Infective endocarditis in a patient with a cardiac implantable electrical device and a dialysis catheter: difficulties in differential diagnosis

 CC BY 4.0
CC BY 4.0
Infective endocarditis in a patient with a cardiac implantable electrical device and a dialysis catheter: difficulties in differential diagnosis
A 43‑year‑old man undergoing dialysis was admitted to a hospital due to fever and chills. His medical history included several cardiological interventions: surgical closure of a ventricular septal defect (June 1984), implantation of a cardiac resynchronization therapy device device due to cardiomyopathy after myocarditis (March 2018), implantation of a biological tricuspid valve (November 2018), and percutaneous closure of the left atrial appendage (April 2019). Laboratory tests showed elevated inflammatory markers—C‑reactive protein at 88 mg/l, (reference range [RR] <5 mg/l) and procalcitonin at 1.47 ng/ml (RR <0.5 ng/ml)—and no leukocytosis (white blood cells, 8.26 × 10³/μl; RR, 4–10 × 10³/μl), although with neutrophil predominance (73%). Microbiological tests showed growth of Staphylococcus epidermidis in 2 venous blood cultures and 1 culture from the dialysis catheter. Empirical antibiotic therapy was initiated with vancomycin and piperacillin / tazobactam.
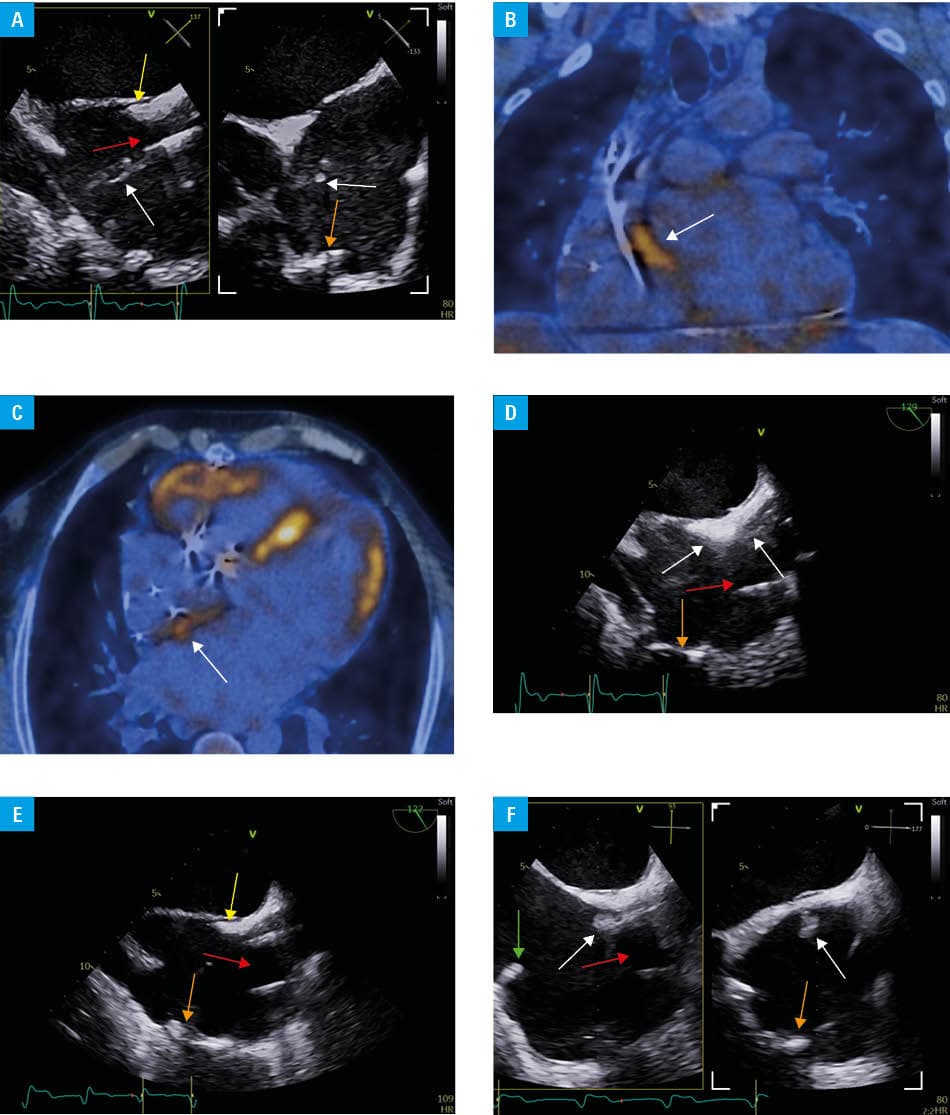
Based on echocardiographic findings, the differential diagnosis included infective endocarditis (IE) or fibrous tissue dislodged during a recent dialysis catheter replacement, which had been performed due to catheter dysfunction (Figure 1A). Given the diagnostic uncertainty, the critical importance of confirming IE, 18F‑fluorodeoxyglucose positron emission tomography / computed tomography (18F‑FDG‑PET/CT) was performed (Figure 1B and 1C). Antibiotic therapy was subsequently modified to vancomycin, gentamicin, and rifampicin. The dialysis catheter was removed. The results of echocardiography and PET, in the context of clinical findings, supported the diagnosis of IE with involvement of the atrial septum near the ostium of the superior vena cava (Figure 1D). No increased metabolic activity was observed on the intracardiac leads. The patient fulfilled 2 major and 2 minor Duke criteria according to the 2023 European Society of Cardiology guidelines1 for the management of IE: positive imaging and blood cultures (major criteria) and a predisposing heart condition and fever (minor criteria). Over the course of 6 weeks of antibiotic therapy, a marked decrease in inflammatory markers and regression of previously described lesions were observed (Figure 1E). However, follow‑up assessment performed 3 months later demonstrated recurrence of abnormal echogenic structures in the same location, likely due to premature reimplantation of the dialysis catheter into the subclavian vein (Figure 1F). The patient declined another hospital admission and was treated with oral rifampicin and vancomycin administered on dialysis days. At 1‑year follow‑up, no echocardiographic or laboratory signs of IE were observed.
This case illustrates the course of IE in a patient with a cardiac implantable electronic device (CIED), dialysis catheter, and prior structural cardiac interventions. The diagnostic process required a multimodal approach, including advanced imaging and nuclear techniques. 18F‑FDG‑PET/CT is particularly valuable in diagnosing IE in patients with mechanical heart implants and CIEDs in the absence of local pocket infections, as demonstrated in this case.2 In patients with confirmed CIED‑related IE, device extraction is recommended.3 In our case, conservative (pharmacological) management was pursued, as transvenous extraction was not possible, the risk associated with open‑heart surgery was very high (Euroscore II, 25%), and metabolic activity on the intracardiac leads on PET was not increased. The most common pathogens causing CIED‑related infections are coagulase‑negative staphylococci and S. aureus.4 Vancomycin is recommended as part of the initial empirical therapy.5
- Delgado V, Ajmone Marsan N, de Waha S, et al. 2023 ESC Guidelines for the management of endocarditis. Eur Heart J. 2023; 44: 3948‑4042. | Crossref
- Wang TKM, Sánchez‑Nadales A, Igbinomwanhia E, et al. Diagnosis of infective endocarditis by subtype using 18F‑fluorodeoxyglucose positron emission tomography / computed tomography: a contemporary meta‑analysis. Circ Cardiovasc Imaging. 2020; 13: e010600. | Crossref
- Le KY, Sohail MR, Friedman PA, et al. Impact of timing of device removal on mortality in patients with cardiovascular implantable electronic device infections. Heart Rhythm. 2011; 8: 1678‑1685. | Crossref
- Hussein AA, Baghdy Y, Wazni OM, et al. Microbiology of cardiac implantable electronic device infections. JACC Clin Electrophysiol. 2016; 2: 498‑505. | Crossref
- Blomström‑Lundqvist C, Traykov V, Erba PA, et al. European Heart Rhythm Association (EHRA) international consensus document on how to prevent, diagnose, and treat cardiac implantable electronic device infections‑endorsed by the Heart Rhythm Society (HRS), the Asia Pacific Heart Rhythm Society (APHRS), the Latin American Heart Rhythm Society (LAHRS), International Society for Cardiovascular Infectious Diseases (ISCVID) and the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) in collaboration with the European Association for Cardio‑Thoracic Surgery (EACTS). Europace. 2020; 22: 515‑549. | Crossref
ARTICLE INFORMATION