Circadian variation in ST-segment elevation myocardial infarction: a nationwide analysis of onset, treatment delays, and culprit artery patterns
Key words: chronobiology, circadian rhythm, percutaneous coronary intervention, ST-segment elevation myocardial infarction, treatment delay

 CC BY 4.0
CC BY 4.0
Circadian variation in ST-segment elevation myocardial infarction: a nationwide analysis of onset, treatment delays, and culprit artery patterns
Introduction: ST‑segment elevation myocardial infarction (STEMI) onset follows a circadian rhythm, yet data from large contemporary national registries remain limited, particularly regarding how the onset time influences treatment delays and coronary pathology.
Objectives: We aimed to examine circadian patterns of STEMI onset and their impact on treatment delays, culprit vessel involvement, and periprocedural mortality.
Patients and methods: We retrospectively analyzed 153 543 STEMI patients from the Polish National Percutaneous Intervention Registry hospitalized between 2014 and 2022. We examined the hourly distribution of symptom onset and its associations with patient characteristics, treatment delays, and infarct‑related artery location.
Results: STEMI onset showed pronounced circadian variation, peaking at 8:00 AM. Although the overall pattern was similar between sexes (P for interaction = 0.15), median onset time occurred earlier in men than women (10:00 AM vs 11:00 AM; P = 0.007). Nocturnal onset (eg, 3:00 AM) was associated with substantially longer median pain‑to‑first‑medical‑contact times than daytime onset (180 vs 90 min at 1:00 PM; P <0.001). We identified a novel opposing circadian rhythm for the infarct‑related artery location—the left anterior descending (LAD) artery seemed to be the main culprit during nocturnal hours with a nadir at noon, while the right coronary artery (RCA) involvement demonstrated an inverse pattern (P <0.001). Despite delayed presentation, periprocedural mortality did not vary significantly by onset time.
Conclusions: This large nationwide cohort demonstrates that STEMI onset follows a robust circadian pattern significantly affecting system delays. The discovery of opposing circadian rhythms for LAD and RCA involvement suggests that time of day influences not only STEMI triggering but also its pathophysiological manifestation.
What's new?
Using data from over 150 000 ST‑segment elevation myocardial infarction (STEMI) patients listed in a Polish national registry, we confirmed that heart attacks follow a strong circadian rhythm, peaking at 8:00 AM. Critically, patients experiencing symptoms during night‑time hours (midnight to 5:00 AM) waited twice as long before seeking medical help than those with daytime symptom onset, which represented a major barrier to timely treatment. We found that the specific coronary artery causing the heart attack varies by the time of day, with left anterior descending artery blockages peaking at night and right coronary artery blockages peaking during daytime, suggesting that circadian biology influences not just when heart attacks occur but also their anatomical manifestation. These findings highlight the need for targeted public health campaigns addressing night‑time treatment delays and suggest that chronobiological factors may influence coronary plaque vulnerability in different vascular territories. Future research should explore whether time‑specific preventive strategies could reduce STEMI incidence and improve outcomes.

Introduction
Acute cardiovascular events follow predictable temporal patterns governed by the body’s circadian rhythm.1-3 This 24‑hour biological clock orchestrates physiological processes that prepare the body for sleep‑wake transitions. Epidemiologic studies have consistently demonstrated that major cardiovascular events—including acute myocardial infarction (MI), stroke, and sudden cardiac death—peak between 6:00 AM and noon across diverse populations.1-5 This morning vulnerability reflects convergent prothrombotic and hemodynamic stressors accompanying the transition from sleep to wakefulness.1-3 Awakening triggers a surge in sympathetic activity and circulating catecholamines, increasing heart rate, blood pressure, and myocardial oxygen demand.6 Concurrently, the hematologic system shifts toward a prothrombotic state: platelet aggregability peaks and plasminogen activator inhibitor‑1 (PAI‑1) activity rises, creating conditions favoring thrombus formation upon plaque rupture.1,2,7 These endogenous rhythms are amplified by exogenous factors including postural changes, physical activity, and psychological stress.1,2,6
Although the morning acute MI peak is well‑established, critical questions remain in modern cardiology.5 First, foundational studies predate widespread adoption of primary percutaneous coronary intervention (PCI) for ST‑segment elevation myocardial infarction (STEMI).8,9 Whether this biological rhythm persists in contemporary populations treated within regional systems of care remains unclear.8-11 Second, the impact of circadian patterns on modern STEMI treatment pathways requires clarification. Current guidelines recommend door‑to‑balloon times below 90 minutes for PCI‑capable hospitals.12,13 While off‑hours presentation may delay treatment, this relationship has not been quantified in large contemporary registries.11,14,15 Understanding how biological timing influences system performance is essential for optimizing care delivery. Finally, whether the circadian rhythm influences not only STEMI triggering but also the specific coronary artery that becomes occluded remains unexplored. Preliminary evidence suggests culprit vessel location may exhibit circadian variation, but robust data from large cohorts are lacking.8,9 Identifying such patterns could provide new mechanistic insights into time‑dependent STEMI pathophysiology.1
Using a large nationwide STEMI registry, this study aimed to characterize the 24‑hour pattern of STEMI onset by sex and age and investigate how cardiovascular risk factors influence this pattern. We sought to quantify the impact of onset time on treatment delays in the primary PCI pathway. Additionally, we tested the novel hypothesis that culprit vessel location exhibits circadian variation, potentially revealing time‑dependent differences in STEMI pathophysiology.
Patients and methods
The Polish National PCI Registry (ORPKI), a comprehensive national registry managed by the Jagiellonian University Medical College, Kraków, Poland, documents all coronary angiographies and PCIs performed in Poland.16-18 Between January 1, 2014, and December 31, 2022, we analyzed data from 153 543 consecutive STEMI patients who underwent coronary angiography and primary PCI across 154 centers. Data were collected prospectively using standardized case report forms. STEMI diagnosis and treatment followed contemporary guidelines.12 The primary variable for this analysis was the hour of symptom onset, as reported by patients or witnesses and documented by physicians, categorized into 24 one‑hour intervals. Treatment delays were calculated from 3 key time points: symptom onset, first medical contact (FMC), and PCI initiation (defined as first balloon inflation or wire passage). Delay intervals included: 1) pain‑to‑FMC time (patient delay), 2) FMC‑to‑PCI time (system delay), and 3) total ischemic time (pain‑to‑PCI).18 Operators determined pharmacotherapy and procedural techniques according to contemporary standards. The infarct‑related artery (IRA), identified on angiography, was categorized as the left anterior descending (LAD) or right coronary artery (RCA) to examine circadian variation in culprit vessel location. The primary clinical outcome was periprocedural mortality (in catheterization laboratory). In addition, data on other periprocedural complications, including stroke, cardiac arrest, coronary artery perforation, dissection, no‑reflow, allergic reaction, and puncture site bleeding were collected.
Statistical analysis
Baseline characteristics were summarized using descriptive statistics. Continuous variables were summarized as mean and SD or median with interquartile range (IQR), and compared using analysis of variance (ANOVA) or the Kruskal–Wallis test, as appropriate for data distribution. Categorical variables were presented as counts and percentages, and compared using the χ2 or likelihood ratio test, if the χ2 assumptions were not met. The 24‑hour distribution of STEMI onset was visualized by plotting the percentage of total events per hour. To identify specific hourly differences in continuous variables, such as age and weight, post hoc pairwise comparisons were performed using the Tukey–Kramer honestly significant difference test. The Wilcoxon rank‑sum test was used to compare median onset times between sexes. To explore whether circadian patterns in treatment delay were modified by patient characteristics, we tested for interactions between the onset hour and baseline features (sex, age >65 y, diabetes mellitus, prior MI, PCI, coronary artery bypass grafting, stroke, chronic kidney disease [CKD], chronic obstructive pulmonary disease [COPD], hypertension, current smoking, and psoriasis). To assess clinical impact, multivariable logistic regression models were used to evaluate associations between circadian onset timing, ischemic time, and the composite outcome of periprocedural complications or death, including onset hour × ischemic time interaction terms. The interactions were analyzed using multiple regression models, and significance in the interaction term was tested using the likelihood ratio test. Model assumptions were assessed by the examination of model residuals. Procedural characteristics (contrast volume and radiation exposure) were also compared across circadian onset hours using ANOVA with post hoc pairwise contrasts. Significance was set at a P value below 0.05 (2‑sided). The analyses were performed using R software, version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria) with the rms package, version 6.7–1.
Results
A total of 153 543 patients with STEMI were included in the final analysis. Table 1 presents the baseline demographic and clinical characteristics of the cohort. The study population included predominantly men (68%), at a mean age of 65.2 (12.1) years.
Characteristic | Total cohort (n = 153 543) |
Data are presented as number (percentage) or mean (SD). | |
Age, y | 65.2 (12.1) |
Men | 104 316 (68) |
Weight, kg | 80.8 (16) |
Comorbidities | |
Arterial hypertension | 92 055 (59.9) |
Current smoking | 47 773 (31.1) |
Diabetes mellitus | 27 724 (18.1) |
Previous myocardial infarction | 19 629 (12.8) |
Previous percutaneous coronary intervention | 18 328 (11.9) |
Chronic kidney disease | 5328 (3.5) |
Previous stroke | 5010 (3.3) |
Chronic obstructive pulmonary disease | 2931 (1.9) |
Previous coronary artery bypass grafting | 2573 (1.7) |
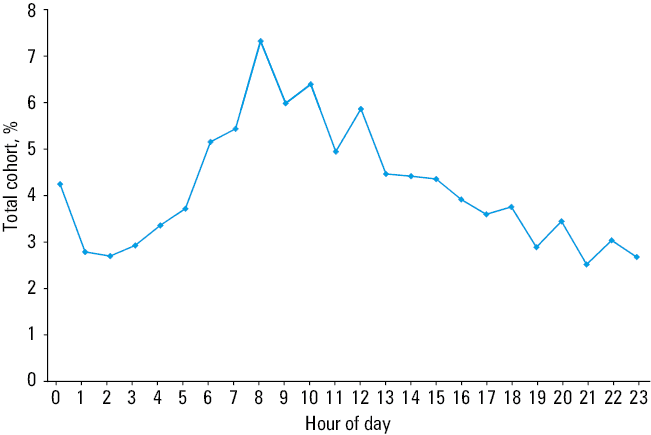
The onset of STEMI demonstrated a distinct and significant circadian variation across the 24‑hour cycle. As illustrated in Figure 1, STEMI incidence followed a bimodal pattern characterized by a prominent morning peak and a smaller evening peak. The frequency of STEMI onset rose steeply after 5:00 AM, culminating in a sharp peak at 8:00 AM that accounted for 7.3% of all daily events. Following this peak, incidence gradually declined throughout the day before reaching a secondary, less pronounced peak between 6:00 PM and 8:00 PM. The nadir occurred during the late night and early morning hours, with the lowest frequency observed between 1:00 AM and 3:00 AM.
Both sexes exhibited a broadly similar bimodal circadian pattern of STEMI onset. However, the distribution differed by sex (P <0.001). Median onset occurred earlier in men (10:00 AM [6:00 AM–4:00 PM]) than in women (11:00 AM [7:00 AM–4:00 PM]; P = 0.007). The circadian pattern remained unaffected by age (>65 vs ≤65 y), diabetes status, or COPD.
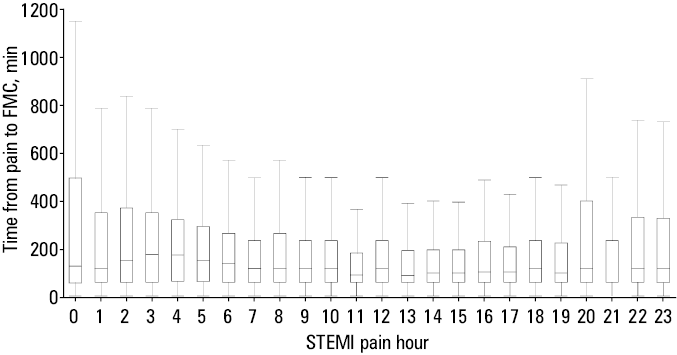
The time of symptom onset significantly influenced treatment delays. Patient‑related delay, measured as pain‑to‑FMC time, was longest for nocturnal STEMIs. Median pain‑to‑FMC time for 3:00 AM events was 180 (60–360) minutes, that is, 2 times longer than for 1:00 PM events (90 [59–196] min; P <0.001; Figure 2). System‑related delays showed similar patterns, with median FMC‑to‑PCI time longer for morning‑onset STEMIs (87 [60–14] min at 7:00 AM) than afternoon‑onset events (77 [52–120] min at 1:00 PM). Consequently, total ischemic time from chest pain onset to PCI varied significantly by time of day. When stratified by baseline characteristics, the circadian variation in pain‑to‑FMC delays persisted across all subgroups. Formal interaction testing showed that sex was not a significant effect modifier (P = 0.15). However, several comorbidities demonstrated significant interactions with circadian timing. Patients with diabetes (P = 0.004), CKD (P <0.001), COPD (P = 0.008), and aged above 65 years (P <0.001) exhibited more pronounced nocturnal delays than those without these characteristics. Prior cardiovascular history (previous MI, PCI) similarly influenced the circadian distribution of both STEMI onset times and treatment delays (P <0.001 for all; Supplementary material, Figure S1).
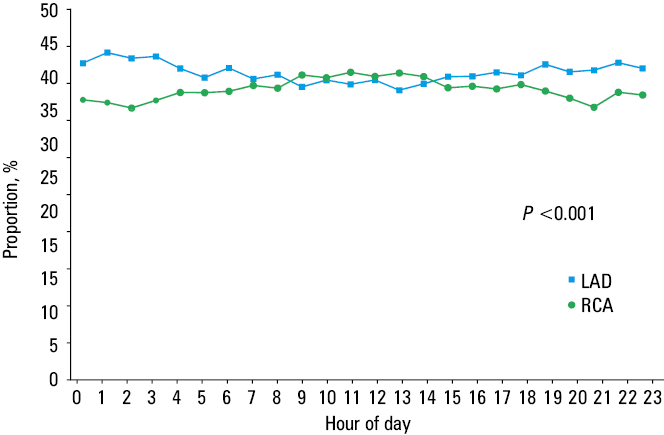
A novel finding of this study is a confirmation of opposing circadian rhythms for IRA location (P <0.001). LAD involvement peaked around midnight and reached its nadir at noon, showing greater frequency during nocturnal hours. Conversely, RCA involvement demonstrated the opposite pattern, peaking during daytime hours and reaching its nadir at night (Figure 3). Contrast volume and radiation exposure demonstrated modest circadian variation. Mean contrast volumes were slightly lower in the patients presenting during the early morning hours, as compared with daytime presentations (eg, midnight vs 6:00 AM: mean difference –4.9 [1.2] ml; P = 0.01). Similarly, radiation exposure was significantly lower for STEMIs occurring at midnight than late evening (mean difference –71.7 [18.4] mGy; P = 0.02; Supplementary material, Figure S2). However, these differences, while significant owing to the large sample size, were of limited clinical significance.
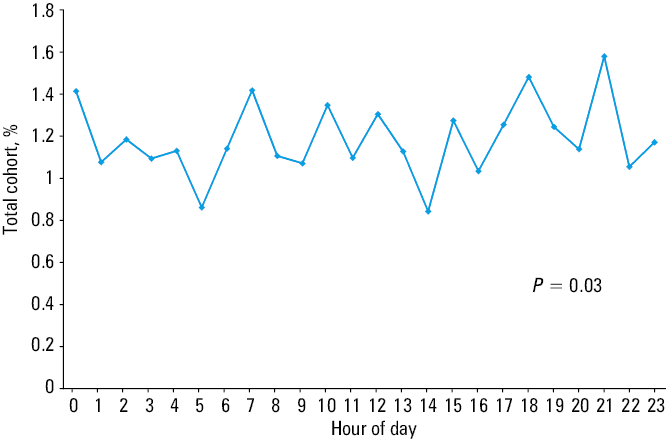
Periprocedural death occurred in 1.18% of patients. An analysis stratified by the hour of symptom onset demonstrated mortality rates ranging from 1.05% to 1.58% (Figure 4). Peak mortality was observed among the patients with symptom onset at 9:00 PM (1.58%; 95% CI, 1.21–2.04) and 6:00 PM (1.48%; 95% CI, 1.12–1.93). The χ2 analysis demonstrated temporal heterogeneity in mortality risk across the 24‑hour period (P = 0.03). In comparison with the overall cohort mortality rate, the patients presenting with symptom onset at 9:00 PM (P = 0.03) and 6:00 PM (P = 0.04) showed a significantly elevated crude mortality risk. However, these associations did not remain significant following the Bonferroni correction for multiple comparisons. Similarly, STEMI onset hour predicted the occurrence of periprocedural complications (P = 0.02) and the composite end point of PCI‑related complications or death (P = 0.02). Pain‑to‑FMC time was a strong independent predictor of adverse outcomes, with longer delays associated with increased complication and mortality rates (P <0.001). Importantly, no significant interaction was detected between the onset hour and delay time, indicating that prolonged ischemic time confers an increased risk regardless of the circadian timing of symptom onset.
Discussion
This large‑scale, nationwide registry study confirms that STEMI onset, rather than occurring randomly, follows a distinct circadian pattern, even in the modern era of primary PCI. Our primary finding—a morning peak in STEMI incidence around 8:00 AM—aligns with extensive historical and contemporary evidence.4,5,8-11 This morning vulnerability results from converging physiological changes that occur upon awakening: sympathetic nervous system activation, elevated blood pressure and heart rate, and a prothrombotic state characterized by increased platelet aggregability and PAI‑1 activity.1-3,6,7,19 Data from over 153 000 patients robustly confirm that these fundamental biological rhythms remain powerful STEMI triggers, regardless of advances in cardiovascular therapies.
While our study demonstrates clear circadian patterns in STEMI timing, it is crucial to recognize that these patterns are not uniform across all populations.20-28 The timing of STEMI represents a highly personalized risk profile shaped by the complex interplay between the body’s molecular clock and individual demographic and clinical characteristics.1,2 Sex influences remain complex and controversial.20,21,27 Although our data show both men and women exhibit the primary morning peak, the literature harbors conflicting evidence. Some studies report attenuated morning peaks or bimodal patterns (morning and evening) in women, potentially reflecting either confounding factors—as women in cardiovascular studies tend to be older and have more comorbidities—or underlying genetic differences, including sex‑specific variations in the CLOCK gene.27 Age effects are more consistently established.25,26 While the morning peak persists across all age groups, elderly patients frequently develop a secondary evening peak, creating a bimodal pattern rarely seen in younger individuals. This shift likely reflects age‑related weakening of circadian system resilience, allowing later‑day stressors to trigger cardiovascular events.6,21,25,26 In addition, clinical comorbidities act as powerful circadian modulators. Long‑standing diabetes can significantly blunt or abolish the morning STEMI peak, primarily through diabetic autonomic neuropathy that dampens the physiological morning sympathetic surge.21,23,24,28 Similarly, the “nondipper” hypertensive phenotype, where nocturnal blood pressure fails to decline, creates continuous rather than periodic hemodynamic stress, potentially disrupting typical circadian patterns.20-22 High triglyceride levels uniquely accentuate the morning peak on weekdays but not weekends, suggesting work‑stress interactions.21 These factors underscore that STEMI timing reflects not just molecular clock function but its complex interaction with individual pathophysiology. Our subgroup analyses further support the notion that patient characteristics modulate circadian patterns in treatment delays. Although sex was not a significant effect modifier of circadian delays (P = 0.15), the patients with diabetes, CKD, COPD, and those aged over 65 years exhibited more pronounced nocturnal delays than their respective counterparts without these characteristics. Prior cardiovascular disease (previous MI or PCI) similarly influenced the circadian distribution of both symptom onset and treatment delays. These findings suggest that comorbidities may amplify circadian vulnerability, predisposing high‑risk subgroups to disproportionately longer delays when symptoms occur during nocturnal hours.
Our analysis brought to light a novel and mechanistically intriguing finding, that is, opposing circadian rhythms for culprit vessel location. The predominance of LAD as IRA at night and RCA involvement during the day represent a significant discovery previously suggested only in smaller studies.8 The morning peak in RCA‑related events corresponds with established cardiovascular pathophysiology. Upon waking, abrupt increases in sympathetic tone, blood pressure, and heart rate create substantial hemodynamic stress.1,2,7 This vulnerability is further explained by the RCA’s unique hemodynamic profile: while both coronary arteries exhibit predominantly diastolic flow,29 Seligman et al30 demonstrated that the RCA has a significantly lower diastolic‑to‑systolic velocity ratio, exposing it to higher systolic flow and pressure. As RCA perfusion occurs throughout both cardiac phases, this increased systolic exposure combined with morning sympathetic surges may particularly predispose the RCA to plaque rupture during early morning hours.29,30 Conversely, the nocturnal LAD‑related STEMI peak suggests different triggering mechanisms. LAD perfusion occurs predominantly during diastole, when nocturnal conditions feature lower heart rate and blood pressure alongside distinct hormonal and autonomic states, including increased vagal tone and inflammatory mediators.29,30 Factors beyond the morning sympathetic surge—such as nocturnal inflammation, endothelial dysfunction, or sleep‑related phenomena (eg, obstructive sleep apnea31)—may preferentially trigger LAD events. Our findings gain particular significance when compared with recent international studies. Chan et al8 in Australia similarly reported morning RCA occlusion peaks and reduced morning LAD occlusion frequency, supporting our results. However, Seneviratna et al9 in Singapore found anterior STEMIs (LAD occlusion surrogates) most prevalent during midnight to 6:00 AM. These discrepancies likely reflect multiple factors: study design differences, population genetics, and environmental influences. Singapore’s tropical climate with minimal day‑night temperature variation may affect circadian rhythms differently than Poland’s or Australia’s temperate climates.8,9 Additionally, ethnic composition differences across study populations may influence genetic predisposition to specific coronary event types. This differential timing carries significant clinical implications. It raises the possibility of chronotherapy, timing medications such as aspirin or P2Y12 inhibitors based on individual coronary anatomy and risk profiles to maximize protection during peak vulnerability periods. Moreover, emerging circadian medicine approaches targeting PER2 pathways through pharmacologic agents or intense light therapy could provide novel cardioprotective strategies, with the time‑of‑day administration being critical for therapeutic efficacy.1,32 Thus, further research should explore the mechanisms underlying this vessel‑specific circadian pattern to develop more personalized prevention strategies.1,2
Our study shows that onset time significantly affects treatment delays. Patient‑related delay (pain‑to‑FMC time) doubles for nocturnal‑onset STEMI, as compared with daytime events—a critical observation consistent with previous reports.4,5,11 Multiple factors contribute to this delay, including symptom misattribution, reluctance to disturb family or emergency services during night‑time hours, or delayed recognition when symptoms begin during sleep. This finding carries immediate practical implications, underscoring the need for public health campaigns emphasizing that chest pain constitutes a medical emergency at any hour and requires immediate action to preserve myocardial tissue. Additionally, the observed increase in system‑related delay (FMC‑to‑PCI) during morning hours, despite higher case volumes, suggests that health care systems continue to face operational challenges during the transition to standard working hours.14,15 These delays carry clinical significance, as each minute from symptom onset to reperfusion increases mortality risk.13 By examining the association between circadian onset timing and outcomes, we found that both onset hour and ischemic time independently predicted complications, but no significant interaction was detected. This indicates that prolonged delays are deleterious regardless of when the symptoms begin. Clinically, this highlights that while circadian timing influences patient behavior and cardiovascular pathophysiology, every additional minute of ischemia confers harm, reinforcing the universal urgency of timely reperfusion strategies. However, despite significant time‑of‑day variations in treatment delays, we observed no difference in periprocedural mortality—a finding consistent with some large‑scale analyses but contrasting with studies linking off‑hour presentation to worse outcomes.18,33-35 The ORPKI registry’s highly efficient national primary PCI network may sufficiently mitigate immediate mortality risk associated with extended ischemic times. However, periprocedural mortality represents only a short‑term end point. Extended ischemic times correlate with larger infarct size, strongly predicting long‑term adverse outcomes, including heart failure and subsequent mortality.13,33-38 Therefore, while immediate survival remains unaffected, increased nocturnal STEMI delays may still produce significant long‑term clinical consequences.
Limitations
This study has several limitations inherent to its retrospective, registry‑based design. First, symptom onset time relies on patient recall, which may be imprecise, particularly for nocturnal events, potentially introducing variability into the hourly data. Second, although the ORPKI registry is comprehensive, it does not capture all potential confounders of the circadian patterns, including sleep disorders (particularly sleep apnea, which is associated with nocturnal MI), medication timing, or psychosocial stressors. Third, our analysis did not account for nonthrombotic causes of STEMI, such as spontaneous coronary artery dissection, coronary vasospasm, or myocardial bridging, which may exhibit different circadian patterns than atherothrombotic events.12,39,40 Fourth, our analysis was limited to a single national population. Despite the large sample size, the findings may not extrapolate to other ethnic groups or health care systems, where regional variations in STEMI timing have been documented. Fifth, we assessed only periprocedural mortality. The absence of long‑term follow‑up data precludes evaluation of how treatment delays affect subsequent outcomes, including heart failure, reinfarction, or 1‑year mortality. Finally, our analysis used traditional STEMI criteria. The emerging occlusion MI paradigm identifies acute coronary occlusion in patients without classic ST‑segment elevation.13,41 Future studies should examine whether incorporating these patients alters the observed circadian patterns of onset time and culprit vessel distribution.
Conclusions
In conclusion, this large‑scale analysis confirms robust circadian variation in STEMI onset, peaking at 8:00 AM. Onset time significantly affects treatment delays, with patients with nocturnal events experiencing the longest times to intervention. Our novel finding of opposing circadian patterns for LAD vs RCA involvement suggests that time of day influences not only when but also where coronary thrombosis occurs. These findings highlight the critical role of chronobiology in understanding STEMI pathophysiology and optimizing delivery of acute coronary care.
- Eckle T, Bertazzo J, Khatua TN, et al. Circadian influences on myocardial ischemia‑reperfusion injury and heart failure. Circ Res. 2024; 134: 675‑694. | Crossref
- Rana S, Prabhu SD, Young ME. Chronobiological influence over cardiovascular function: the good, the bad, and the ugly. Circ Res. 2020; 126: 258‑279. | Crossref
- Thosar SS, Butler MP, Shea SA. Role of the circadian system in cardiovascular disease. J Clin Invest. 2018; 128: 2157‑2167. | Crossref
- Kanth R, Ittaman S, Rezkalla S. Circadian patterns of ST‑elevation myocardial infarction in the new millennium. Clin Med Res. 2013; 11: 66‑72. | Crossref
- Muller JE, Stone PH, Turi ZG, et al. Circadian variation in the frequency of onset of acute myocardial infarction. N Engl J Med. 1985; 313: 1315‑1322. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION