CTLA4, PTNP22, and FOXO3A gene variants as genetic biomarkers for co-occurrence of type 1 diabetes and autoimmune thyroid diseases in the Polish population
Key words: autoimmune thyroid disease, genetic factors, type 1 diabetes

 CC BY 4.0
CC BY 4.0
CTLA4, PTNP22, and FOXO3A gene variants as genetic biomarkers for co-occurrence of type 1 diabetes and autoimmune thyroid diseases in the Polish population
Introduction: Genetic predisposition is a common determinant of autoimmune endocrinopathies, particularly type 1 diabetes (T1D) and autoimmune thyroid disease (AITD). Although their coexistence is frequent, the underlying genetic background is not fully understood.
Objectives: We aimed to identify genetic polymorphisms predictive of an increased risk for co‑occurring T1D and AITD, and to assess their potential impact on glycemic control.
Patients and methods: We genotyped 5 selected polymorphisms (rs3087243 and rs231775 in the CTLA4 gene; rs12730735 in the PTPN22 gene; and rs2802292 and rs9400239 in the FOXO3A gene) in 277 patients with T1D. Clinical data on thyroid status, the presence of thyroid antibodies, treatment, and metabolic control were analyzed.
Results: Thyroid disorders, mostly Hashimoto hypothyroidism, were diagnosed in 32.9% of the patients. As many as 75% required L‑thyroxine (mean thyroid‑stimulating hormone level, 2.15 IU/l). Among thyroid peroxidase- and thyroglobulin‑positive patients, 81.6% and 75%, respectively, had a prior diagnosis of a thyroid disorder. The GG genotype of rs3087243 (CTLA4) conferred a higher risk of hypothyroidism and other thyroid diseases. The GG variant of rs2802292 (FOXO3A) was associated with a reduced prevalence of thyroid disease in family history. Carriers of the AG genotypes in rs3087243 and rs231775 (CTLA4), as well as the GG genotype in rs2802292 (FOXO3A), showed a lower probability of achieving diabetes control, particularly with longer disease duration. However, the CT genotype of rs12730735 (PTPN22) increased the likelihood of achieving glycemic control.
Conclusions: CTLA4 polymorphisms were associated with an elevated risk of a thyroid disease and poorer glycemic control; FOXO3A showed a dual role, that is, protective against familial thyroid disease but unfavorable for glycemic regulation; and the PTPN22 variant improved glycemic control. Genetic profiling may improve risk assessment and management in patients with T1D.
What's new?
This is the first study to demonstrate that selected CTLA4 variants not only increase the risk of thyroid autoimmunity in type 1 diabetes (T1D) but also influence long‑term glycemic control. We provide novel evidence that the rs2802292 variant of the FOXO3A gene, previously implicated in longevity, has dual effects. It is protective against familial thyroid disorders but impairs diabetes control. We identified a previously unreported role of the rs12730735 variant of the PTPN22 gene in improving metabolic control, which stresses its clinical and translational importance. These findings introduce new genetic determinants of the co‑occurrence of thyroid disease and T1D, expand current knowledge, and emphasize the added value of genetic profiling for personalized risk prediction and patient management.

Introduction
The incidence of autoimmune diseases has markedly increased in recent years. There is a growing assumption that the development of these conditions is influenced by the interplay between genetic and environmental factors. One of the characteristic features is the presence of autoantibodies that trigger cellular and humoral mechanisms, thus leading to organ or tissue destruction.
Epidemiologic studies have demonstrated a significant proportion of patients affected by multiple concomitant autoimmune disorders, including autoimmune thyroid diseases (AITD), type 1 diabetes (T1D), rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), multiple sclerosis, Sjögren syndrome, and celiac disease. Autoimmune diseases affect as much as 5%–10% of the global population and their prevalence is higher in women.1
Environmental exposures that may contribute to their development include viral and bacterial infections, drugs, stress, and diet.
Genetic predisposition is common across all autoimmune endocrinopathies, particularly T1D and AITD. The latter may occur before, after several years, or sometimes may be diagnosed simultaneously with T1D. The coexistence of T1D with AITD is classified as the autoimmune polyendocrine syndrome type 2 or type 3.
A cross‑sectional study found that the prevalence of AITD was 17%–30% in adult patients, out of whom 4%–18% presented simultaneously with T1D.2
Many studies have focused on identifying the genetic basis for the coexistence of these autoimmune diseases, with special attention paid to the cytotoxic T lymphocyte‑associated protein‑4 gene (CTLA4), the protein tyrosine phosphatase nonreceptor type‑22 gene (PTPN22), and the Forkhead box O‑3A gene (FOXO3A).
The CTLA4 gene
CTLA4 is a key immune checkpoint gene on chromosome 2 that is crucial for limiting T‑cell activation and preventing autoimmunity. Variants of CTLA4 are implicated in genetic susceptibility to T1D and AITD.3 Three polymorphisms of that gene are of particular interest, that is, rs231775 (+49A/G), where the G allele reduces CTLA4 inhibitory function, potentially enhancing T‑cell activation; rs3087243 associated with altered CTLA4 expression, and rs5742909 (318C/T) that may affect transcriptional activity (its link to T1D is less evident).
A meta‑analysis of 76 studies confirmed rs231775 as a potential biomarker for T1D, while rs231775 and rs3087243 increased the risk of T1D with AITD.4
The PTPN22 gene
The PTPN22 gene encodes a negative regulator of T‑cell signaling via lymphoid‑specific tyrosine phosphatase, maintaining immune tolerance by interacting with c‑Src tyrosine kinase and inhibiting T‑cell receptor pathways.5
Its 2 variants were assessed: 1) rs12730735 that alters Lyp function, reducing inhibition of T‑cell activation and promoting autoimmunity, and 2) rs2476601 (1865C>T, R620W) disrupting protein structure, which is strongly associated with T1D, RA, SLE, AITD, or psoriasis.6
While rs2476601 is extensively studied, rs12730735 has been linked to only a few autoimmune diseases but not to T1D together with AITD.6
The FOXO3A gene
FOXO3A regulates apoptosis, oxidative stress response, and immune homeostasis, particularly through the survival of T cells (Tregs). Its polymorphism may influence susceptibility to autoimmunity, although evidence is less robust than in the case of CTLA4 or PTPN22. Data suggest a potential role of FOXO3A variants in the coexistence of T1D and AITD, which warrants further research.7
CTLA4, PTPN22, and FOXO3A show similar mechanisms, such as checkpoint dysregulation, impaired Treg function, and altered T‑cell signaling that favor the coexistence of T1D with AITD.
The genetic characteristics of selected polymorphisms are given in Table 1.8,9
SNP | Risk | Alternative | Position (hg38) | HGVS | MAF | ClinVar submission accession | Risk factor |
Abbreviations: AITD, autoimmune thyroid disease; HGVS, Human Genome Variation Society; MAF, mutation annotation format; SNP, single‑nucleotide polymorphism; T1D, type 1 diabetes | |||||||
rs3087243 (CTLA4) | A | G | chr2:203874196 | NG_011502.1:g.11411G>A | 0.35 (EUR) | RCV001515646.7 | T1D, autoimmune diseases |
rs231775 (CTLA4) | G | A | chr2:203867991 | NG_011502.1:g.5206A>G | 0.45 (EUR) | RCV001255201.1 | T1D, autoimmunity |
rs12730735 (PTPN22) | T | C | chr1:113838835 | NG_007403.2:g.331+713T>C | 0.25 (EUR) | Not reported in ClinVar | Autoimmunity (AITD, regional) |
rs2802292 (FOXO3A) | T | G | chr6:108587315 | NG_158842.1:g.239G>T | 0.4 (EUR) | Not reported in ClinVar | Longevity, immune regulation |
rs9400239 (FOXO3A) | C | T | chr6:108656460 | NG_012124.2:g.62345C>T | 0.3 (EUR) | Not reported in ClinVar | Longevity, metabolic traits |
Figure 1 shows the conceptual relationship between the PTPN22, CTLA4, and FOXO3A genes (adapted from Stranford et al,10 Walker et al,11 and Hendrick et al12).
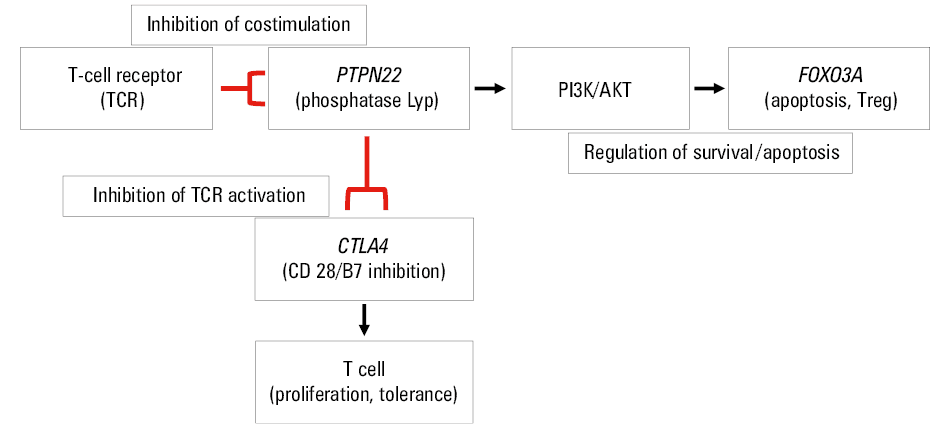
Abbreviations: AKT, protein kinase B; Lyp, lymphoid‑specific tyrosine phosphatase; PI3K, phosphoinositide 3‑kinase; Treg, regulatory T cells
This study was conceptualized to investigate genetic predisposition to autoimmune diseases through genetic profiling. Its primary objective was to identify predictive genetic biomarkers associated with T1D and AITDs. The CTLA4, PTPN22, and FOXO3A gene variants were selected based on their established roles in immune regulation, autoimmunity, and metabolic homeostasis—pathways central to both T1D and AITD. However, previous studies investigating their involvement in the coexistence of T1D and AITD had yielded inconsistent and incomplete results. The genetic homogeneity of our study population provided a favorable context for clarifying these associations and reducing potential confounding due to population stratification. Together, these loci represent a biologically plausible network of immune and metabolic regulators potentially underlying the coexistence of T1D and AITD.
The aim of the present study was to further evaluate the clinical relevance of selected genetic polymorphisms previously identified in this cohort by assessing their association with the risk of co‑occurrence of T1D and AITD, as well as their impact on glycemic control.
Patients and methods
Patient cohort
The study protocol was approved by the Bioethics Committee of the Medical University of Silesia, Poland (PCN/0022/KB1/104/19). All eligible candidates provided written informed consent to participate in the study. The study group consisted of 277 adults with T1D treated at the Department of Internal Medicine, Diabetology and Nephrology, and at the Diabetes Outpatient Clinic, Medical University of Silesia (Zabrze, Poland).
Demographic, anthropometric, and environmental data of the patients were collected, including sex, age, body weight, height, a history of diabetes therapy, other comorbidities, and medication use. The study participants also provided information about their smoking habits, alcohol consumption, physical activity, diet, COVID‑19 vaccinations, and a history of SARS‑CoV‑2 infection. Gynecological data were collected from the female participants, and the information on their offspring was obtained from all the patients. The same study population and the frequencies of same genetic variants have been already published.13
The exclusion criteria were other types of diabetes and / or a lack of consent to participate in the study.
Biochemical and genetic analyses
A venous blood sample (2 × 4.9 ml) was collected from each participant, and glycated hemoglobin (HbA1c) was assayed using high‑performance liquid chromatography. Other blood tests included thyroid‑stimulating hormone (TSH), thyroid peroxidase (TPO) antibodies (TPOAbs), and thyroglobulin antibodies (TGAbs). TPOAbs and TGAbs were considered positive if their levels were above 30 IU/ml and 4.11 IU/ml, respectively.
Gene and single‑nucleotide polymorphisms (SNPs) related to autoimmune diseases were selected through an extensive search of the literature and the bioinformatics database (http://www.ncbi.nlm.nih.gov/snp/). As a result, 2 SNP loci in the CTLA4 gene (rs3087243 and rs231775), 1 SNP locus in the PTPN22 gene (rs12730735), and 2 SNP loci in the FOXO3A gene (rs2802292, rs9400239) were selected. TaqMan probes (Thermo Fisher Scientific, Vacaville, California, United States) were used in the SNP tests.
DNA isolation was performed using the RBC kit, where red blood cells were separated from the whole blood, collected into EDTA tubes and frozen at –20 °C. The MagCore Genomic DNA Whole Blood Kit (RBC Bioscience Corp., New Taipei City, Taiwan) of the MagCore isolation system was used to perform genetic studies. The material was used for genetic tests (allelic discrimination of the CTLA4, PTPN22, and FOXO3A polymorphisms).
Genomic DNA was isolated using the DNA isolation MagCore Genomic DNA Whole Blood Kit in accordance with the manufacturer’s instructions. SNP allelic discrimination was performed using real‑time fluorescence‑based quantitative polymerase chain reaction (ROCHE LifeCycler 96, Roche Diagnostics International Poland, Warszawa, Poland). Two blank control samples were placed in each 96‑well plate for quality control. Five genotypes were determined in each patient, and their prevalence rates were established.
Statistical analysis
Statistical analysis was performed using the R language in R Studio (2024.04.2+764.pro1; Boston, Massachusetts, United States). Qualitative variables were presented as the number of cases and percentage, whereas quantitative variables were presented as mean and SD for variables with a normal distribution, and as median with interquartile range (IQR) for variables with a non‑normal distribution. The normality of variable distribution was assessed using histograms and QQ plots generated in the R Studio. The relationships among variables were evaluated using χ2 tests for categorical variables. The t test was applied for continuous variables whose distribution was close to normal, while the Wilcoxon rank‑sum test was conducted for continuous variables with non‑normal distribution. A P value below 0.05 was considered significant.
The distribution of alleles was checked for compliance with the Hardy‑Weinberg equilibrium by comparing their actual distribution with the expected distribution, using the χ2 test. The proportion test was used to compare the allele distribution in the study population to that in the Central European population.
Single‑factor logistic regression models were used to examine the effect of allele variants on the occurrence of specific traits. The analysis of variance (ANOVA) was performed to evaluate the impact of variants on continuous variables.
To assess the impact of genetic variants on selected polymorphisms, multivariable logistic regression models were constructed and considered the interaction between sex and the variant. Additionally, to evaluate the effect of variants on glycemic control, multivariable logistic regression models were applied according to disease duration. These models included the interactions between the genetic variants and disease duration.
Results
The general characteristics of the study group are given in Table 2, with a more detailed description published elsewhere.13 The study group included 277 patients with T1D (65.7% women), at a mean age of 33.13 (12.47) years, and median duration of T1D 12 (4–19) years. As many as 59.5% of the patients were treated with multiple daily insulin injections and 58.8% used continuous glucose monitoring systems. Mean HbA1c level was 8.16%, with no sex‑related differences among the groups. Chronic diabetes complications and other comorbidities were also assessed. Thyroid disorders were found in 32.8% of the patients (median duration, 8 [2–11] y). The most prevalent thyroid disorder was hypothyroidism associated with autoimmune thyroiditis (Hashimoto disease [HD]). As many as 75% of the patients with thyroid disorders (median TSH level, 2.15 [1.22–2.38] IU/l) were on L‑thyroxine supplementation. TPOAbs and TGAbs were measured in all participants to identify individuals with autoimmune thyroiditis. A total of 81.6% and 75% of the patients positive for TPOAbs and TGAbs, respectively, had been already diagnosed with a thyroid condition. The patients with HD and hypothyroidism presented with significantly higher levels of TSH (Supplementary material, Table S1).
Parameter | Value | |
Continuous variables are presented as mean (SD) for normally distributed data or median (interquartile range) for non‑normal distribution. Categorical variables are presented as number and percentage.
Abbreviations: BMI, body mass index; CGM, continuous glucose monitoring; CSII, continuous subcutaneous insulin infusion; HbA1c, glycated hemoglobin; MDI, multiple daily injection; TGAb, thyroglobulin antibody; TPOAb, thyroid peroxidase antibody; TSH, thyroid‑stimulating hormone; others, see Table 1 | ||
Sex | Women | 182 (65.7) |
Men | 95 (34.3) | |
Age, y | 33.13 (12.47) | |
BMI, kg/m² | 24.45 (4.35) | |
T1D duration, y | 12 (4–19) | |
T1D treatment | MDIs | 165 (59.6) |
CSII | 165 (59.6) | |
CGM use | 163 (58.8) | |
HbA1c, % | 8.15 (2.04) | |
Chronic diabetes complications | Retinopathy | 58 (20.9) |
Nephropathy | 16 (5.7) | |
Neuropathy | 32 (11.5) | |
Thyroid diseases | Any thyroid disease | 91 (32.8) |
Graves disease | 4 (4.4) | |
Hypothyroidism | 73 (80.2) | |
Hashimoto disease | 58 (63.3) | |
Nodular goiter | 18 (19.8) | |
Thyroid disease duration, y | 6 (2–11) | |
L‑thyroxin therapy | Yes | 69 (75.8) |
Dose, µg/day | 75 (50–100) | |
Thyroid hormone levels | TSH, µIU/ml | 1.76 (1.22–2.38) |
TPOAb, IU/ml | 14.98 (10.77–39.85) | |
TGAb, IU/ml | 1.87 (1.02–11.98) | |
Other diseases | Ulcerative colitis | 3 (1.1) |
Atopic dermatitis | 31 (11.2) | |
Asthma | 12 (4.3) | |
Other allergies | 31 (11.2) | |
Irritable bowel syndrome | 7 (2.5) | |
Hypertension | 53 (19.1) | |
Ischemic heart disease | 7 (2.5) | |
Dyslipidemia | 14 (5) | |
Family history | Thyroid diseases | 97 (35) |
Diabetes (T1D, T2D) | 163 (58.8) | |
The prevalence of other autoimmune diseases was also assessed, with vitiligo and celiac disease being the most common disorders. No sex‑related differences were found in terms of body mass index, glycemic control, HD, or hypothyroidism rates (Supplementary material, Table S2). The study found that patients using continuous subcutaneous insulin infusion had lower levels of HbA1c (P <0.001). The use of glucose monitoring systems also resulted in lower HbA1c concentrations (P = 0.02; Supplementary material, Table S3).
The allele and genotype frequencies of the polymorphisms are given in Table 3.
Variable | N (%) | 95% CI | HWE P value | |
a In a small number of samples, genotyping of all analyzed variants was unsuccessful due to isolated assay failures or suboptimal sample quality.
Abbreviations: HWE, Hardy–Weinberg equilibrium | ||||
CTLA4 rs3087243 | AA | 25 (9.2) | 5.8–12.6 | 0.36 |
AG | 127 (46.5) | 40.6–52.4 | ||
GG | 121 (44.3) | 38.5–50.2 | ||
CTLA4 rs231775 | AA | 76 (27.84) | 22.5–33.2 | 0.55 |
AG | 141 (51.6) | 45.8–57.5 | ||
GG | 56 (20.5) | 17.7–25.3 | ||
PTPN22 rs12730735 | TT | 150 (54.9) | 49.1–60.8 | 0.68 |
CT | 107 (39.2) | 33.4–44.9 | ||
CC | 16 (5.9) | 3.1–8.6 | ||
FOXO3A rs2802292 | TT | 80 (29.2) | 23.8–34.5 | 0.13 |
GT | 148 (54) | 48.1–59.9 | ||
GG | 46 (16.8) | 12.4–21.2 | ||
FOXO3A rs9400239 | CC | 104 (38.1) | 32.4–43.8 | 0.13 |
CT | 141 (51.6) | 45.8–57.5 | ||
TT | 28 (10.3) | 6.7–13.8 | ||
The distribution of genotype frequencies was consistent with the Hardy‒Weinberg equilibrium (P >0.01). Our study found a significant difference between the allele distribution of the rs3087243 polymorphisms of the CTLA4 gene and the distribution reported in the Central European population. We found no differences in the distribution of the other polymorphisms as compared to the Central European population (Table 4). The univariate logistic regression analysis showed that the GG variant of the rs3087243 polymorphism in the CTLA4 gene was significantly associated with higher likelihood of thyroid diseases, hypothyroidism, and significantly lower odds of atopic dermatitis. No significant impact of the rs231775 variant of the CTLA4 gene on the occurrence of the analyzed traits was observed.
Variable | Frequency in the study population, % | 95% CI | Frequency in the general population (CE)a, % | P value | |
a Ensembl (CEU) – public genome database; allele frequency data for the Central European (CEU) population
Abbreviations: CE, Central Europe | |||||
CTLA4 rs3087243 | A | 33 | 27.5–38.5 | 48 | 0.04 |
G | 67 | 61.5–72.5 | 52 | ||
CTLA4 rs231775 | A | 54 | 48.1–59.9 | 63 | 0.25 |
G | 46 | 40.1–51.9 | 37 | ||
PTPN22 rs12730735 | C | 25 | 19.9–30.1 | 29 | 0.63 |
T | 75 | 69.9–80.1 | 71 | ||
FOXO3A rs2802292 | G | 44 | 38.1–49.8 | 35 | 0.25 |
T | 56 | 50.1–61.8 | 65 | ||
FOXO3A rs9400239 | T | 36 | 30.3–41.6 | 27 | 0.22 |
C | 64 | 58.3–69.6 | 73 | ||
The GG variant of the rs2802292 polymorphism in the FOXO3A gene was linked to significantly reduced prevalence of thyroid disease in family history (Table 5).
Gene | Disease | Genotype | No, n (%) | Yes, n (%) | OR (95% CI) | P value |
Abbreviations: OR, odds ratio | ||||||
CTLA4 rs3087243 | Atopic dermatitis | AA | 22 (8.3) | 3 (37.5) | 1 | – |
AG | 122 (46.2) | 4 (50) | 0.24 (0.05–1.29) | 0.07 | ||
GG | 120 (45.4) | 1 (12.5) | 0.06 (0–0.5) | 0.02 | ||
CTLA4 rs3087243 | Thyroid disease | AA | 21 (11.5) | 4 (4.4) | 1 | – |
AG | 86 (47.2) | 41 (45) | 2.5 (0.88–8.99) | 0.11 | ||
GG | 75 (41.2) | 46 (50.5) | 3.22 (1.14–11.56) | 0.04 | ||
CTLA4 rs3087243 | Hypothyroidism | AA | 3 (16.7) | 1 (1.8) | 1 | – |
AG | 9 (50) | 32 (43.8) | 10.67 (1.2–230.88) | 0.05 | ||
GG | 6 (33.3) | 40 (54.8) | 20 (2.18–444.11) | 0.02 | ||
PTPN22 rs12730735 | Hepatic diseases | TT | 129 (52.6) | 20 (74) | 1 | – |
CC | 14 (5.7) | 2 (7.4) | 0.92 (0.14–3.64) | 0.92 | ||
CT | 102 (41.6) | 5 (18.5) | 0.32 (0.1–0.81) | 0.03 | ||
FOXO3 rs2802292 | Family history of thyroid disease | TT | 46 (26.44) | 34 (35.05) | 1 | – |
GG | 37 (21.26) | 9 (9.28) | 0.33 (0.13–0.75) | 0.01 | ||
GT | 91 (52.3) | 54 (55.67) | 0.8 (0.46–1.4) | 0.44 | ||
The ANOVA did not show any correlation between the gene variants and T1D duration or obesity.
The impact of genetic variants in the analyzed genes on glycemic control (using HbA1c of 6.5% as a threshold) was also assessed with consideration given to disease duration (below and above 5 y). The multivariable logistic regression model showed that patients with the AG variant of the rs3087243 polymorphism of the CTLA4 gene and with the AG variant of the rs231775 polymorphism of the CTLA4 gene had significantly lower likelihood of achieving glycemic control, particularly with longer disease duration. Similarly, the combined presence of the GG variant of the rs2802292 polymorphism of the FOXO3A gene and a longer duration of T1D reduced the likelihood of achieving glycemic control. On the other hand, the CT variant of the rs12730735 polymorphism in the PTPN22 gene increased the probability of achieving better glycemic control (Table 6).
Variable | OR | SE | 95% CI | P value |
CTLA4 rs3087243 AG | 0.462 | 0.789 | 0.094–2.247 | 0.38 |
CTLA4 rs3087243 GG | 0.214 | 0.838 | 0.039–1.126 | 0.06 |
TD1 >5 y | 0.063 | 1.25 | 0.003–0.56 | 0.03 |
CTLA4 rs3087243AG, T1D >5 y | 7.027 | 1.328 | 0.655–176.244 | 0.14 |
CTLA4 rs3087243GG, T1D >5 y | 8.615 | 1.374 | 0.727–229.149 | 0.12 |
CTLA4 rs231775AG | 0.462 | 0.789 | 0.094–2.247 | 0.33 |
CTLA4 rs231775GG | 0.214 | 0.838 | 0.039–1.126 | 0.07 |
T1D >5 y | 0.063 | 1.25 | 0.003–0.56 | 0.03 |
CTLA4 rs231775AG, T1D >5 y | 7.027 | 1.328 | 0.655–176.244 | 0.14 |
CTLA4 rs231775GG, T1D >5 y | 8.615 | 1.374 | 0.727–229.149 | 0.12 |
PTPN22 rs12730735CT | 3.079 | 0.531 | 1.106–9.049 | 0.03 |
PTPN22 rs12730735CC | 1.5 | 1.219 | 0.069–13.596 | 0.74 |
T1D >5 y | 0.685 | 0.485 | 0.269–1.842 | 0.43 |
PTPN22 rs12730735CT, T1D >5 y | 0.328 | 0.693 | 0.082–1.257 | 0.11 |
PTPN22 rs12730735CC, T1D >5 y | 0.398 | 1.63 | 0.011–13.427 | 0.57 |
FOXO3A rs2802292GT | 1.022 | 0.593 | 0.324–3.423 | 0.97 |
FOXO3A rs2802292GG | 2.375 | 0.715 | 0.583–9.984 | 0.23 |
T1D >5 y | 0.884 | 0.571 | 0.295–2.856 | 0.83 |
FOXO3A rs2802292GT, T1D >5 y | 0.402 | 0.748 | 0.09–1.722 | 0.22 |
FOXO3A rs2802292GG, T1D >5 y | 0.101 | 1.073 | 0.01–0.745 | 0.03 |
FOXO3A rs9400239CT | 0.908 | 0.533 | 0.322–2.656 | 0.86 |
FOXO3A rs9400239TT | 0.594 | 1.195 | 0.028–4.856 | 0.66 |
T1D >5 y | 0.528 | 0.515 | 0.194–1.493 | 0.21 |
FOXO3A rs9400239CT, T1D >5 y | 0.59 | 0.695 | 0.147–2.28 | 0.45 |
FOXO3A rs9400239TT, T1D >5 y | 0.344 | 1.6 | 0.01–11.159 | 0.5 |
The analysis of genotype associations with the presence of autoimmune diseases showed significant differences for CTLA4 rs3087243 and FOXO3A rs2802292.
Regarding CTLA4 rs3087243, the prevalence of autoimmune diseases was 32% in AA homozygotes, 56.7% among AG heterozygotes, and reached 60.3% in GG homozygotes (P = 0.04). This finding suggests that the G allele may increase susceptibility to autoimmune diseases.
Considering FOXO3A rs2802292, a significant increase in the risk of autoimmune diseases was observed with an increasing number of T alleles—autoimmune diseases occurred in 41.3% of the patients with the GG genotype, 58.1% in GT heterozygotes, and 61.3% in TT homozygotes (P = 0.03). These results indicate that the T allele may contribute to the development of autoimmune diseases.
In the case of CTLA4 rs231775, the percentage of patients with autoimmune diseases ranged from 51.8% (GG) to 59.9% (AG). However, the differences did not reach statistical significance (P = 0.14). Similarly, regarding PTPN22 rs12730735 (P = 0.45) and FOXO3A rs9400239 (P = 0.13), no significant associations were observed, with some trends suggesting a higher risk in specific genotypes (Table 7). The summary of the study findings is presented in Table 8.
SNP | Genotype | Lack of autoimmune disease | Presence of autoimmune disease | Total, n | Percentage of autoimmune diseases | P valuea |
a χ2 test
Abbreviations: see Table 1 | ||||||
CTLA4 rs3087243 | AA | 17 | 8 | 25 | 32 | 0.04 |
AG | 55 | 72 | 127 | 56.7 | ||
GG | 48 | 73 | 121 | 60.3 | ||
CTLA4 rs231775 | AA | 36 | 40 | 76 | 52.6 | 0.14 |
AG | 57 | 85 | 142 | 59.9 | ||
GG | 27 | 29 | 56 | 51.8 | ||
PTPN22 rs12730735 | CC | 9 | 7 | 16 | 43.7 | 0.45 |
CT | 47 | 60 | 107 | 56.1 | ||
TT | 64 | 86 | 150 | 57.3 | ||
FOXO3A rs2802292 | GG | 27 | 19 | 46 | 41.3 | 0.03 |
GT | 62 | 86 | 148 | 58.1 | ||
TT | 31 | 49 | 80 | 61.2 | ||
FOXO3A rs9400239 | CC | 45 | 59 | 104 | 56.7 | 0.13 |
CT | 60 | 81 | 141 | 57.4 | ||
TT | 14 | 14 | 28 | 50 | ||
Gene / SNP | Genotype | Clinical association | Direction / effect |
a Diabetes control is defined as HbA1c ≤6.5%, longer T1D duration refers to >5 years of the disease.
| |||
CTLA4 rs3087243 | GG | Thyroid diseases (AITD, hypothyroidism) | ↑ Risk |
AA | Autoimmune diseases | ↓ Risk | |
GG | Atopic dermatitis | ↓ Risk | |
CTLA4 rs231775 | AG | Diabetes control (HbA1c ≤6.5%) | ↓ Likelihood (longer T1D duration) |
PTPN22 rs12730735 | CT | Diabetes control | ↑ Likelihood of better control |
FOXO3A rs2802292 | GG | Family history of thyroid disease | ↓ Risk |
GG | Autoimmune diseases | ↓ Risk | |
FOXO3A rs9400239 | – | Autoimmune diseases | No significant association |
Discussion
The co‑occurrence of T1D with AITD is relatively common due to shared autoimmune mechanisms. There are several genes and genetic markers that are primarily involved in immune regulation, antigen presentation, and autoimmunity.14 The genetic markers include the human leukocyte antigen (HLA) region (HLA‑DR3‑5),15,16 HLA antigens (DQ2 and DQ8),17,18 as well as non‑HLA functional SNP of various genes, such as CTLA4, PTPN22, interleukin‑2 receptor (IL2Ra), vitamin D receptor (VDR), and tumor‑necrosis‑factor α (TNF-α).19,20 Other genes were associated with T1D and AITD and included the cluster of differentiation‑40 (CD40), the FOXP3, an insulin variable number of tandem repeats (INS‑VNTR), the MHC class I polypeptide‑related sequence A (MICA), the C‑type lectin domain containing 16A (CLEC16A), the Erb‑B2 receptor tyrosine kinase 3 (ERBB3), and the interferon‑induced helicase C domain‑containing protein 1 (IFIH1) gene.18-21
In our study, 277 patients were evaluated for the co‑occurrence of T1D and other autoimmune diseases, with a particular focus on AITD (the most prevalent co‑occurring condition).
Similarly to previous studies, thyroid diseases were the most prevalent autoimmune conditions in the population of patients with T1D, affecting 32.8% of the participants. The most frequently observed thyroid disorder was HD. The presence of thyroid antibodies correlated with significantly higher TSH levels, and over 20% of the patients were newly diagnosed with thyroid disease.
Previous studies have shown that the prevalence of T1D co‑occurring with other autoimmune diseases varied by sex, age, ethnicity, and diabetes duration (ranging from 18.3% to 27%), with AITD being the most prevalent co‑occurring condition.22 Recent Polish studies have also highlighted that the duration of T1D may influence the development of subclinical target organ damage and metabolic complications.23,24 In a Finnish study, 1 in 5 patients with T1D had another autoimmune disease,25 while in the United States, this association was observed in 1 out of 4 individuals.26 Both these studies were conducted primarily in white populations.
A 2024 Mendelian randomization study also confirmed a genetic association between T1D and AITD (odds ratio [OR], 1.27; 95% CI, 1.11–1.46; P <0.001).27 Our study demonstrated a significant difference in the distribution of alleles of the CTLA4 gene rs3087243 polymorphism, as compared with the general population. Specifically, the GG variant of this polymorphism was associated with an increased risk of thyroid disease.
Similar to our findings, Howson et al28 investigated the CTLA4 gene in a large cohort (>4000) of British patients with T1D, stratifying them by either the presence or the absence of TPOAbs. They found an association between the rs3087243 variant of the CTLA4 gene (OR, 1.49 for allele G; 95% CI, 1.29–1.72) and the group positive for TPOAbs in comparison with the TPOAb‑negative group (OR, 1.16; 95% CI, 1.1–1.24).28
In the Asian (Japanese) population, the rs3087243(G) allele was associated with a 1.3‑fold increased risk of AITD and a 1.5‑fold increased risk of T1D. No association was observed between the SNP and T1D in patients without AITD, which suggests that previously reported links between rs3087243 and T1D may have largely reflected the association between rs3087243 and AITD.29 Another Japanese study also suggested a strong association between the CTLA4 gene polymorphisms and AITD, with a high prevalence rate of AITD in patients with T1D.30
Apart from the British study,28 our study is the only one assessing the rs3087243 polymorphism of the CTLA4 gene in white patients with T1D and a genetic predisposition to the co‑occurrence of T1D with thyroid diseases in the carriers of the GG variant.
Regarding the rs231775 variant of the CTLA4 gene, the allele distribution in our study was not significantly different from that reported in the general population, and no similar association was found between that variant and any thyroid disease or other autoimmune disease. However, the CT variant of rs231775 was associated with poorer glycemic control, particularly among the patients with diabetes duration of over 5 years. This association suggests that genetic variation in immune checkpoint regulation may influence long‑term metabolic outcomes.
In a study on the Indian population, the authors analyzed 84 patients with hypothyroidism and 62 controls from Gujarat, India.31 The rs231775 polymorphism in the CTLA4 gene was associated with a higher risk of autoimmune hypothyroidism: ORs for AA were 5.33 for AG (95% CI, 2.04–13.92; P = 0.0004) and 5.78 for GG (95% CI, 1.83–18.25; P = 0.0004). However, the study involved a relatively small cohort and was conducted in a genetically distinct population, which may account for differences with other studies.
In another study conducted on a group of Polish children with AITD and T1D, Borysewicz‑Sańczyk et al32 evaluated selected SNPs, including the CTLA4 gene. Significant differences were observed in CTLA4 (rs231775 G>A) alleles between the patients with T1D and the control group. The GG genotype in rs231775 in the CTLA4 gene was significantly more common in the patients with T1D. However, no association with AITD was found among Polish children and adolescents, which is in line with our findings.
No studies have examined the association between the PTPN22 gene variant (rs12730735) and the co‑occurrence of T1D with AITD. Data from the studies involving patients with other autoimmune diseases are limited.33,34 In our work, the distribution of alleles for the gene variant did not differ from the distribution in the general population. However, the CT variant of rs12730735 was associated with significantly better glycemic control.
Recently, the FOXO3A gene and its variants have become a focus of research considering longevity, obesity, bipolar disorder, and autoimmune diseases, such as vitiligo and HD.35-39
We examined 2 FOXO3A gene variants (rs2802292 and rs9400239), and found no differences in the allele distribution, as compared to that in the general population. Notably, the rs2802292 polymorphism in the FOXO3A gene has not previously been studied in patients with autoimmune diseases. Our findings indicate that individuals homozygous for the GG variant of rs2802292 in the FOXO3A gene showed a significantly lower prevalence of a family history of thyroid disease. This suggests that this polymorphism may exert a protective effect. Given that FOXO3A regulates immune homeostasis, oxidative stress responses, and T‑cell activity, the GG genotype could enhance transcriptional activity, favoring immune tolerance, thereby reducing familial clustering of thyroid autoimmunity. Clinically, this finding indicates that individuals with this variant might have a lower baseline risk, although environmental triggers and other genetic factors may be involved.
There are insufficient data on the FOXO3A gene polymorphism rs9400239.
Only a single study40 on patients with HD found a higher prevalence rate of the TT variant of rs9400239 in patients with HD vs healthy individuals (16.5% vs 9.3%; P = 0.06). Furthermore, T allele presence for rs9400239 was more common in patients with HD than the control group (39.9% vs 31.4%; OR, 1.45; 95% CI, 1.1–1.91; P = 0.02). The authors stressed a potential association between FOXO3A and the pathogenesis of AITD.
These results are supported by analyses showing significant associations between specific genetic variants and the prevalence of autoimmune diseases. In particular, the G allele of CTLA4, rs3087243, and the T allele of FOXO3A, rs2802292, were associated with an increased risk of autoimmune diseases, with the risk increasing progressively with the number of alleles (CTLA4 rs3087243: AA → AG → GG, 32% → 56.7% → 60.3%; FOXO3A rs2802292: GG → GT → TT, 41.3% → 58.1% → 61.3%).
In conclusion, genetic markers, particularly the functional variants of selected genes, such as CTLA4, PTPN22, and FOXO3A, play a significant role in understanding the co‑occurrence of T1D with other autoimmune diseases. Our study provides new insights into the association of specific polymorphisms with an increased risk of T1D and AITD. The most notable finding is the identification of the rs3087243 polymorphism of the CTLA4 gene and the demonstration that its GG variant is associated with a higher risk of AITD. Another important finding is that the GG variant (rs2802292) in the FOXO3A gene may potentially reduce the risk of developing thyroid disease.
The observed associations may reflect the functional roles of these polymorphisms in immune regulation and metabolic stress response. CTLA4 variants (rs3087243 and rs231775) modulate T‑cell activation, and the carriers of the AG genotype may present with persistent low‑grade autoimmunity, impairing long‑term glycemic control, particularly with prolonged disease duration. Similarly, the GG genotype of rs2802292 in the FOXO3A gene, involved in oxidative stress response, may influence insulin sensitivity. Variants in this gene may alter the expression of genes regulating gluconeogenesis, insulin signaling, and stress resistance. The GG genotype could lead to impaired cellular adaptation to chronic hyperglycemia or oxidative stress in long‑standing T1D, which reduces insulin sensitivity and limits the ability to maintain optimal glycemic control. However, the CT variant of rs12730735 in PTPN22 encodes a key negative regulator of T‑cell signaling. Variants in this gene influence the threshold for T‑cell activation and autoimmune reactivity. The CT genotype might reduce excessive immune activation, thereby lowering autoimmune‑mediated inflammation. This attenuation could reduce insulin resistance linked to systemic inflammation, leading to better metabolic stability and improved glycemic control.
This study has several limitations. The sample size could have been larger, which might have improved the ability to detect other genetic effects. The selected polymorphisms within the CTLA4, PTPN22, and FOXO3A genes seem to be the most relevant for our study, but other polymorphisms within these genes were not investigated.
In summary, the use of a genetic panel based on the identified variants seems particularly useful for identifying T1D patients with an increased or decreased risk of AITD, which may have significant implications for personalized treatment. Early identification of individuals from risk groups could support more targeted monitoring of thyroid function and antibody levels, enabling earlier diagnosis and treatment of thyroid disorders.
Some of the investigated polymorphisms have not previously been studied in relation to the co‑occurrence of autoimmune diseases, which is a significant contribution to current knowledge. Another strength of the study is the ethnic homogeneity of the cohort, which minimizes the risk of population stratification bias and thereby reinforces the reliability of the analyses. From a clinical perspective, incorporating genetic information into patient assessment may facilitate individualized monitoring plans, more accurate risk stratification, and tailored preventive or therapeutic strategies. Patients carrying high‑risk alleles (eg, CTLA4 rs3087243GG or FOXO3A rs2802292T alleles) can be identified as having increased susceptibility to AITD. These patients could benefit from earlier and more frequent thyroid function tests and antibody screenings, allowing timely diagnosis and treatment of thyroid dysfunction before clinical symptoms appear. Variants affecting glycemic control (eg, CTLA4 rs3087243AG, rs231775AG, and FOXO3A rs2802292GG in patients with longer disease duration) may indicate individuals at a risk of poorer glycemic outcomes. Clinicians could implement frequent monitoring of HbA1c, consider more intensive insulin therapy, or adopt advanced glucose monitoring systems or hybrid‑closed loop pumps for these patients. Knowledge of protective variants (eg, PTPN22 rs12730735CT) allows for identification of patients likely to achieve better glycemic control, potentially reducing unnecessary interventions. Furthermore, better understanding of the functional significance of the genetic variants opens the prospect of implementing genotype‑tailored therapies, which in the future may translate into more precise and effective treatment of coexisting autoimmune disease.
- Li Q, Yang W, Li J, Shan Z. Emerging trends and hot spots in autoimmune thyroiditis research from 2000 to 2022: a bibliometric analysis. Front Immunol. 2022, 13: 953465. | Crossref
- Kahles H, Fain PR, Baker P, et al. Genetics of autoimmune thyroiditis in type 1 diabetes reveals a novel association with DPB1*0201: data from the type 1 diabetes genetics consortium. Diabetes Care. 2015; 38: S21‑S28. | Crossref
- Hossen MM, Ma Y, Yin Z, et al. Current understanding of CTLA‑4: from mechanism to autoimmune diseases. Front Immunol. 2023; 14: 1198365. | Crossref
- Chen M, Li S. Associations between cytotoxic T‑lymphocyte‑associated antigen 4 gene polymorphisms and diabetes mellitus: a meta‑analysis of 76 case‑control studies. Biosci Rep. 2019; 39: BSR20190309. | Crossref
- Brownlie RJ, Zamoyska R, Salmond RJ. Regulation of autoimmune and anti‑tumour T‑cell responses by PTPN22. Immunology. 2018; 154: 377‑382. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION