Novel transseptal approach for percutaneous closure of a postsurgical ventricular septal defect

 CC BY 4.0
CC BY 4.0
Novel transseptal approach for percutaneous closure of a postsurgical ventricular septal defect
A 52‑year‑old man was admitted to our center for the first episode of heart failure (HF). He had a history of mechanical aortic valve (AoV) implantation performed 13 years prior, subsequent Bentall procedure with bioprosthetic AoV replacement (Freestyle 29 mm; Medtronic, Minneapolis, Minnesota, United States), and coronary artery bypass grafting performed 2 months earlier because of AoV degeneration. The patient also had leadless pacemaker implanted postoperatively due to complete atrioventricular block.
Two weeks prior to admission, the patient started experiencing progressive decline in functional capacity, with New York Heart Association class III dyspnea on admission. On examination, a loud systolic murmur, mild peripheral edema, and pulmonary crackles were noted. Laboratory test results showed elevated levels of N‑terminal pro–B‑type natriuretic peptide (9546.9 pg/ml; reference range [RR], 0–125 pg/ml) and serum creatinine (1.56 mg/dl; RR, 0.73–1.18 mg/dl). Transthoracic echocardiography demonstrated a dilated left ventricle (LV) with regional wall motion abnormalities but preserved global systolic function. The right ventricle (RV) was enlarged with reduced systolic function (tricuspid annular plane systolic excursion, 17 mm). Severe tricuspid regurgitation and moderate‑to‑severe mitral regurgitation were observed, while the bioprosthetic AoV functioned normally. A systolic–diastolic left‑to‑right shunt with a 5‑mm color jet was detected in the subaortic region, directed toward the tricuspid valve—suggestive of a postsurgical ventricular septal defect (VSD; Figure 1A–1C).1 Cardiac computed tomography confirmed a defect measuring 11 mm × 10 mm in the membranous septum. Transesophageal echocardiography confirmed moderate mitral and tricuspid regurgitation. Standard HF therapy was initiated, resulting in clinical stabilization.
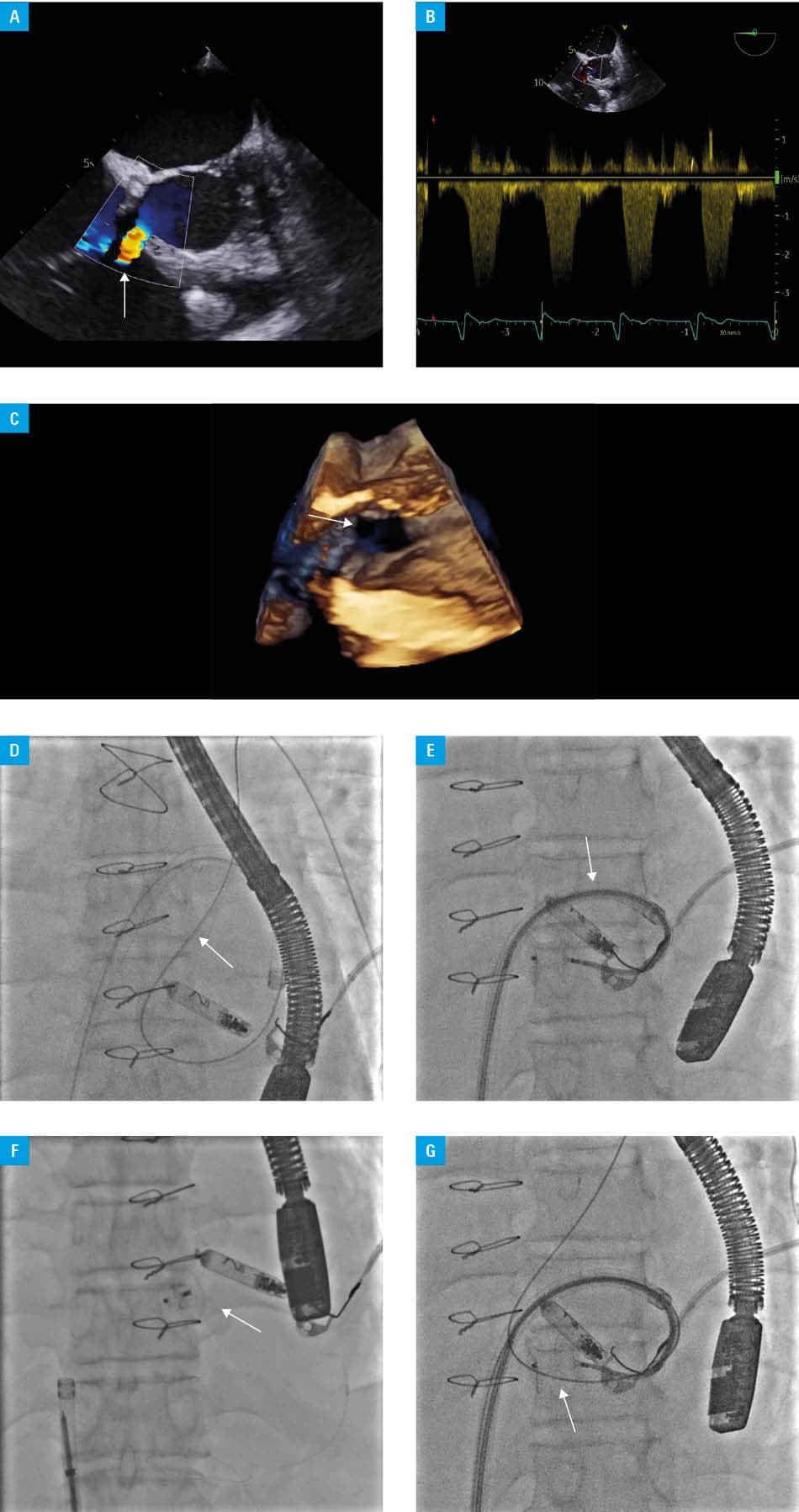
The heart team recommended urgent percutaneous closure due to RV enlargement and evidence of systolic dysfunction. Given the atypical VSD location, a modified interventional approach was required. Transseptal puncture of the interatrial septum was performed via right femoral venous access. A 13F Faradrive steerable sheath (91 cm; Boston Scientific, Marlborough, Massachusetts, United States) was advanced. Using a pigtail catheter (5F; Boston Scientific) with a hydrophilic guidewire, the mitral valve and the VSD were crossed. The hydrophilic wire was exchanged for a stiff wire, which was advanced into the pulmonary artery. A 7F delivery sheath (Amplatzer TorqVue 45 °, 120 cm; Abbott, Abbott Park, Illinois, United States) was introduced over the stiff wire, with a second (“buddy”) wire placed in parallel. A 12‑mm Amplatzer Muscular VSD Occluder (Abbott) was deployed: the first disc was released in the RV and gently retracted against the interventricular septum, whereas the second disc was deployed in the LV (Figure 1D–1G).2 After confirming stable positioning, the buddy wire was removed, and the occluder was released. Follow‑up echocardiography confirmed optimal device placement with a small residual left‑to‑right shunt. Occluder contact with the tricuspid septal leaflet was noted, as expected due to the subaortic VSD location, but only mild‑to‑moderate tricuspid regurgitation was observed. The patient underwent rehabilitation with good clinical improvement, and was discharged in a stable condition 5 days later.
This case illustrates a novel technique for percutaneous VSD closure in complex, postsurgical anatomy. A similar approach with different procedural elements has been previously described.4 The use of transseptal atrial access proved feasible and enabled full sheath steerability, facilitating successful device deployment. Our center has performed 2 such procedures within the past year, demonstrating the value of this modified approach in select challenging cases.
- Abdelmohsen GA, Gabel HA, Al‑Ata JA, et al. Percutaneous closure of postoperative residual ventricular septal defects, including dehiscence of surgical patches. Cardiovasc Diagn Ther. 2023; 13: 710‑727. | Crossref
- Szkutnik M, Kusa J, Białkowski J. Percutaneous closure of post‑traumatic and congenital muscular ventricular septal defects with the Amplatzer Muscular VSD Occluder. Kardiol Pol. 2008; 66: 715‑720.
- Klein AJ, Garcia JA, Carroll JD. Percutaneous closure of an iatrogenic ventricular septal defect following mechanical aortic valve replacement using the transseptal technique. Catheter Cardiovasc Interv. 2007; 70: 1018‑1024. | Crossref
- Yap J, Chen S, Stripe BR, et al. Transseptal access for left heart structural interventions in the setting of prior atrial septal defect closure. Catheter Cardiovasc Interv. 2020; 95: 414‑419. | Crossref
ARTICLE INFORMATION