Hybrid extraction of a dislodged Abbott Aveir leadless pacemaker from the left pulmonary artery

 CC BY 4.0
CC BY 4.0
Hybrid extraction of a dislodged Abbott Aveir leadless pacemaker from the left pulmonary artery
A 79‑year‑old woman with a history of aortic valve replacement, diabetes, chronic kidney disease (glomerular filtration rate, 28 ml/min/1.73 m2; reference range [RR] ≥60 ml/min/1.73 m2), and atrial fibrillation presented with heart failure decompensation caused by high‑degree atrioventricular blocks. Her left ventricular ejection fraction was 45% (RR ≥54%). Due to a high risk of infection, she was referred for a leadless pacemaker implantation following compensation. The Aveir VR device (Abbott Laboratories, Abbott Park, Illinois, United States) was implanted from the right femoral vein. After mapping various locations of the interventricular septum, the Aveir VR device was implanted in its mid‑apical segment. Once its stability was tested in acute setting, optimal sensing (9.2 mV during pace‑mapping; 7.5 mV postprocedurally; RR >5 mV), and impedance (410 Ω during pace‑mapping; 430 Ω postprocedurally; RR, 200–1500 Ω), with relatively high pacing thresholds (3.75 V at 1.5 ms during pace‑mapping; 3 V at 1.5 ms postprocedurally; Figure 1A), were observed. As noted, impedance remained relatively stable from mapping to deployment, and after implantation.1
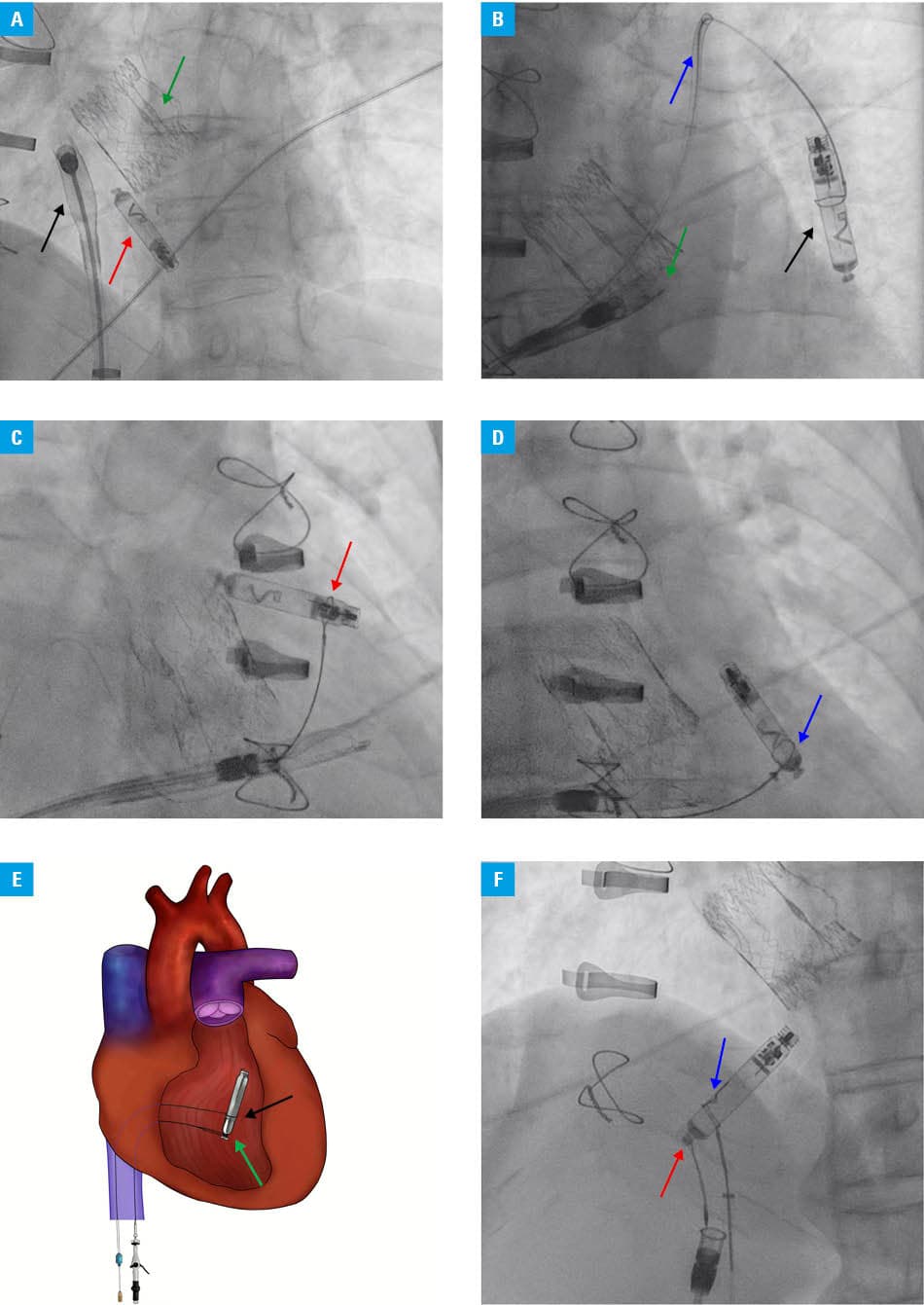
Within 24 hours, electrocardiography and interview showed no capture, and chest X‑ray confirmed device embolization into the left pulmonary artery. On the next day, retrieval was attempted. An Abbott Aveir retrieval tool sheath was introduced via left femoral venous access into the right ventricle (RV), although due to already complex anatomical curvature, it was impossible to advance it any further.2,3 Thus, a 90‑cm long Cordis 7F sheath (Cordis Corporation, Miami Lakes, Florida, United States) was introduced from the right femoral vein to the pulmonary artery, with pulmonary angiography confirming the device lodged in the lower lobar artery. A 20‑mm Goose Neck snare (Medtronic, Minneapolis, Minnesota, United States) was navigated into the left pulmonary artery (Figure 1B). Two failed attempts were made to snare the device close to the fixation helix and retract it through the pulmonary valve (Figure 1C). Ultimately, the device moved with bloodstream into the pulmonary artery, where it was in an optimal position to be captured near the docking button. Eventually, it was grasped with the snare just below the button and successfully withdrawn to the RV (Figure 1D). Numerous attempts to stabilize the device and transfer it to the retrieval system were unsuccessful due to the RV anatomy, and thus, the system was further retrieved and positioned stably in the inferior vena cava, where the docking button was secured, with the retrieval system and the device extracted without complications (Figure 1E and 1F). Subsequently, a transvenous system was implanted, and the patient was safely discharged.
Leadless pacemakers open a new era of pacing, as they allow to substantially reduce the risk of device‑related infections and lead‑related complications. They are magnetic resonance imaging‑conditional devices, and evidence supports their safety in the radiation therapy environment.4 However, their management involves new challenges, including a need for thorough diagnostics postimplantation to detect any complications. Currently, there are 2 such systems available on the market, Micra (Medtronic) and Aveir VR, with the latter being slightly longer and thinner, which allows for its embolization into more distal pulmonary branches.5 Even though a dedicated Aveir VR retrieval tool is available, it may be impossible to advance it further than to the RV. Therefore, potential adjunct tools, such as the Goose Neck snare, seem necessary for a successful retrieval from the pulmonary arteries. It should also be emphasized that the lack of an increase in impedance from mapping to final release of the device, particularly when accompanied by a relatively high pacing threshold, may indicate suboptimal or unstable position of the device and suggest the need for its repositioning.
- Neuzil P, Hubbard C, Doshi RN, et al. Implantation techniques for a helix‑fixation dual‑chamber leadless pacemaker. Heart Rhythm. 2024; 21: 2552‑2562. | Crossref
- Tajstra M, Dyrbuś M, Kurek A, Gąsior M. Micra leadless pacemaker extraction using Aveir retrieval catheter‑initial experience in Poland. Pol Heart J. 2025; 83: 926‑928. | Crossref
- Neuzil P, Exner DV, Knops RE, et al. Worldwide chronic retrieval experience of helix‑fixation leadless cardiac pacemakers. J Am Coll Cardiol. 2025; 85: 1111‑1120. | Crossref
- Dyrbuś M, Machowicz J, Błachut A, et al. Radiation therapy in the presence of non‑transvenous cardiac implantable electronic devices: a case series. Pol Heart J. 2025 Sept 3. [Epub ahead of print] | Crossref
- Sterliński M, Boczar K, Ząbek A, et al. Single‑chamber leadless pacemaker Aveir VR implantation: pioneer experience in Poland. Insights and preliminary report from a multicenter national registry. Pol Heart J. 2024; 82: 791‑793. | Crossref
ARTICLE INFORMATION