits at the skin‑epidermis border. However, the levels of the complement components C3 (98 mg/dl; RR, 90–180 mg/dl) and C4 (15 mg/dl; RR, 10–40 mg/dl) were normal. Prednisone was administered at an initial daily dose of 40 mg, which was gradually reduced to 10 mg, leading to clinical remission. However, an attempt to discontinue prednisone therapy resulted in the recurrence of skin lesions. In March 2019, generalized erythematous–edematous skin lesions recurred on the patient’s face, trunk, and limbs (Figure 1A). Repeated laboratory diagnostics confirmed the presence of antinuclear antibody (1:100) and leukopenia (leukocytes, 3.8 × 10⁹/l; RR, 4–11 × 109/l), but absence of anti‑dsDNA (46.8 IU/ml; RR <100 IU/ml) and the fact that skin lesions were independent of ultraviolet (UV) radiation exposure were confusing. Skin biopsy performed again in October 2019 showed epidermal infiltrates composed mainly of T lymphocytes (CD3+, CD4+, CD5+, CD7–/+, CD8–/+, CD30–) and a few B lymphocytes (CD20+), with a Ki67 proliferation index of almost 100% (Figure 1B–1F). Cutaneous nodular lymphoma at the stage of MF was diagnosed. Pegylated interferon α-2a, methotrexate, and radiotherapy were employed, resulting in a temporary disease remission. In April 2020, the patient’s skin lesions progressed, and he reported fever and night sweats. Abdominal computed tomography (CT) showed hepatosplenomegaly and lymphadenopathy, while fluorine‑18 fluorodeoxyglucose positron emission tomography / CT identified numerous active lesions in the skin, muscles, bones, lungs, lymph nodes, and sigmoid colon. Biopsy of the tumor in the left shoulder blade area showed CD30+ clone expansion, confirming progression of the disease to an aggressive, infiltrative form of granulomatous MF. The patient was treated with an anti‑CD30 monoclonal antibody brentuximab, chemotherapy comprising gemcitabine, liposomal doxorubicin, and methylprednisolone, followed by a further cyclophosphamide, doxorubicin, vincristine, and prednisone regimen, and local brachytherapy of the tumor in the left eyelid. Unfortunately, the treatment was ineffective. The lymphoma lesions progressed, and numerous adverse effects were documented in laboratory tests, including transient agranulocytosis, acute kidney injury, and opportunistic bacterial superinfections. The patient died in May 2021.
Very few patients with SLE and MF have been described.4 In its early stages, MF may resemble SLE, as it exhibits similar skin symptoms, such as erythematous plaques. In SLE, however, they are associated with UV exposure. In early MF, macular lesions are mainly located in areas not exposed to UV radiation.5 Moreover, early MF may be histologically subtle and overlap with inflammatory dermatoses, including SLE. In advanced MF, these dermatoses form erythematous–edematous tumors associated with lymphoid cell infiltration,5 and may subsequently involve lymph nodes and internal organs.5 Clinicians caring for AD patients should be aware of the increased risk of developing autoimmune diseases and necessary follow‑up for malignancies. Biopsy should be performed in patients with SLE, who have persistent or atypical skin lesions, especially if they are not responding to standard therapy, or if there has been a change in morphology (eg, nodules or ulceration).6 This procedure may sometimes need to be repeated.
- Ponvilawan B, Charoenngam N, Wongtrakul W, et al. Association of atopic dermatitis with an increased risk of systemic lupus erythematosus: a systematic review and meta‑analysis. J Postgrad Med. 2021; 67: 139‑145. | Crossref
- Clarke AE, Pooley N, Marjenberg Z, et al. Risk of malignancy in patients with systemic lupus erythematosus: systematic review and meta‑analysis. Semin Arthritis Rheum. 2021; 51: 1230‑1241. | Crossref
- Klein A, Polliack A, Gafter‑Gvili A. Systemic lupus erythematosus and lymphoma: incidence, pathogenesis and biology. Leuk Res. 2018; 75: 45‑49. | Crossref
- Vieyra‑Garcia PA, Cerroni L, Clark RA, Wolf P. Lupus erythematosus tumidus in a patient with mycosis fungoides stage IB after complete response to PUVA. J Eur Acad Dermatol Venereol. 2021; 35: e758‑e760. | Crossref
- Willemze R, Kerl H, Sterry W, et al. EORTC classification for primary cutaneous lymphomas: a proposal from the Cutaneous Lymphoma Study Group of the European Organization for Research and Treatment of Cancer. Blood. 1997; 90: 354‑371. | Crossref
ARTICLE INFORMATION