Echinococcosis is a zoonotic infection with the larval stage of Echinococcus tapeworms. There are 2 forms of echinococcosis (also called hydatid disease): cystic echinococcosis (CE) and alveolar echinococcosis (AE).1 AE, less common than CE, is caused by E. multilocularis. Infection occurs through oral ingestion of products contaminated with fox feces containing parasite eggs.
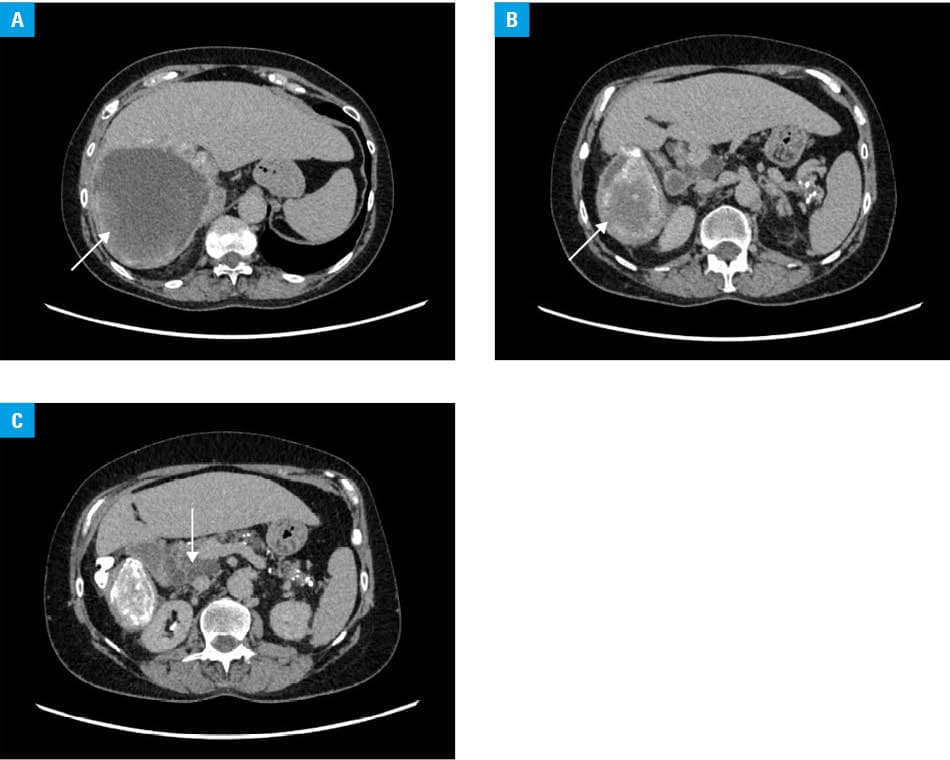
We present a rare case of a patient with primary extrahepatic AE located in the right adrenal gland and the pancreatic head. A 60‑year‑old woman was admitted to a hospital for further diagnostics of a tumor in the right adrenal gland, with the largest diameter of 18 cm (Figure 1A and 1B). On computed tomography (CT) and magnetic resonance imaging, the lesion was described as a predominantly fluid mass with a thick, calcified wall, infiltrating the liver, hepatic veins, and the portal vein. A multicystic lesion of 10 cm in diameter was also observed in the pancreatic head (Figure 1C). Chest CT showed multiple focal lung lesions diagnosed as disseminated echinococcosis.
Adrenal biopsy results gave rise to a suspicion of an echinococcal disease. Immunoglobulin G tests confirmed E. multilocularis infection. Albendazole was prescribed, and ceftriaxone and metronidazole were added temporarily after the biopsy due to a clinical suspicion of later unconfirmed adrenal abscess. The patient was disqualified from surgical intervention and continues treatment with albendazole in a department of infectious diseases.
AE is a rare disease with hydatid cysts most often found in the liver and lungs, while their location in the adrenal gland is extremely unlikely (0.05% of the cases).2,3 It is still unknown how the oncospheres reach this organ. A possible way may be direct dissemination through the blood and lymphatic system to the adrenal gland. Considering that in every described case, the hydatid cysts were localized in the right adrenal gland, an invasion of the larvae directly from the liver seems more likely. Pancreatic AE is even rarer, with approximately 10 cases described so far.4 Clinical manifestations of pancreatic AE are highly variable, often mimicking extensive malignant diseases.
AE has no pathognomonic clinical signs, and its diagnosis requires imaging and laboratory tests. Serological enzyme‑linked immunosorbent assays for the EgHF, EgP, Em2, Em2+, or EmVF antigens are a method of choice, often followed by a confirmatory western blot test. In the case of ambiguous results, a histopathologic examination or detection of parasite‑specific DNA using a polymerase chain reaction test on biopsy material may also be performed.5
The ultimate goal of AE treatment is total eradication of parasitic lesions, achieved when all germinative cells are eliminated. However, due to the absence of highly effective and fast‑acting medications against E. multilocularis, lesion resection is one of the available treatment choices, particularly in the case of pseudotumor progression. Surgical procedures should be undertaken with curative intent.6 Apart from surgery, currently recommended systemic treatment includes benzimidazoles (preferably albendazole and mebendazole). The duration of pharmacotherapy depends on the completeness of surgical removal, that is, 2 years in the case of radical lesion resection, and lifelong in all other cases.6
- Huang M, Zheng H. Primary alveolar echinococcosis (Echinococcus multilocularis) of the adrenal gland: report of two cases. Int J Infect Dis. 2013; 17: e653‑e655. | Crossref
- Akhan O, Canyigit M, Kaya D, et al. Long‑term follow‑up of the percutaneous treatment of hydatid cyst in the adrenal gland: a case report and review of the literature. Cardiovasc Intervent Radiol. 2011; 34: S256‑S259. | Crossref
- Wilk-Śledziewska K, Śledziewski R, Piotrowska W, et al. Unraveling the enigma: Echinococcus multilocularis in the adrenal gland as a very rare cause of hypertension in a young patient. Pol Arch Intern Med. 2024; 134: 16839. | Crossref
- Zhou RX, Hu HJ, Ma WJ, et al. Alveolar echinococcosis in the head of pancreas: a case report. Medicine (Baltimore). 2018; 97: e0072. | Crossref
- Autier B, Gottstein B, Millon L, et al. Alveolar echinococcosis in immunocompromised hosts. Clin Microbiol Infect. 2023; 29: 593‑599. | Crossref
ARTICLE INFORMATION