Serum Mas-related G protein–coupled receptor X2 concentration in drug-induced immediate hypersensitivity reactions
Key words: drug hypersensitivity reactions, fluoroquinolones, Hymenoptera venom, Mas-related G protein–coupled receptor X2, neuromuscular blocking agents

 CC BY 4.0
CC BY 4.0
Serum Mas-related G protein–coupled receptor X2 concentration in drug-induced immediate hypersensitivity reactions
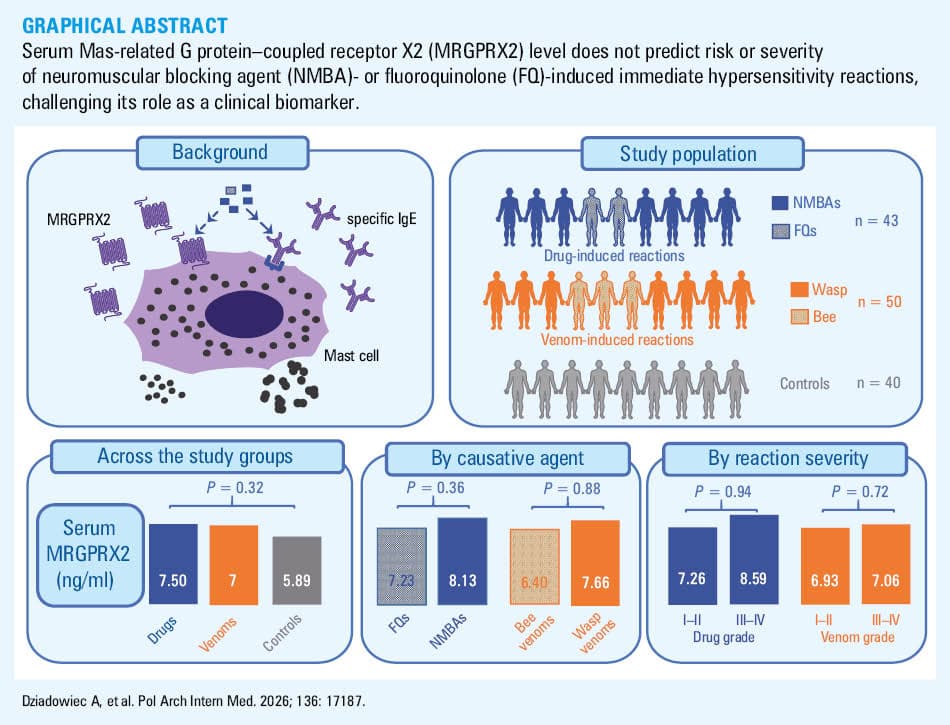
Introduction: Mas‑related G protein–coupled receptor X2 (MRGPRX2) has emerged as a mediator of mast cell activation in acute and chronic conditions. Exogenous ligands, such as neuromuscular blocking agents (NMBAs) and fluoroquinolones (FQs), can trigger MRGPRX2‑dependent activation and may augment immunoglobulin E (IgE)-mediated pathways. Although investigators have measured serum MRGPRX2 level in asthma, mastocytosis, and chronic urticaria, its role in immediate hypersensitivity reactions (IHRs) to FQs or NMBAs remains unclear.
Objectives: We conducted this study to determine whether increased serum MRGPRX2 concentration is a risk factor for IHRs to NMBAs or FQs, and whether its concentration is related to reaction severity, causative agent, or serum tryptase.
Patients and methods: We studied 43 patients with a history of IHRs to NMBAs or FQs, and compared them with 50 patients with IHR to Hymenoptera venom and 40 control individuals. The participants underwent a diagnostic evaluation that included skin testing, specific IgE measurement, and a basophil activation test when indicated. We measured serum MRGPRX2 level with an enzyme‑linked immunosorbent assay.
Results: Median serum MRGPRX2 concentrations with interquartile ranges for the drug‑induced reactions group, the Hymenoptera venom–induced reactions group, and the control group were 7.5 (3.73–15.64), 7 (3.96–10.62), and 5.89 (2.43–9.98) ng/ml, respectively (P = 0.32). Serum MRGPRX2 concentration showed no relationship with reaction severity, specific causative agents, or serum tryptase level.
Conclusions: In this cohort, serum MRGPRX2 concentration was not a risk factor for the investigated drug- and venom‑induced IHRs. These findings do not support using serum MRGPRX2 level as a predictor of the reaction occurrence or severity in these settings.
What's new?
Recent discoveries concerning the surface Mas‑related G protein–coupled receptor X2 (MRGPRX2) of mast cells have generated significant interest among clinicians and researchers investigating diseases involving these cells. Experimental studies have shown that several exogenous ligands, such as fluoroquinolones, neuromuscular blocking agents, and wasp venom components, can trigger MRGPRX2‑driven degranulation, raising concerns about its role in drug- and venom‑induced anaphylaxis. Yet, clinical implications of these observations remain uncertain. In particular, it is unclear whether elevated serum MRGPRX2 concentration is a risk factor for anaphylaxis upon exposure to the aforementioned agents. We provided the first clinical evidence that serum MRGPRX2 concentration neither predicts the severity of fluoroquinolone- or muscle relaxant–induced reactions, nor varies by a culprit agent, and it is not elevated as compared with controls. These findings may help guide pharmacotherapeutic decision‑making in patients with mast cell–related disorders, including Hymenoptera venom allergy and mastocytosis.
Introduction
In recent years, substantial attention has been paid to the role of the Mas‑related G protein–coupled receptor X2 (MRGPRX2) in mast cell–mediated diseases.1-5 Beyond its role in chronic conditions, such as asthma,6 MRGPRX2 activation has been implicated in immediate hypersensitivity reactions (IHRs),7 and incorporated into the latest European Academy of Allergy and Clinical Immunology classification as a mechanism of type VII hypersensitivity.8 Moreover, MRGPRX2 has recently been recognized as one of the key determinants in IHR endotypes.9 Importantly, MRGPRX2‑dependent and immunoglobulin E (IgE)-dependent pathways may act synergistically, amplifying mast cell activation and potentially facilitating IgE‑mediated anaphylaxis.10
The current interest in MRGPRX2‑related mechanisms originates from the seminal work of McNeil et al.11 Using an advanced research model, these authors demonstrated that mast cell degranulation can be induced by MRGPRX2 activation not only in response to endogenous ligands (eg, substance P), but also to noncanonical exogenous ligands, including neuromuscular blocking agents (NMBAs) and fluoroquinolones (FQs). This discovery established MRGPRX2‑dependent activation as a novel pathway for mast cell degranulation, independent of classical IgE‑mediated reactions, and provided an explanation for hypersensitivity reactions in patients without prior drug sensitization. Subsequent studies, however, have added complexity. Babina et al10 reported that IgE‑dependent and MRGPRX2‑dependent signals can converge to generate an additive response. Furthermore, Bawzair et al12 recently demonstrated that MRGPRX2 activation may facilitate development of IgE‑dependent anaphylaxis.
Despite these advances, major gaps remain in our understanding of MRGPRX2 in mast cell–related diseases; for instance, little is known about the clinical significance of circulating MRGPRX2. Only a few studies have examined serum MRGPRX2 concentration. Its elevated levels have been reported in asthma6 and severe urticaria,13,14 and have also been studied in mastocytosis and in anaphylaxis induced by iodinated contrast media.7,15 To date, however, serum MRGPRX2 levels have not been investigated in patients with a history of IHRs to NMBAs or FQs, leaving it unclear whether MRGPRX2 might serve as a biomarker for such reactions.
In this study, we sought to determine whether serum MRGPRX2 concentrations are elevated in patients with immediate drug‑induced hypersensitivity reactions in comparison with controls from the general population. We also included a comparison group of patients with severe immediate allergic reactions to Hymenoptera (wasp and bee) venom, who, to our knowledge, have not previously been studied in this context. This group is of particular interest, given that wasp venom contains mastoparan, a known MRGPRX2 agonist,16 and considering clinical observations reported in the literature suggesting that recurrent anaphylaxis following exposure to both Hymenoptera venom and ciprofloxacin may be mediated by MRGPRX2 activation.1,17 Finally, we investigated whether serum MRGPRX2 concentration is associated with 1) the severity of the clinical reaction, 2) the causative agent, or 3) serum tryptase level.
Patients and methods
Clinical diagnostic workup
Reaction severity in patients was graded using the Ring and Messmer system.18,19 Standard diagnostic workups were performed to identify the culprit agent, including skin prick testing, intradermal testing, measurement of specific IgE, and basophil activation tests when indicated.19-21 The patients with NMBA hypersensitivity who had experienced perioperative reactions were confirmed negative for other potential causes. Systemic mastocytosis was diagnosed according to established criteria.22
Laboratory diagnostic procedures
Serum tryptase and specific IgE concentrations were measured using the commercial ImmunoCAP assay (Thermo Fisher, Waltham, Massachusetts, United States), as described previously.23,24 For NMBAs, IgE specific to morphine was measured as a surrogate, given the shared dominant epitopes between morphine and NMBAs.25 Basophil activation tests were performed and analyzed according to previously established protocols.26,27 Briefly, the Flow2 CAST assay (Bühlmann Laboratories AG, Schönenbuch, Switzerland) was used. Basophils were identified as CCR3+/SSC‑low (EDTA samples) or CD123+/HLA‑DR+ (heparinized samples from Golnik, Slovenia). Results were considered positive with at least 5% CD63+ basophils and a stimulation index equal to or above 2. Nonresponders were excluded. The blood samples were collected on a scheduled basis as part of routine diagnostic evaluations.
Enzyme‑linked immunosorbent assay
Whole blood from the patients and controls was collected into S‑Monovette serum separator vacutainer tubes (Sarstedt AG, Nümbrecht, Germany). The samples were centrifuged at 1500 × g for 15 minutes, and serum was carefully separated, aliquoted into clean tubes, and stored at −80 °C. MRGPRX2 concentration in the serum samples was measured using a commercial enzyme‑linked immunosorbent assay (ELISA) kit (MyBioSource, MBS9333336, San Diego, California, United States) according to the manufacturer’s instructions. Prior to ELISA testing, serum samples were centrifuged at 1500 × g for 10 minutes at 4 °C, and the supernatant was carefully collected for analysis.
Statistical analysis
Baseline characteristics were summarized using descriptive statistics (counts and percentages for qualitative variables, and median with interquartile range [IQR] for continuous data). Normality of distribution was assessed with the Shapiro–Wilk test. Results are reported as medians with IQR due to the non‑normal distribution of the variables. The Kruskal–Wallis test was used for multiple group comparisons, and the Mann–Whitney test for comparisons between 2 groups. Associations between MRGPRX2 and tryptase level were evaluated using the Spearman correlation. All tests were 2‑tailed. The analyses were performed with GraphPad Prism package (GraphPad Software, La Jolla, California, Unites States), with significance set at a P value below 0.05.
The study was conducted in accordance with the Declaration of Helsinki, and was approved by the appropriate bioethics committees of the Jagiellonian University, Poland and the University Clinic Golnik, Slovenia (1072.6120.175.2020 and KME 150/09/13, respectively). Written informed consent was obtained from all participants.
Results
The study included 43 patients who had experienced IHRs to NMBAs or FQs, 50 patients with IHRs to Hymenoptera venom, and a control group of 40 individuals from the general population without a history of hypersensitivity to NMBAs, FQs, or Hymenoptera venom. Median (IQR) age of the drug‑induced reaction group was 56 (43–63) years, and the group included 29 women and 14 men. Median age of the venom‑induced reaction group was 53 (45–68) years, with 26 women and 24 men. Finally, median age of the control group was 41 (34–50) years, and it comprised 27 women and 13 men. Additional clinical details are provided in Table 1.
Variable | Patients with drug‑induced hypersensitivity reactions (n = 43) | Patients with Hymenoptera venom–induced hypersensitivity reactions (n = 50) |
Data are presented as median (interquartile range) unless indicated otherwise.
a Allergen‑specific IgE for ciprofloxacin is not commercially available.
Abbreviations: FQ, fluoroquinolone; Ig, immunoglobulin; nd, not done; NMBA, neuromuscular blocking agent | ||
Culprits | FQs: ciprofloxacin (n = 7) | Bee venom (n = 19) |
NMBAs: atracurium (n = 8); rocuronium (n = 21); cisatracurium, vecuronium, suxamethonium (n = 2 each); pipecuronium (n = 1) | Wasp venom (n = 31) | |
Ring and Messmer grade I; II; III; IV, n (%) | 7 (17.1); 9 (22); 24 (58.5); 1 (2.4) | 2 (4); 4 (8); 41 (82); 3 (6) |
Specific IgEa, kUA/l | 0.02 (0.001–0.04) | 3 (1.17–18.3) |
Basal serum tryptase, ng/ml | 4.43 (3.39–6.7) | 5.83 (4.8–11.9) |
Basophil activation test | Positive in 18 out of 40 performed | nd |
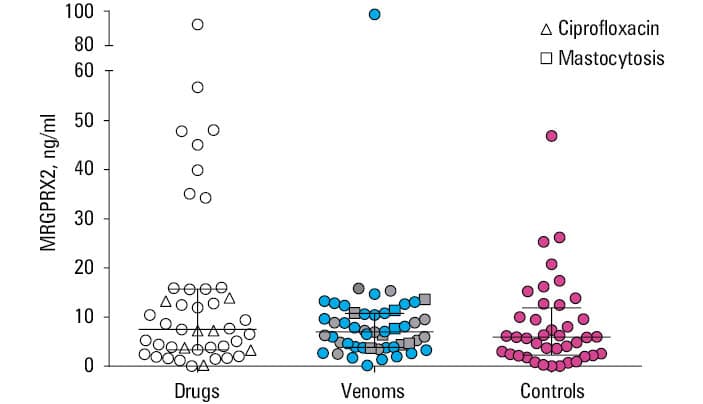
The results of serum MRGPRX2 measurements in the 3 study groups are shown in Figure 1. Median (IQR) values were 7.5 (3.73–15.64) ng/ml in the drug‑induced reaction group, 7 (3.96–10.62) ng/ml in the Hymenoptera venom–induced reaction group, and 5.89 (2.43–9.98) ng/ml in the control group. No marked differences were observed among the groups (P = 0.32).
Serum MRGPRX2 concentrations stratified by reaction severity are presented in Table 2. Reactions graded I–II on the Ring and Messmer scale were compared with those graded III–IV within each group. The differences were insignificant, as were those between all patients with grade I–II reactions, all patients with grade III–IV reactions, and controls (P = 0.3).
Variable | Reaction grade I and II (n = 22) | Reaction grade III and IV (n = 69) | P value |
Data are presented as median (interquartile range) in ng/ml.
a Clinical presentations of 2 patients were not sufficiently distinct to assign them to any group. | |||
Drug‑induced reaction | 7.26 (3.32–34.27) | 8.59 (4.03–15.64) | 0.94 |
Venom‑induced reaction | 6.93 (5.96–8.07) | 7.06 (3.96–10.79) | 0.72 |
All patientsa | 7.23 (3.85–15.35) | 7.66 (3.96–12.35) | 0.99 |
Serum MRGPRX2 concentrations stratified by a causative agent are shown in Table 3. Comparisons included the patients with reactions to FQs vs NMBAs, bee venom vs wasp venom, and all drug‑induced vs all venom‑induced reactions. None of these comparisons revealed significant differences, as was the case for the comparisons between drug‑induced reactions, venom‑induced reactions, and controls (P = 0.32).
Reaction type | Causative agent | Value | P value |
Data are presented as median (interquartile range) in ng/ml.
Abbreviations: see Table 1 | |||
Drug‑induced reaction | FQs (n = 7) | 7.23 (3.73–7.26) | 0.36 |
NMBAs (n = 36) | 8.13 (3.81–15.91) | ||
Venom‑induced reaction | Bee venom (n = 19) | 6.4 (4.82–8.88) | 0.88 |
Wasp venom (n = 31) | 7.66 (3.77–10.79) | ||
All patients | Drugs (n = 43) | 7.5 (3.73–15.64) | 0.48 |
Venoms (n = 50) | 7 (3.85–10.62) | ||
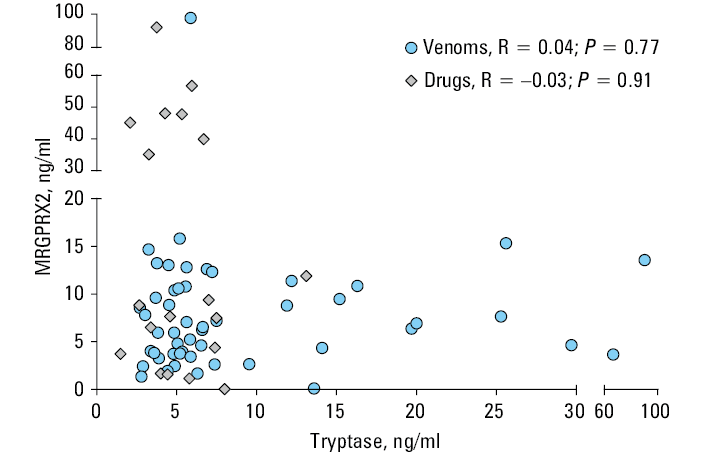
The correlation analysis between serum MRGPRX2 and tryptase concentrations is shown in Figure 2. MRGPRX2 levels did not correlate with tryptase concentrations. Eight patients in the venom‑induced reaction group had systemic mastocytosis. Their serum MRGPRX2 levels did not differ from those of other patients with venom‑induced reactions (P = 0.73) or controls (P = 0.42; Figure 1).
Discussion
Serum Mas‑related G protein–coupled receptor X2 concentration across study groups
Our study did not show significant differences in serum MRGPRX2 concentrations among the study groups, that is, the patients with drug‑induced hypersensitivity reactions (NMBAs and FQs), patients with venom (wasp and bee)-induced reactions, and healthy controls (Figure 1). Previous studies have reported elevated serum MRGPRX2 levels in patients with asthma, particularly allergic asthma, as compared with healthy individuals.6 Some reports in chronic urticaria suggest that serum MRGPRX2 level may be a risk factor for severe chronic spontaneous urticaria (CSU)13 and that its concentrations are higher in severe CSU, as compared with nonsevere CSU but not with controls.14 Another study28 found increased MRGPRX2 concentration in patients with chronic urticaria relative to controls, but measurements were taken from whole blood rather than serum. In chronic prurigo, serum MRGPRX2 concentration correlated with clinical severity, although the study included only 10 patients.29 Taken together, the available evidence on the clinical relevance of serum MRGPRX2 levels is inconsistent (chronic urticaria) or limited to single reports (asthma and chronic prurigo). Notably, most reports have addressed chronic mast cell–related conditions, whereas evidence in immediate hypersensitivity is scarce and limited to a single study on reactions induced by iodinated contrast media.7 In that study, serum MRGPRX2 concentrations were higher in patients with anaphylaxis than in those with nonanaphylactic reactions, though the difference was borderline significant (P = 0.044).
Relationship to reaction severity and causative agents
The rationale for considering reaction severity as a differentiating factor in MRGPRX2- vs IgE‑dependent mechanisms comes from Gaudenzio et al,30 who showed that mast cells produce small, rapidly released granules following MRGPRX2 activation, whereas IgE‑dependent activation triggers larger granules and more prolonged responses. In murine models, this translated into more severe systemic anaphylaxis in IgE‑dependent reactions. However, our data showed that reaction severity was not dependent on serum MRGPRX2 concentration. As presented in Table 2, there were no significant differences in MRGPRX2 concentration between grade I–II and grade III–IV reactions, either in the group of patients with drug‑induced reactions or in the group with reactions induced by wasp or bee venom. Similarly, a comparison of all patients with grade I–II reactions and those with grade III–IV reactions showed no significant difference in MRGPRX2 concentration (Table 2). Mastoparan, a wasp venom peptide, is a confirmed MRGPRX2 agonist,11,16,31 which could theoretically contribute to symptom development in venom‑induced reactions. Nonetheless, a comparison of MRGPRX2 concentrations as per the causative agent demonstrated no differences between the patients with wasp venom allergy and the other participants (Table 3). Current knowledge of drug ligands that activate MRGPRX2 is largely based on experiments conducted in cell lines or animal models. Consequently, it remains unclear whether the differences among drug groups that act as MRGPRX2 agonists are of practical significance in vivo in humans. As shown in Table 3, our study found no differences in serum MRGPRX2 levels between the patients reacting to FQs and NMBAs, or between the patients with bee- and wasp venom–induced reactions. Furthermore, no difference in MRGPRX2 concentration was observed when comparing all patients with drug‑induced reactions with those with reactions induced by wasp or bee venom (Table 3). These findings suggest that serum MRGPRX2 levels in vivo may not reflect pathway‑specific activation in humans.
Serum Mas‑related G protein–coupled receptor X2 concentration in mastocytosis and correlation with tryptase level
Systemic mastocytosis is a prototypical mast cell–related disease and a common comorbidity in patients with severe Hymenoptera venom allergy.24 Patients with mastocytosis who exhibit hypersensitivity to MRGPRX2‑activating drugs have been recently identified,32 highlighting the need for tailored management strategies.1 To date, only 1 study has measured serum MRGPRX2 levels in systemic mastocytosis,15 finding no elevation in comparison to controls, which is consistent with our results. That study also analyzed correlations between serum MRGPRX2 levels and tryptase, a well‑established mast cell biomarker, but found none—again paralleling our findings (Figure 2). It should be noted that tryptase is a granule‑derived enzyme, whereas MRGPRX2 is a membrane receptor, which may explain differences in their detectability in serum. Interestingly, both tryptase and MRGPRX2 have been detected in extracellular vesicles released from mast cells and isolated from serum, with their presence observed in patients with mastocytosis but not in healthy individuals.33 Overall, our results indicate that serum MRGPRX2 concentration does not differentiate patients by reaction severity or causative agent, and is not elevated in mastocytosis, suggesting its limited utility as a circulating biomarker in IHRs.
Limitations
When interpreting the study findings, its limitations should be considered. One of these is the relatively small number of included patients, particularly in the subgroup with drug‑induced reactions, as compared with studies on asthma or chronic urticaria.7,13 Increasing the sample size and representativeness in future research would further enhance the reliability and generalizability of the findings. In addition, regarding serum MRGPRX2 concentration, discrepancies among previous studies may reflect methodological differences. Many investigations, including ours, have detected measurable MRGPRX2 concentrations in both study and control groups.5,7,13-15 However, the aforementioned study by Kim et al33 reported the presence of MRGPRX2 in extracellular vesicles in patients with mastocytosis, but not in healthy individuals. Proteomic approaches could further verify the rate at which the receptor is released into circulation. This has not yet been researched in such studies.34,35
Conclusions and perspectives
Our study found no evidence that elevated serum MRGPRX2 concentration constitutes a risk factor for IHRs to FQs, NMBAs, or Hymenoptera venoms, unlike previous reports in asthma, chronic urticaria, and contrast media–induced anaphylaxis.6,7,13 To our knowledge, this is the first study to address this question, filling a critical knowledge gap regarding the clinical relevance of serum MRGPRX2 levels in these patient groups. Despite growing interest in MRGPRX2‑mediated immediate reactions, many clinical questions remain unresolved. For instance, it is unclear whether patients with mastocytosis who experience allergic symptoms in response to a known MRGPRX2 agonist (eg, NMBA) should avoid exposure to other agonists (eg, FQs). Our findings do not support such preventive recommendations, nor do they confirm a direct clinical role for MRGPRX2 in the investigated reactions.
Reporting these negative results helps prevent systematic bias arising from selective publication of positive findings, thereby supporting the reliability and completeness of scientific evidence.36,37 It also fulfills an ethical obligation to study participants by ensuring that the data they contributed are made publicly available.38 Moreover, by ruling out one hypothesis, these results can guide future research toward alternative explanations, such as MRGPRX2 genetic polymorphisms that increase receptor affinity for specific ligands or elevated local receptor expression in individuals hypersensitive to MRGPRX2 agonists.39,40
- Castells M, Madden M, Oskeritzian CA. Mast cells and Mas‑related G protein‑coupled receptor X2: itching for novel pathophysiological insights to clinical relevance. Curr Allergy Asthma Rep. 2024; 25: 5. | Crossref
- Olivieri B, Ghilarducci A, Nalin F, Bonadonna P. Mast cell conditions and drug allergy: when to suspect and how to manage. Curr Opin Allergy Clin Immunol. 2024; 24: 195‑202. | Crossref
- Worm M, Pazur K, Morakabati P, Redhu D. IgE and non‑IgE‑mediated pathways in anaphylaxis. Semin Immunopathol. 2025; 47: 34. | Crossref
- Alvarez‑Arango S, Kumar M, Chow TG, Sabato V. Non‑IgE‑mediated immediate drug‑induced hypersensitivity reactions. J Allergy Clin Immunol Pract. 2024; 12: 1109‑1119. | Crossref
- Kolkhir P, Ali H, Babina M, et al. MRGPRX2 in drug allergy: what we know and what we do not know. J Allergy Clin Immunol. 2023; 151: 410‑412. | Crossref
ARTICLE INFORMATION