Coexistence of sarcoidosis and Sjögren syndrome (SS) represents a rare but clinically relevant diagnostic challenge. Sarcoidosis, once considered an exclusion criterion for SS, may in fact coexist with it. Oral manifestations can serve as the first sign of systemic involvement. Awareness of this overlap is crucial for both internists and dental practitioners, as severe xerostomia or salivary gland swelling in patients with sarcoidosis may warrant an evaluation for SS.1-3
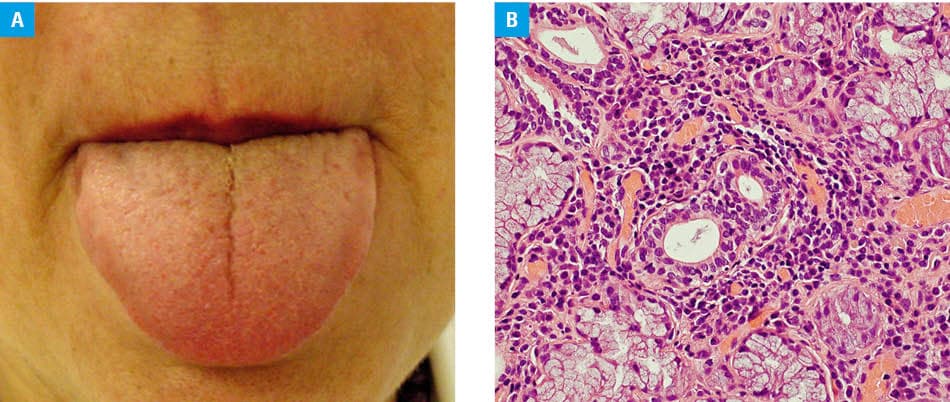
A 65‑year‑old woman with a 5‑year history of pulmonary sarcoidosis presented to the Department of Periodontology of the University Dental Clinic in Kraków with progressive xerostomia, oral burning sensations, halitosis, and occasional difficulty swallowing (Figure 1A). She also reported recent worsening of eye dryness. Clinical examination showed dry, atrophic oral mucosa and multiple cervical carious lesions (score 6 on the Challacombe scale; unstimulated salivary flow <0.05 ml/min; reference range [RR], 0.3–0.4 ml/min).
Previous laboratory tests showed normal levels of C‑reactive protein (1 mg/l; RR <3 mg/l) and serum calcium (2.31 mmol/l; RR, 2.2–2.55 mmol/l), and no evidence of hepatitis B, hepatitis C, or HIV infection. The patient did not have immunoglobulin G4–related disease. Computed tomography of the chest demonstrated regression of previous micronodular lesions, with only residual 2‑mm nodules, consistent with inactive sarcoidosis.
Despite disease stability, the persistence and progression of xerostomia and ocular dryness prompted reassessment for SS. Serologic testing showed antinuclear antibody positivity (1:160; granular pattern), and the tests for antineutrophil cytoplasmic antibodies were negative. Repeat testing demonstrated anti‑Ro/SS–related antigen A antibody positivity. Minor salivary gland biopsy showed focal lymphocytic sialadenitis with 6 foci (focus score >1) and no granulomatous inflammation (Figure 1B).
According to the 2016 American College of Rheumatology and European Alliance of Associations for Rheumatology classification criteria1 (focus score ≥1, anti‑Ro positivity, and unstimulated salivary flow <0.1 ml/min), a diagnosis of primary SS was established in addition to sarcoidosis. The patient received symptomatic treatment with saliva substitutes and dental care, resulting in improved oral comfort at 6‑month follow‑up.
This case highlights that sarcoidosis and SS can coexist despite earlier views regarding their mutual exclusion. The key diagnostic step was the reassessment prompted by severe xerostomia in a patient with otherwise stable sarcoidosis. The case underscores the diagnostic value of oral examination and biopsy findings, as well as the importance of a multidisciplinary approach involving dental, rheumatology, ophtalmology, and pulmonary specialists. Recognition of anti‑Ro seroconversion and biopsy‑proven focal lymphocytic sialadenitis enabled accurate classification and appropriate management.4,5
Such coexisting conditions emphasize the need for vigilance when sicca symptoms persist, even in patients with known systemic disorders. Sarcoidosis and SS can coexist, and a thourough examination of the oral cavity is crucial in detecting such overlapping diseases.
- Shiboski CH, Shiboski SC, Seror R, et al. 2016 American College of Rheumatology / European League Against Rheumatism classification criteria for primary Sjögren’s syndrome. Ann Rheum Dis. 2017; 76: 9‑16. | Crossref
- Ramos‑Casals M, Brito‑Zeron P, Garcia‑Carrasco M, Font J. Sarcoidosis or Sjögren syndrome? Clues to defining mimicry or coexistence in 59 cases. Medicine (Baltimore). 2004; 83: 85‑95. | Crossref
- Flores‑Chavez A, Ng WF, Alunno A, et al. Characterisation of the coexistence between sarcoidosis and Sjögren’s syndrome. Analysis of 43 patients. Clin Exp Rheumatol. 2022; 40: 2329‑2337. | Crossref
- Tokuyasu H, Harada T, Touge H, et al. Primary Sjögren’s syndrome complicated by sarcoidosis. Intern Med. 2008; 47: 2049‑2052. | Crossref
- Li X, Wu J, Ruan G, Chen YC. Multisystem sarcoidosis combined with Sjögren’s syndrome: a case report and literature review. Curr Med Imaging. 2023; 19: 1599‑1603. | Crossref
ARTICLE INFORMATION