Temporal trends in homocysteine level measurements at a tertiary cardiovascular center in the years 2016–2024: prevalence of hyperhomocysteinemia and homocystinuria

 CC BY 4.0
CC BY 4.0
Temporal trends in homocysteine level measurements at a tertiary cardiovascular center in the years 2016–2024: prevalence of hyperhomocysteinemia and homocystinuria
Introduction
Homocysteine (Hcy), a noncoded, sulfur‑containing amino acid derived from methionine, is primarily obtained from dietary animal proteins.1,2 In 1969, Kilmer McCully postulated that elevated total Hcy (tHcy) concentrations led to premature atherosclerosis.2 Although plasma tHcy levels above 15 µmol/l have been shown to be associated with an increased risk of coronary artery disease (CAD) through mechanisms such as impaired endothelial function, oxidative stress, and a prothrombotic state,2 the Hcy‑based theory of atherosclerosis has lost significance over the past 2 decades.
Hyperhomocysteinemia (HHcy), defined as plasma tHcy concentrations greater than 15 µmol/l, is determined by both genetic variants and acquired factors, including renal diseases (eg, chronic kidney disease3), thyroid disorders,4 and nutritional factors, such as vitamin B deficiencies or a high‑protein diet.5 Based on tHcy levels, the spectrum of HHcy ranges from mild (15–30 µmol/l) to severe (>100 µmol/l).6 Elevated tHcy levels have been observed in patients with venous thromboembolism (VTE)7; however, current guidelines do not recommend its measurement as part of routine thrombophilia screening.8
Homocystinuria, characterized by tHcy levels above 100 µmol/l, is a rare autosomal recessive metabolic disorder mostly caused by mutations in the cystathionine β-synthase (CBS) gene, with a prevalence of 1–9 per 100 000 individuals.2,9 It typically presents early in life with multisystem involvement, including lens dislocation, marfanoid skeletal abnormalities, neurologic impairments, early‑onset atherosclerotic vascular disease, and an increased risk of arterial thrombosis (particularly ischemic stroke) and VTE events.9 Without timely diagnosis and treatment, patients face severe complications. However, the exact proportion of homocystynuric individuals diagnosed in adulthood remains unknown, and the disease appears to be markedly underdiagnosed, often leading to suboptimal management.10
Randomized trials investigating the effect of tHcy‑lowering therapies (mainly vitamin B12 and folate supplementation) on cardiovascular risk have yielded inconsistent or negative results. This was observed despite an approximate 25% reduction in tHcy levels, although individuals with a markedly elevated tHcy concentration were underrepresented in that study.11 Recent guidelines on cardiovascular disease prevention do not recommend tHcy‑lowering interventions, but emphasize the importance of diagnosing and treating nutritional deficiencies, particularly in patients with severe HHcy.12 Consequently, the clinical relevance of tHcy testing has declined in most centers, whereas lipoprotein(a) (Lp[a]) has gained increasing attention, largely due to ongoing Lp(a)-lowering trials.13,14
We tested a hypothesis that requests for tHcy level measurement in cardiovascular centers are declining and may be largely unnecessary, particularly among older individuals, given the rarity of homocystynuria. Therefore, we analyzed temporal trends in the frequency of all such requests with respect to clinical indications and the proportion of patients diagnosed with HHcy, especially homocystynuria.
Patients and methods
We retrospectively analyzed all tHcy measurements performed in inpatients and outpatients at the St. John Paul II Hospital in Kraków, Poland, between January 2016 and December 2024. The hospital is a 576‑bed tertiary referral center providing continuous 24/7 diagnostic and therapeutic services, with 26 clinical departments primarily specializing in cardiology, cardiac and vascular surgery, pulmonology, and thoracic surgery. In 2023, the institution reported 149 152 admissions, including 29 460 hospitalizations and 119 692 outpatient visits.
Clinical categories were assigned according to documented diagnoses based on the International Classification of Diseases, 10th Revision codes, focusing on CAD, VTE, cerebrovascular events, and peripheral artery disease (PAD). tHcy level measurements performed for scientific reasons were excluded.
Patients were asked to remain fasting for at least 8 hours prior to blood sampling. Plasma tHcy levels were determined using an enzymatic assay (Homocysteine Enzymatic Assay, Roche Diagnostics, Mannheim, Germany).
At the discretion of the attending physician, testing for the common MTHFR C677T gene variant was performed. Genotyping was carried out using a TaqMan single‑nucleotide polymorphism assay (Applied Biosystems, ThermoFisher Scientific, Foster City, California, United States; rs1801133) on a QuantStudio Dx Real‑Time PCR instrument (ThermoFisher Scientific). Since 2019, in selected patients, a CBS gene analysis has also been requested to confirm a genetic cause of homocystinuria.
All patients provided written informed consent to participate. As this study was part of routine clinical workup, approval of a Bioethical Committee was not required.
Statistical analysis
Continuous variables were reported as mean with SD or median with interquartile range (IQR), as appropriate, while categorical data were presented as counts and percentages. The Shapiro–Wilk test was applied to assess the normality of distributions. For 2‑group comparisons, the Mann–Whitney test was used. Categorical variables were analyzed using the χ2 test. Correlations were evaluated using Spearman coefficients. Comparisons across more than 2 groups were performed using the Kruskal–Wallis test. A P value below 0.05 was considered significant. All analyses were conducted using Python (version 3.10.12; Python Software Foundation, Wilmington, Delaware, United States) with libraries including pandas, numpy, and scipy for statistical testing.
Results
During the study period, a total of 10 055 tHcy level measurements were performed in 9269 patients (4681 women; 50.5%) at a median (IQR) age of 54 (41–68) years. Most patients were tested only once (n = 8670; 93.5%). Repeated measurements were less common: 478 patients (5.2%) underwent 2 tests, 90 (1%) underwent 3 tests, and 15 (0.2%) had 4 measurements performed. Higher numbers of repeated assessments were rare, with 9 individuals having 5 measurements performed, 3 having 6 tests, 2 undergoing 7 tests, and 1 patient each with 10 and 12 measurements.
As shown in Figure 1A, the number of measurements increased 6‑fold in 2024, as compared with 2016 (P <0.001). In 2020, during the COVID‑19 pandemic, the number of tests declined by 17%, as compared with 2019, and remained lower in 2021. After 2021, the frequency of tHcy testing increased again, exceeding the prepandemic levels in subsequent years.
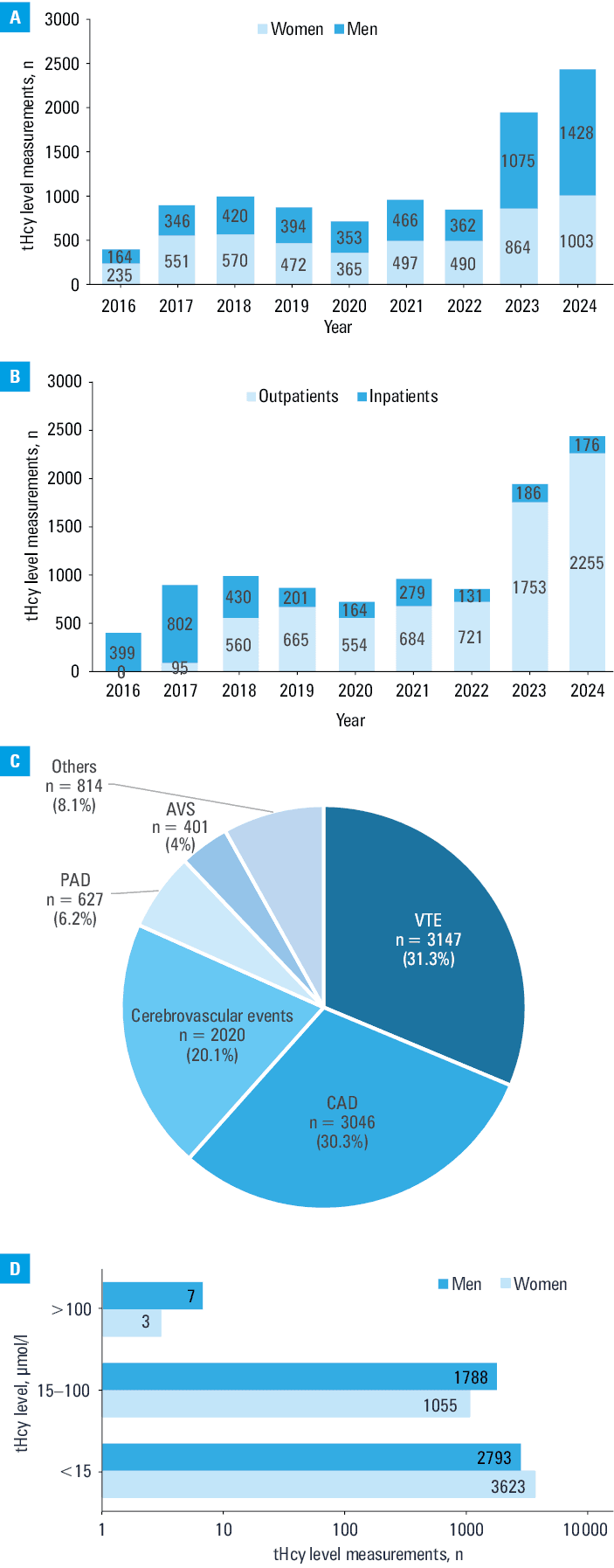
Abbreviations: AVS, aortic valve stenosis; CAD, coronary artery disease; PAD, peripheral artery disease; VTE, venous thromboembolism
The overall median (IQR) age of patients undergoing tHcy testing rose markedly during the study period from 48 (36–61) years in 2016 to 65 (54–75) years in 2024 (P = 0.007). Women were younger than men (median [IQR], 50 [38–66] vs 59 [46–69] y; P <0.001). The most common age groups were 39–54 years (28.7%) and 54–69 years (29.6%).
Of all tHcy level measurements, 7287 (72.5%) were performed in outpatients (median [IQR] age, 56 [43–68] y) and 2768 (27.5%) in hospitalized patients (median [IQR] age, 51 [39–64] y; Figure 1B). Women were more frequently tested between 2017 and 2022, both in the outpatient and inpatient settings, whereas men predominated in the years 2023 and 2024. A majority of outpatient tHcy requests originated from cardiology clinics (6858 tests; 94.1%).
The distribution of clinical indications for tHcy testing in the years 2016–2024 is shown in Figure 1C. In 2016–2018, VTE was the leading indication (55%–61%), followed by CAD (<21%). From 2020 onward, the trend reversed, with CAD becoming the most frequent indication in 2024 (n = 1020; 54.8%), while the proportion of VTE cases declined to 17.6% (n = 328; P <0.001). Cerebrovascular events remained a relatively stable indication, showing a slight increase from 16.7% in 2016 to 19.1% in 2024. In contrast, the frequency of PAD as the indication for testing, initially uncommon, rose sharply in 2023 and 2024, reaching 13.5% and 16.6% of cases, respectively.
The median (IQR) tHcy concentration in the whole group was 12.8 (10.2–16) µmol/l. Men had higher levels than women (median [IQR], 13.9 [11.6–17.1] vs 11.5 [9.2–14.6] µmol/l; P <0.001), which is at least in part associated with older age of the male population in the present study. A positive correlation was observed between the tHcy level and age in the whole patient group (R = 0.39; P <0.001).
As shown in Figure 1D, a total of 6416 patients (69.1%) had tHcy levels below 15 μmol/l, with a median (IQR) level of 11.2 (8.9–13.5) μmol/l. Within this subgroup, men had higher levels than women (median [IQR], 12.1 [9.8–13.9] vs 10.5 [8.3–12.8] μmol/l; P <0.001). Elevated tHcy concentrations between 15 and 100 μmol/l were found in 2843 individuals (30.6%), including 1055 women (37.1%). The median (IQR) tHcy concentration in this subgroup was 18.2 (15–20.5) μmol/l, and was similar in women and men (18.3 [15.3–21] vs 18.2 [14.9–20.2] μmol/l; P <0.001). The patients in this subgroup were older than those with concentrations below 15 μmol/l. The individuals with tHcy concentrations between 15 and 100 μmol/l had a higher prevalence of CAD (38.6% vs 28.1% of those with tHcy <15 μmol/l; P <0.001), PAD (12.9% vs 3.5%; P <0.001), and cerebrovascular events (21.5% vs 14.2%; P <0.001).
Of note, there were 10 patients (0.1%) with severe HHcy (tHcy >100 μmol/l), who had a median (IQR) tHcy level of 205.9 (154.5–256.5) μmol/l. Their characteristics are shown in Supplementary material, Table S1. None of these patients had stage 5 chronic kidney disease. Most patients were diagnosed with CAD and cerebrovascular diseases.
The survival status of patients was assessed through the end of October 2025. Two patients died: a 77‑year‑old woman from sudden cardiac death, and a 38‑year‑old man from massive pulmonary bleeding following cardiac surgery.
Genetic testing for the MTHFR C677T variant was requested in 533 patients (5.6%). In subsequent years, the number of genetic tests requested steadily declined from 184 in 2017 to as few as 16 in 2023 and 2 in 2024. The heterozygous CT genotype was the most frequent (n = 246; 46.2%), followed by the homozygous CC wild‑type genotype (n = 209; 39.2%) and the homozygous TT genotype (n = 78, 14.6%).
Next‑generation sequencing of the CBS gene was performed solely in 4 out of 10 patients with the highest tHcy levels. One patient was a carrier of a compound heterozygote of CBS variants c.833T>C (p.Ile278Thr) and c.1358+2T>A, and 2 individuals were homozygous for c.833T>C (Supplementary material, Table S1). One patient was heterozygous for c.833T>C.
Discussion
Our study shows that the number of tHcy level measurements has increased substantially over the past decade, despite the absence of recommendations supporting their routine use in contemporary cardiology or neurology guidelines. A significant proportion of tHcy level measurements were requested as part of comprehensive thrombophilia panels, both in outpatient and inpatient settings. Physicians increasingly used these panels in the setting of thromboembolic events, particularly after myocardial infarction or ischemic stroke, despite limited evidence supporting this practice.12 The rise in the frequency of tHcy testing was further driven by the persistent perception that this amino acid represents a modifiable vascular risk factor which should be treated with vitamins rather than targeted interventions.15
The change in clinical indications also shows that tHcy level testing moved further from evidence‑based practice. Initially performed primarily for VTE, it later became most commonly requested for CAD, despite a lack of guideline support. This pattern likely reflects local practice habits and highlights the need to align testing with current recommendations.
In our cohort, mild elevations (15–100 µmol/l) may partly result from an unverified fasting status, as dietary intake and nonfasting samples can modestly raise tHcy levels. Importantly, this limitation does not affect the interpretation of severe elevations (>100 µmol/l), which cannot be explained by nonfasting alone. Therefore, our observations regarding severe HHcy remain reliable.
We identified 10 adults with tHcy concentrations greater than 100 µmol/l, a finding strongly suggestive of an inherited disorder, such as classic homocystinuria. Despite this, these individuals received only low‑dose folate and were not referred for metabolic evaluation, which stands in stark contrast to the standard of care for confirmed or suspected homocystinuria. Optimal management requires assessment of pyridoxine responsiveness, with B6-responsive patients treated with high‑dose pyridoxine together with folate and vitamin B12 supplementation. In B6-nonresponsive individuals, treatment requires a strict low‑methionine diet supported by methionine‑free amino acid preparations and betaine therapy with ongoing specialist follow‑up.16 These distinctions underscore the fundamentally different therapeutic objectives in acquired and inherited forms of HHcy.16,17 Failure to provide appropriate management exposes patients to a significantly increased risk of thromboembolic and cerebrovascular complications and premature mortality. Thus, the detection of these cases underscores a substantial gap in clinical awareness.
Based on our analysis, tHcy level measurement in the cardiology settings appears to function more as an unintended screening tool for rare metabolic disorders, such as classic homocystinuria, rather than an effective marker for risk stratification of CAD. We believe that clarifying this distinction will help clinicians better understand the clinical implications of requesting this test. The 6‑fold increase in testing volume also carries resource implications without proportional clinical benefit. Funds allocated to routine tHcy testing could instead be used for the evaluation of clinically valuable biomarkers, such as Lp(a), which are recommended in cardiovascular guidelines.18
There is international evidence that genetic testing for the MTHFR C677T variant has no practical value in diagnosing patients with cardiovascular or neurologic disorders.8 The sharp decline in the frequency of MTHFR C677T testing reflects broad consensus that this variant lacks diagnostic or prognostic utility for these diseases.19 In contrast, targeted CBS gene sequencing was appropriately requested only in patients with severe HHcy, among whom pathogenic variants were identified.
In conclusion, contrary to expectations, the frequency of tHcy testing continued to increase despite the absence of guideline support.1 However, markedly elevated tHcy levels in adults may indicate an underlying genetic cause and should prompt appropriate genetic evaluation of the patient and their family members, as well as referral to a specialist in rare metabolic diseases.20 Our findings highlight the need for greater awareness, particularly among internists and cardiologists, regarding the diagnostic significance and management of severe HHcy. Although routine tHcy level measurement is not justified in the assessment of common cardiovascular conditions, markedly elevated levels require prompt metabolic evaluation and timely multidisciplinary care, a step that was often overlooked by the physicians who requested the test. Ensuring recognition and adequate treatment of such patients is essential to reducing preventable morbidity and premature mortality.
- Undas A, Perła‑Kaján J, Głowacki R. Homocysteine in adult patients with cardiovascular disease: is it clinically relevant in 2025? A tribute to Hieronim Jakubowski (1946‑2025). Pol Arch Intern Med. 2025; 135: 17012. | Crossref
- McCully KS. Vascular pathology of homocysteinemia: implications for the pathogenesis of arteriosclerosis. Am J Pathol. 1969; 56: 111‑128. | Crossref
- Perna AF, Ingrosso D. Homocysteine and chronic kidney disease: an ongoing narrative. J Nephrol. 2019; 32: 673‑675. | Crossref
- Cui L, Wang F, Li C, et al. Homocysteine and thyroid diseases. Front Endocrinol (Lausanne). 2025; 16: 1572997. | Crossref
- Tinelli C, Di Pino A, Ficulle E, et al. Hyperhomocysteinemia as a risk factor and potential nutraceutical target for certain pathologies. Front Nutr. 2019; 6: 49. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION