Pickering syndrome and unilateral renal artery stenosis in a patient with a solitary viable kidney

 CC BY 4.0
CC BY 4.0
Pickering syndrome and unilateral renal artery stenosis in a patient with a solitary viable kidney
In their study published in 1988, Pickering et al1 described a group of patients with recurrent pulmonary edema and hypertension due to renal artery stenosis treated with renal revascularization. Hypertension was accompanied by impaired kidney function in most patients. According to the 2024 European Society of Cardiology guidelines,2 renal artery angioplasty and stenting may be considered (class IIb recommendations) in patients with hemodynamically significant, atherosclerotic renal artery stenosis with: recurrent heart failure or sudden‑onset flash pulmonary edema, unstable angina, resistant hypertension, hypertension with unexplained unilaterally small kidney or chronic kidney disease (CKD), bilateral renal artery stenosis, or unilateral renal artery stenosis in a solitary viable kidney.
A 61‑year‑old woman was admitted due to resistant hypertension and deterioration of kidney excretory function with a serum creatinine level of 4.02 mg/dl (reference range [RR], 0.55–1.02 mg/dl) and estimated glomerular filtration rate (eGFR), calculated using the Chronic Kidney Disease Epidemiology Collaboration formula, of 11.6 ml/min/1.73 m2 (RR >90/ml/min/1.73 m2). The patient’s medical history included hypertension, hyperlipidemia, smoking, coronary atherosclerotic disease treated with percutaneous coronary interventions with stent implantation, heart failure with mildly reduced ejection fraction (EF; 40%), episodes of pulmonary edema with high blood pressure, peripheral arterial disease treated with angioplasty of the right superficial femoral and right popliteal arteries, and stage G4 CKD. Moreover, acute kidney injury (AKI) was observed after starting angiotensin‑converting enzyme inhibitor (ACEI) therapy. Abdominal ultrasound showed asymmetry of the kidneys with a small right kidney (78 mm × 30 mm) and a normal‑sized left kidney (105 mm × 49 mm). As the clinical presentation was characteristic of renovascular hypertension and Pickering syndrome, contrast‑enhanced computed tomography angiography (CTA) was offered to the patient during previous hospitalizations in another center. The first time, it was postponed due to fear of deterioration of kidney function, and on the second occasion, the patient did not consent to the procedure.
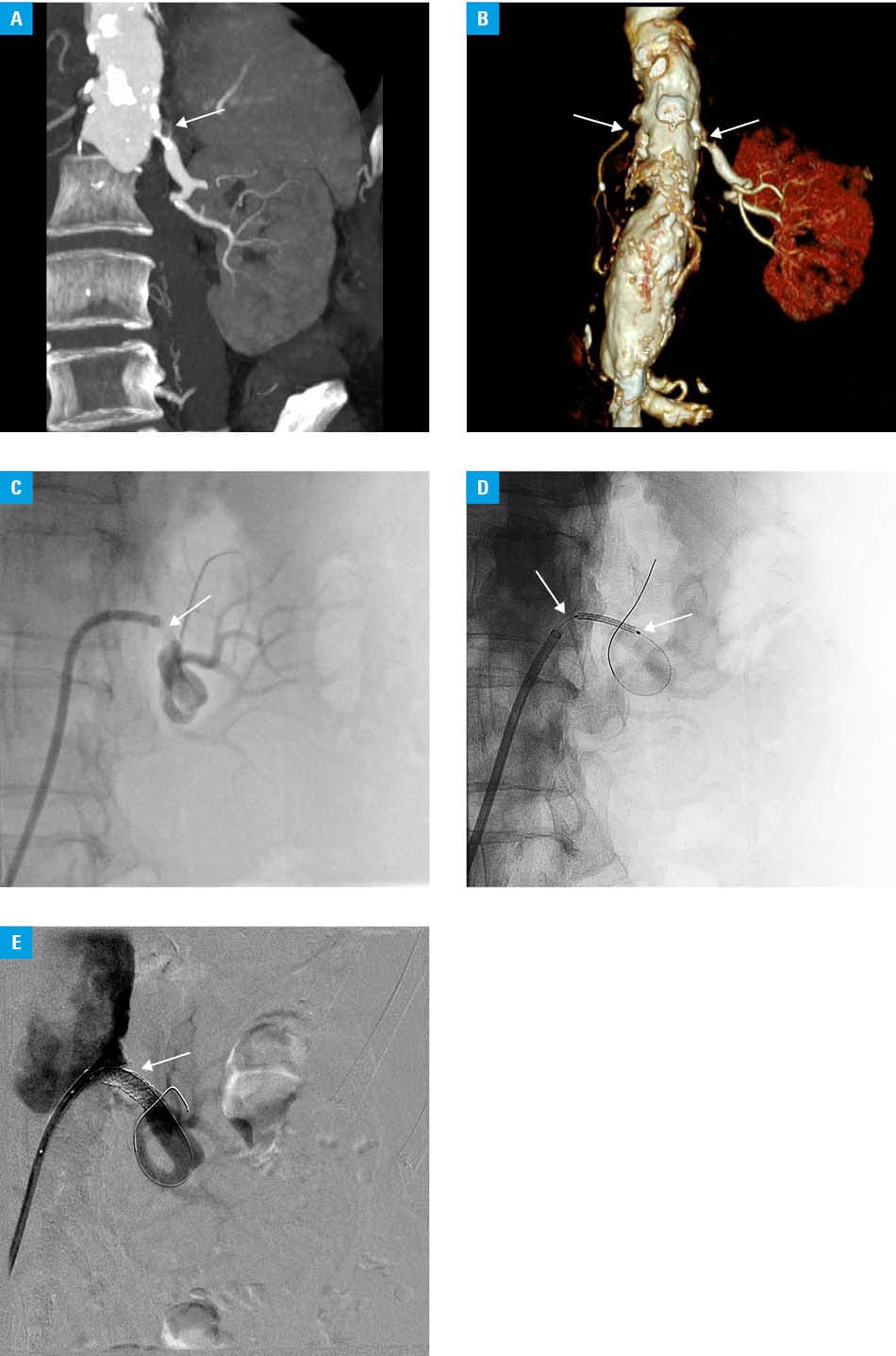
During current hospitalization, the patient gave her consent for contrast‑enhanced CTA, which showed abdominal aorta aneurysm, critical stenosis of the celiac trunk, occlusion of the right renal artery, critical atherosclerotic stenosis of the left renal artery, and areas of low contrast enhancement of the left kidney cortex, related to ischemia (Figure 1A and 1B). Five days later, renal artery stenting was performed. Dual antiplatelet therapy (DAPT) with aspirin and clopidogrel was initiated before the procedure. Initial arteriography demonstrated critical stenosis of the left renal artery (Figure 1C). Using a right femoral 6‑F access with a dedicated bent renal sheath, the stenotic area was navigated with a 2.4‑F microcatheter and a 0.014‑inch microwire. A balloon‑mounted bare metal stent measuring 6 mm × 18 mm (Express SD, Boston Scientific, Maple Grove, Minnesota) was placed (Figure 1D) and deployed at 12 bar pressure. Final angiography demonstrated an optimal result with no residual stenosis and patent peripheral branches (Figure 1E). At discharge, 4 days later, the patient’s creatinine concentration decreased to 1.38 mg/dl (eGFR, 41.4 ml/min/1.73 m2). Due to improved blood pressure control, blood pressure–lowering pharmacological treatment was reduced. Four months later, the patient’s serum creatinine concentration was 1.53 mg/dl (eGFR, 36.3 ml/min/1.73 m2). At that time, ACEI was added to the treatment. No deterioration of kidney excretory function was observed after the next 3 months, with the serum creatinine level of 1.32 mg/dl (eGFR, 43.4 ml/min/1.73 m2). Follow‑up echocardiography showed improvement in left ventricular systolic function (EF, 53%). Long‑term DAPT was continued.
In patients presenting with high‑risk atherosclerotic renovascular disease phenotypes, such as resistant hypertension, recurrent pulmonary edema, heart failure, and deterioration of kidney function, renal artery stenting is associated with renal and cardiovascular benefits.3 Diagnosis and treatment of renal artery stenosis require intravascular contrast media (ICM)-enhanced imaging. Based on unjustified historical conviction, the use of ICM was limited in patients with impaired kidney function due to fear of ICM nephrotoxicity; however, recent data suggest that prevalence and severity of postcontrast AKI were overestimated.4,5 In every case, the benefits of ICM use should be weighed against potential risks. This case report confirmed that patients with characteristic clinical presentation of Pickering syndrome may benefit from kidney revascularization.
- Pickering TG, Herman L, Devereux RB, et al. Recurrent pulmonary edema in hypertension due to bilateral renal artery stenosis: treatment by angioplasty or surgical revascularization. Lancet. 1988; 8610: 551‑552. | Crossref
- McEvoy JW, McCarthy CP, Bruno RM, et al. 2024 ESC Guidelines for the management of elevated blood pressure and hypertension. Eur Heart J. 2024; 45: 3912‑4018. | Crossref
- Mancia G, Kreutz R, Brunstöm M, et al. 2023 ESH Guidelines for the management of arterial hypertension. The Task Force for the management of arterial hypertension of the European Society of Hypertension. J Hypertens. 2023; 41: 1875‑2071. | Crossref
- Chmielewski M, Serafin Z, Kamińska D, et al. The use of intravascular contrast media in patients with impaired kidney function ‑ joint clinical practice position statement of the Polish Society of Nephrology and the Polish Medical Society of Radiology. Pol J Radiol. 2024; 89: e161‑e171. | Crossref
- Chomicka I, Kwiatkowska M, Leśniak A, et al. Post‑contrast acute kidney injury in patients with various stages of chronic kidney disease ‑ is fear justified? Toxins. 2021; 13: 395. | Crossref
ARTICLE INFORMATION