Direct oral anticoagulants in patients with venous thromboembolism: current challenges in everyday practice
Key words: anticoagulation management, direct oral anticoagulants, factor Xa inhibitors, special populations, venous thromboembolism

 CC BY 4.0
CC BY 4.0
Direct oral anticoagulants in patients with venous thromboembolism: current challenges in everyday practice
Direct oral anticoagulants (DOACs) have transformed venous thromboembolism (VTE) treatment by offering predictable pharmacokinetics and eliminating routine monitoring requirements. Despite robust clinical trial evidence supporting their efficacy, real‑world implementation continues to present challenges in special populations. This review synthesizes recent evidence on DOAC usage in VTE patients, with emphasis on current challenges encountered in everyday clinical practice, including special populations, treatment adherence, bleeding management, and emerging dosing strategies. A literature search was conducted across PubMed, MEDLINE, and Cochrane databases for peer‑reviewed articles published in the last 5 years using the following search terms: “direct oral anticoagulants,” “DOACs,” “venous thromboembolism,” “VTE,” “deep vein thrombosis,” and “pulmonary embolism.” Inclusion criteria prioritized randomized controlled trials, meta‑analyses, systematic reviews, and observational studies. Current evidence demonstrates DOACs as first‑line therapy for most VTE patients, with clinical challenges remaining in patients with obesity, severe renal impairment, cancer‑associated thrombosis, and unusual site thrombosis. Network meta‑analyses reveal comparable efficacy among DOACs, with apixaban demonstrating favorable bleeding profiles. Adherence significantly impacts outcomes, with consistently high adherence reducing recurrent VTE risk. Reversal agents have improved management of DOAC‑associated bleeding. DOACs represent the standard of care for VTE treatment, with increasing real‑world evidence supporting their safety and efficacy. Clinicians must navigate persistent challenges in special populations through individualized risk‑benefit assessment. Encouraging physicians to focus both on patient education to optimize adherence and on provider awareness of emerging evidence on dose modifications and reversal strategies is imperative to proper and effective implementation of DOACs in these groups.
Introduction
Venous thromboembolism (VTE) is a leading cause of mortality, in North America ranking as the third and fifth most common cause of cardiovascular‑related and all‑cause mortality, respectively.1 Encompassing several subtypes, such as deep vein thrombosis (DVT) and pulmonary embolism (PE), VTE represents a significant global health burden with an annual incidence of approximately 1–2 per 1000 adults.2,3 Traditional anticoagulation was achieved with vitamin K antagonists (VKAs), which, while effective, require frequent monitoring, have drug‑food interactions, and demonstrate interpatient variability in dose response.4 These limitations invited the development of direct oral anticoagulants (DOACs), which have fundamentally transformed VTE management over the past decade.
Direct oral anticoagulants
What are direct oral anticoagulants?
DOACs represent medications that directly inhibit specific coagulation factors without requiring cofactors.5,6 Unlike VKAs, which affect multiple vitamin K–dependent cofactors, DOACs target single components of the coagulation cascade; activated factor X (FXa; targeted by rivaroxaban, apixaban, and edoxaban) and thrombin / FIIa (targeted by dabigatran).7 This targeted approach provides predictable anticoagulation with fixed dosing, rapid onset, and elimination of routine laboratory monitoring.8,9
History and development
FXa is an ideal therapeutic target for anticoagulation, positioned at the convergence of both intrinsic and extrinsic coagulation pathways, with each FXa molecule generating approximately 1000 molecules of thrombin.
The landmark EINSTEIN trials (Oral Rivaroxaban for Symptomatic Venous Thromboembolism) established rivaroxaban’s efficacy for VTE treatment, demonstrating noninferiority to standard therapy (enoxaparin followed by VKAs).10 Subsequently, the AMPLIFY trial (A Safety and Efficacy Trial Evaluating the Use of Apixaban in the Treatment of Symptomatic Deep Vein Thrombosis and Pulmonary Embolism) showed apixaban’s effectiveness with reduced bleeding, as compared with conventional therapy.11 The Hokusai‑VTE trial12 (A Phase 3, Randomized, Parallel‑Group, Multi‑Center, Multi‑National Study for the Evaluation of Efficacy and Safety of [LMW] Heparin / Edoxaban Versus [LMW] Heparin / Warfarin in Subjects With Symptomatic Deep‑Vein Thrombosis [DVT] and or Pulmonary Embolism [PE]) confirmed edoxaban’s noninferiority, and the RE‑COVER trials13 (Efficacy and Safety of Dabigatran Compared to Warfarin for 6 Month Treatment of Acute Symptomatic Venous Thromboembolism) validated dabigatran for VTE treatment. These pivotal studies formed the evidence base for Food and Drug Administration (FDA) approval and clinical adoption of DOACs as first‑line VTE therapy.
Current mainline direct oral anticoagulants
Four DOACs are currently approved for VTE treatment in the United States.4,8 The group of FXa inhibitors include: rivaroxaban administered at 15 mg twice daily for 21 days, then 20 mg once daily (food requirement with 15–20 mg doses); apixaban administered at 10 mg twice daily for 7 days, then 5 mg twice daily (no food requirement); and edoxaban given at 60 mg once daily (requires 5–10 days initial heparin); dose adjustment to 30 mg if creatinine clearance (CrCl) is 15–50 ml/min. Direct thrombin inhibitor dabigatran is administered at 150 mg twice daily (requires 5–10 days initial heparin), and should be avoided if CrCl is below 30 ml/min.
Rivaroxaban and apixaban offer the advantage of single‑drug therapy without heparin bridging, potentially simplifying outpatient management.10,14 Dabigatran has the unique benefit of a specific reversal agent (idarucizumab), while FXa inhibitors can be reversed with andexanet alfa.15,16
Indications and contraindications
DOACs are indicated for treatment and extended secondary prevention of VTE, with evidence supporting their use across most patient populations. The American College of Chest Physicians (CHEST) and the 2024 European expert consensus strongly recommend DOACs as the first‑line therapy for VTE management.17-19 The 2023 American Society of Clinical Oncology (ASCO) guidelines added apixaban as a strong recommendation for cancer‑associated VTE, recognizing accumulating evidence in this previously challenging population.20
Key contraindications to DOACs include: 1) pregnancy and breastfeeding: as DOACs lack safety data and demonstrate potential teratogenic effects; low‑molecular‑weight heparin (LMWH) remains the standard19; 2) mechanical heart valves: due to increased thrombotic events observed with dabigatran in the RE‑ALIGN trial (Dabigatran Etexilate in Patients With Mechanical Heart Valves)4; 3) severe renal impairment: dabigatran should be avoided if CrCl is below 30 ml/min, edoxaban and apixaban doses should be reduced, and rivaroxaban is contraindicated for CrCl below 15 ml/min8,21; 4) strong modulators of cytochrome P450 3A4 and P‑glycoprotein: concurrent use with strong inducers (rifampin, phenytoin, carbamazepine) or strong inhibitors (ketoconazole, ritonavir) may require alternative anticoagulation4; 5) antiphospholipid syndrome: due to an increased risk of recurrent arterial thrombotic events with DOACs, as compared with VKAs.22,23
Venous thromboembolism
Pathophysiology
VTE pathogenesis follows the Virchow triad of venous stasis, endothelial injury, and hypercoagulability.2 Venous stasis, the most consequential factor, occurs when blood flow velocity decreases, particularly in valve pockets of deep leg veins. Prolonged immobility, surgery, or prolonged travel creates conditions favoring thrombus formation. Endothelial injury from trauma, surgery, central venous catheters, or inflammatory states exposes subendothelial collagen and tissue factor, initiating the coagulation cascade. Hypercoagulability may result from inherited thrombophilias (factor V Leiden, prothrombin G20210A mutation, protein C/S deficiency), acquired conditions (malignancy, pregnancy, hormone therapy), or inflammatory disorders.2,24 Without intervention, thrombi may propagate proximally, embolize to pulmonary circulation, or organize with potential for chronic complications, including post‑thrombotic syndrome.
Types of venous thromboembolism
DVT involves thrombus formation in deep veins, most commonly in lower extremities. Proximal DVT (popliteal, femoral, or iliac veins) carries a higher embolization risk than distal DVT (calf veins).
PE results from embolization of venous thrombi to pulmonary arteries, occurring in approximately 30%–40% of untreated proximal DVT cases. PE represents approximately 44% of VTE presentations, with another 14% presenting as combined DVT‑PE. Mortality within 1 month approximates 10% for PE, as compared with 6% for DVT alone.25
Unusual site thrombosis includes cerebral venous thrombosis, splanchnic vein thrombosis (portal, mesenteric, splenic), and renal vein thrombosis. Evidence for DOAC use in unusual site thrombosis remains limited, though emerging data suggest potential benefits.26
Diagnosis and treatment guidelines
The 2020 National Institute for Care and Health Excellence guidelines and 2023 American Society of Hematology recommendations advocate for DOAC initiation within 4 hours of VTE diagnosis when feasible.27 Initial treatment decisions should consider bleeding risk, renal function, drug interactions, body weight, and patient preferences.4,19
Standard VTE treatment duration for provoked VTE (reversible risk factor) is minimum 3 months17; for unprovoked VTE, 3–6 months initially, with consideration for extended therapy based on recurrence risk and bleeding risk.28 For cancer‑associated VTE, treatment should last for a minimum of 6 months, often indefinite when cancer is active.29 For second unprovoked VTE, indefinite anticoagulation should be considered.
Extended treatment with reduced‑dose DOACs (rivaroxaban 10 mg daily, apixaban 2.5 mg twice daily) demonstrates efficacy for VTE prevention while potentially reducing bleeding risk.30,31
Methods
This narrative review synthesized current evidence on DOAC use in VTE patients, with particular emphasis on challenges encountered in clinical practice. A comprehensive literature search was conducted in October 2025 across PubMed, MEDLINE, and Cochrane Library databases for peer‑reviewed articles published between 2019 and 2025.
Search strategy
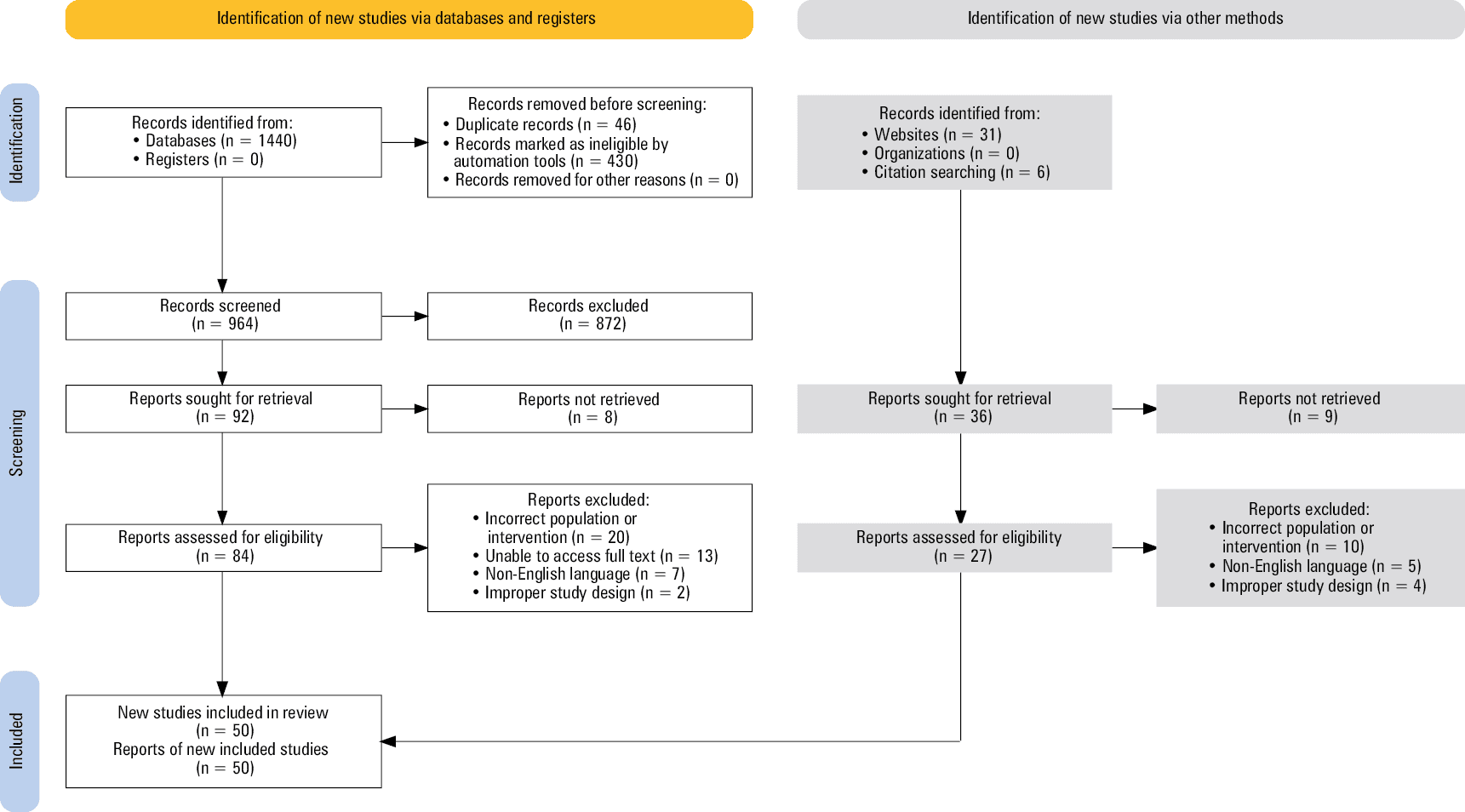
The following search terms were used in combination: “direct oral anticoagulants,” “DOACs,” “novel oral anticoagulants,” “NOACs,” “factor Xa inhibitors,” “direct thrombin inhibitors,” “rivaroxaban,” “apixaban,” “edoxaban,” “dabigatran,” “venous thromboembolism,” “VTE,” “deep vein thrombosis,” “DVT,” “pulmonary embolism,” and “PE.” The study selection process, including identification, screening, and eligibility assessment, is detailed in Figure 1. Following peer review, 14 additional references were incorporated to address reviewer feedback and include recently published evidence.
The inclusion criteria encompassed randomized controlled trials (RCTs), meta‑analyses, systematic reviews, observational studies, and clinical guidelines addressing DOAC use in VTE. Priority was given to recent publications (2019–2025). Articles were required to be in English and address clinically relevant outcomes, including efficacy, safety, adherence, or special populations.
The exclusion criteria were non‑English publications, articles published before 2019, case reports, conference abstracts without full‑text publication, and studies not directly addressing VTE management.
Data extraction
Relevant data were extracted regarding DOAC pharmacology, clinical trial outcomes, real‑world effectiveness, special population considerations, adherence patterns, bleeding management, and emerging therapeutic strategies. The review emphasizes practical clinical applications and current challenges in DOAC implementation.
Comparative effectiveness of direct oral anticoagulants
Meta‑analyses comparing the 4 DOACs for acute VTE treatment showed no significant differences in efficacy for preventing recurrent VTE.32 A 2020 analysis of 16 RCTs32 found that while rivaroxaban appeared to have the lowest risk of VTE recurrence and apixaban demonstrated the lowest major bleeding risk, the quality of evidence was rated as low for VTE outcomes and very low for bleeding in indirect comparisons. This reflects the absence of direct head‑to‑head trials between DOACs, relying instead on indirect comparisons through shared warfarin comparators.
Long et al14 confirmed that DOACs demonstrate similar or superior efficacy to conventional anticoagulation for DVT treatment, with potentially favorable bleeding profiles. Real‑world comparative effectiveness studies provide additional insights. Kang et al33 examined patients with second recurrent VTE, finding that DOAC use was associated with 62% relative risk reduction, as compared with warfarin (hazard ratio, 0.38; 95% CI, 0.18–0.77) with comparable major bleeding risk. This real‑world evidence complements RCT findings and extends applicability to higher‑risk populations often excluded from trials.
Special population challenges
Obesity and extreme body weight
Obesity presents a significant challenge for DOAC use given limited representation in pivotal trials and concerns about altered pharmacokinetics.21,34 Patients with body mass index (BMI) above 40 kg/m² or weight exceeding 120 kg comprised small percentages of trial populations, creating uncertainty about optimal dosing.
Martin et al35 reviewed anticoagulation approaches in morbid obesity (BMI ≥40 kg/m²). The current 2021 International Society on Thrombosis and Haemostasis guidance35 suggests standard doses of apixaban or rivaroxaban for VTE treatment in patients with BMI above 40 kg/m² or weight above 120 kg without routine drug level monitoring. However, evidence remains insufficient, particularly for patients with BMI over 50 kg/m² or weight over 150 kg. Dabigatran and edoxaban are generally not recommended in extreme obesity due to more pronounced renal clearance and limited obesity data.
Renal impairment
Renal function critically influences DOAC selection and dosing given varying degrees of renal elimination.8,21 Dabigatran’s 80% renal clearance makes it unsuitable for patients with severe renal impairment (CrCl <30 ml/min).17 Edoxaban requires dose reduction to 30 mg daily for CrCl 15–50 ml/min.36 Apixaban demonstrates the most favorable profile in renal impairment with only 27% renal elimination, though dose reduction is recommended for severe impairment.37
Dobesh et al21 addressed DOAC use in advanced renal impairment, noting that while moderate kidney disease (CrCl, 30–50 ml/min) allows for standard or reduced dosing depending on the agent, severe impairment requires careful consideration of pharmacokinetic alterations.
Cancer‑associated thromboembolism
Cancer patients face a 5‑fold elevated VTE risk from hypercoagulability, chemotherapy effects, indwelling catheters, and immobility.3,20,38,39 Historically, LMWH represented the standard therapy based on CLOT trial (Randomized Comparison of Low‑Molecular‑Weight Heparin versus Oral Anticoagulant Therapy for the Prevention of Recurrent Venous Thromboembolism in Patients with Cancer) data.40,41 However, DOACs have emerged as viable alternatives with practical advantages, including oral administration.
The 2023 ASCO guideline update added apixaban with high‑quality evidence and strong recommendation for cancer‑associated VTE treatment, joined by rivaroxaban as an option.20 This change reflected data from the CARAVAGGIO trial (Apixaban for the Treatment of Venous Thromboembolism in Patients with Cancer) demonstrating apixaban’s noninferiority to dalteparin with similar bleeding rates.42
However, challenges persist, as many aspects of VTE management yield discordant findings. Regarding cancer‑associated thrombosis, recent guidelines and meta‑analyses claim that patients with gastrointestinal cancers on DOACs have 2–4 times higher incidence of clinically relevant bleeding, as compared with LMWH.41,43 However, Upadhyaya et al29 studied gastrointestinal and genitourinary cancer patients, finding no difference in major bleeding or clinically relevant nonmajor bleeding between DOACs and LMWH, with comparable VTE recurrence. Shahbar et al39 identified predictors of bleeding in cancer patients on DOACs, including decreased CrCl and dexamethasone use. Effects of altered dosing in cancer‑associated VTE remains less clear. Some studies find no difference in outcomes between reduced and standard dosing; the EVE trial (Apixaban in Preventing Secondary Cancer Related Venous Thrombosis in Cancer Patients Who Have Completed Anticoagulation Therapy) found that apixaban dosed at 2.5 mg vs 5 mg did not decrease combined bleeding events in cancer patients with VTE.44 However, other significant studies’ results are at odds with these findings. The API‑CAT trial45 (Long‑term Treatment of Cancer Associated VTE: Reduced vs Full Dose of Apixaban: API‑CAT STUDY for Apixaban Cancer Associated Thrombosis) found that reduced‑dose DOACs lead to a lower incidence of clinically significant bleeding events, and a meta‑analysis by Bakht et al31 demonstrated that reduced‑dose DOACs showed safety profiles superior or comparable to full‑dose in cancer patients regarding VTE, bleeding, and mortality. These findings suggest growing acceptance of DOACs in cancer‑associated VTE, though careful patient selection and dosing decisions based on bleeding risk factors remain essential.46
Fragile and elderly patients
Elderly patients with frailty, polypharmacy, and multimorbidity present unique challenges. While being significantly underrepresented in clinical trials, these patients are at an increased risk of VTE and have increased sensitivity to anticoagulation.47 Park et al48 examined DOAC safety and effectiveness in fragile VTE patients using propensity score matching, finding that DOACs achieved effectiveness comparable to traditional anticoagulation with similar safety profiles. This real‑world evidence supports DOAC use in elderly populations, though careful attention to renal function, drug interactions, and fall risk remains necessary.
Adherence and persistence
Medication adherence critically influences DOAC effectiveness, particularly for extended treatment. Kang et al49 identified 4 distinct adherence trajectories during extended DOAC therapy: consistently high adherence, gradually declining, rapidly declining, and no extended treatment. Compared with the no extended treatment group, consistently high adherence demonstrated 91% reduction in recurrent VTE risk without increased major bleeding.
Paradoxically, rapidly declining adherence is associated with 2.65‑fold increased major bleeding risk.49 This finding suggests that intermittent DOAC exposure may create periods of heightened bleeding vulnerability without maintaining consistent anticoagulation benefits. These data underscore the importance of patient education, addressing barriers to adherence, and regular follow‑up during extended therapy.
Reversal agents and bleeding management
DOAC‑associated bleeding previously represented a significant concern given initial lack of specific reversal agents. Two agents have since gained approval, that is, idarucizumab for dabigatran and andexanet alfa for FXa inhibitors.15,16,50 Al Aseri et al16 provided an updated review of DOAC reversal agents. Idarucizumab, a humanized monoclonal antibody fragment, binds dabigatran, neutralizing its anticoagulant effect within minutes. The RE‑VERSE AD trial (Reversal of Dabigatran Anticoagulant Effect with Idarucizumab) demonstrated a rapid, complete reversal in 88%–98% of patients with life‑threatening bleeding or requiring urgent surgery.51
Andexanet alfa, a modified recombinant FXa molecule lacking enzymatic activity, acts as a decoy binding FXa inhibitors.15 Phase III trials (ANNEXA‑A [Trial of Andexanet Alfa in ICrH Patients Receiving an Oral FXa Inhibitor] and ANNEXA‑R [A Phase 3 Randomized, Double‑Blind, Placebo Controlled Trial Demonstrating Sustained Reversal of Rivaroxaban Induced Anticoagulation in Older Subjects by Andexanet alfa {PRT064445}, a Universal Antidote for Factor Xa {fXa} Inhibitors]) showed 92%–94% reduction in anti‑FXa activity within minutes of administration.52 The ANNEXA‑4 study (Prospective, Open‑Label Study of Andexanet Alfa in Patients Receiving a Factor Xa Inhibitor Who Have Acute Major Bleeding) demonstrated effective hemostasis in approximately 82% of patients with major bleeding.53
Goldin et al15 reviewed DOAC reversal for critical bleeding, noting that patients receiving specific reversal agents demonstrated significantly shorter hospital and intensive care unit stay plus fewer ventilator days, as compared with nonspecific reversal approaches. While thrombotic complications remain a concern following reversal agent administration (approximately 10% in ANNEXA‑4 trial), these agents provide critical management options for life‑threatening bleeding. Recent evidence has emerged regarding the use of prothrombin complex concentrate (PCC) as an agent for DOAC reversal. A meta‑analysis by Chaudhary et al54 compared PCC to andexanet alfa and idarucizumab in reversing anticoagulation in intracranial hemorrhage, finding that there was no difference in successful anticoagulation reversal, all‑cause mortality, or thromboembolic events between the agents.
For non–life‑threatening bleeding, supportive measures, including DOAC discontinuation, mechanical compression, local hemostatic measures, and fluid resuscitation often suffice given DOACs’ relatively short half‑lives.4,16
Emerging strategies: reduced‑dose extended therapy
Extended anticoagulation beyond initial VTE treatment reduces recurrence risk but increases bleeding risk. Recent evidence supports reduced‑dose DOAC regimens for extended prophylaxis. In their Cochrane review, Imberti et al30 found that all studied DOACs proved effective for extended VTE prevention, though bleeding events increased in comparison with placebo.
A meta‑analysis by Bakht et al31 specifically examined reduced‑dose vs full‑dose DOACs in cancer patients, finding that reduced‑dose regimens demonstrated safety profiles either superior or comparable to full‑dose regarding VTE recurrence, bleeding events, and all‑cause mortality. This suggests that for selected patients requiring extended anticoagulation, particularly those at a higher bleeding risk, reduced‑dose regimens may optimize the benefit‑risk ratio.
The EINSTEIN‑CHOICE trial55 (Reduced‑dosed Rivaroxaban in the Long‑term Prevention of Recurrent Symptomatic VTE) demonstrated that rivaroxaban at both 10 mg and 20 mg daily proved superior to aspirin for extended VTE prevention, with the lower dose showing numerical trends toward less bleeding. Similarly, the AMPLIFY‑EXT trial56 (Extended‑Duration Low‑Intensity Apixaban to Prevent Recurrence in High‑Risk Patients With Provoked Venous Thromboembolism) found apixaban 2.5 mg twice daily effective for extended treatment with acceptable bleeding rates. These data informed FDA approval of reduced‑dose options for extended VTE prophylaxis.
Inpatient vs outpatient management
The shift toward outpatient VTE management has accelerated with DOAC availability. DOACs’ rapid onset, predictable pharmacokinetics, and lack of monitoring requirements make them ideally suited for outpatient management in appropriate cases.57
Criteria for outpatient management generally include hemodynamic stability, adequate cardiopulmonary reserve, low bleeding risk, ability to adhere to therapy, and adequate outpatient follow‑up. High‑risk PE, significant comorbidities, or social barriers may necessitate hospitalization despite DOAC availability.
Perioperative management
Perioperative DOAC management requires balancing thrombotic and bleeding risks. The PAUSE study (Perioperative Anticoagulant Use for Surgery Evaluation) established practical guidance: for low‑bleeding‑risk procedures, hold DOACs for 1 day (apixaban / rivaroxaban) or 2 days (dabigatran / edoxaban) preoperatively; for high‑bleeding‑risk procedures, extend holding to 2 days (apixaban / rivaroxaban) or 4 days (dabigatran / edoxaban), adjusted for renal function.58
Resumption typically occurs 24–72 hours postoperatively depending on bleeding risk and achievement of hemostasis. Bridging with therapeutic‑dose parenteral anticoagulation during DOAC interruption is not recommended based on the PAUSE study findings showing acceptably low thrombotic event rates without bridging.58
Postoperative prophylaxis of venous thromboembolism
Tun et al59 reviewed DOACs for postoperative VTE prophylaxis, highlighting that phase III trials demonstrated promising results, particularly for orthopedic surgery. Rivaroxaban and apixaban have gained approval for thromboprophylaxis following hip and knee arthroplasty based on RECORD (eg, Rivaroxaban [10mg] Given Once Daily in Patients Undergoing Total Hip Replacement Compared to Enoxaparin) and ADVANCE (eg, Study of Apixaban for the Prevention of Thrombosis‑related Events Following Knee Replacement Surgery) trial programs60,61 showing noninferior or superior efficacy in comparison with enoxaparin.
Unusual site thrombosis
Evidence for DOAC use in unusual site thrombosis remains limited. Ferro et al26 compared dabigatran to warfarin for cerebral venous thrombosis in the RE‑SPECT CVT trial (A Clinical Trial Comparing Efficacy and Safety of Dabigatran Etexilate With Warfarin in Patients with Cerebral Venous and Dural Sinus Thrombosis), finding similar efficacy and safety. While promising, evidence remains insufficient to strongly recommend DOACs over warfarin for unusual site thrombosis, though they represent reasonable alternatives in selected patients.
Clinical recommendations
Based on the current guidelines and recent data, the recommendations reported in Table 1 guide DOAC use in VTE patients.
Patient population | Preferred DOAC(s) | Recommendations | Considerations |
Abbreviations: BID, twice daily; BMI, body mass index; CHEST, American College of Chest Physicians; DOAC, direct oral anticoagulant; DVT, deep vein thrombosis; GI, gastrointestinal; LMWH, low‑molecular‑weight heparin; PAUSE, Perioperative Anticoagulant Use for Surgery Evaluation; PE, pulmonary embolism; VTE, venous thromboembolism | |||
Standard VTE (DVT/PE) | All DOACs | First‑line therapy for acute VTE4,5 | Superior or comparable efficacy to warfarin. Favorable bleeding profile. |
Cancer‑associated VTE | First line: apixaban Second line: rivaroxaban | Well‑researched and established alternatives to LMWH20 | Assess bleeding risk carefully in GI malignancies, thrombocytopenia, and patients with concomitant steroid use. |
Obesity (BMI >40 kg/m2; weight >120 kg) | Standard‑dose apixaban or rivaroxaban | Standard dosing, no need for routine monitoring34 | Limited evidence in patients with BMI >50 kg/m2 or weight >150 kg. Avoid dabigatran and edoxaban. |
Renal impairment | Apixaban, edoxaban (with dose reduction in moderate‑severe renal impairment) | Adjust dose as needed. Dabigatran not recommended for severe impairment8,21 | Regular renal function monitoring during treatment. |
Extended VTE prophylaxis | Reduced‑dose apixaban or rivaroxaban | Consider for patients at elevated bleeding risk. Apixaban 2.5 mg BID or rivaroxaban 10 mg daily10,55,56 | Protocol for indefinite therapy for unprovoked VTE. |
Poor adherence / noncompliance | Patient preference of DOAC | Educate patients on importance of adherence, address barriers to compliance.49 | Consistently high adherence reduces VTE recurrence by 91% with regular follow‑up. |
Major bleeding events on DOACs | Reversal agents: andexanet alfa or idarucizumab (dabigatran) | Implement institutional protocols for rapid assessment and treatment in life‑threatening bleeding.16 | Availability of specific reversal agents is essential for acute DOAC bleeding management. |
Perioperative management | Any DOAC | Follow CHEST guidelines and PAUSE protocols. No bridging required.18,58,59 | Hold 1–4 d preprocedure based on DOAC, bleeding risk, and renal function. Resume 24–72 h postoperatively. |
Gaps and ongoing research
Gaps in the literature regarding the use of DOACs in VTE patients still remain, with ongoing clinical trials and studies aiming to close these blind spots. While apixaban has become the standard for patients with atrial fibrillation (AF), there is ongoing research to determine the efficacy of alternative DOACs in this population; the LIBREXIA‑AF study (A Study of Milvexian Versus Apixaban in Participants with Atrial Fibrillation) is an ongoing phase III clinical trial evaluating melvexian, an oral FXI inhibitor as an alternative to apixaban.62 Within this population, there is also limited evidence regarding anticoagulation in patients with valvular stenosis, with guidelines recommending VKAs in individuals with valvular heart disease and AF. Currently, the DAVID‑MS trial (Dabigatran for Mitral Stenosis Atrial Fibrillation) is evaluating the viability of DOACs in this population in comparison with the current standard of VKAs.63 Advances in technological monitoring and intervention, while having limited evidence so far, have the potential to improve outcomes in DOAC use in AF patients. The REACT‑AF clinical trial (The Rhythm Evaluation for Anticoagulation with Continuous Monitoring of Atrial Fibrillation) aims to use technological advancement to achieve this goal. This RCT compares the standard of care of continuous anticoagulation with time‑limited (1 month) DOAC use guided by AF‑sensing smart watches in patients with paroxysmal and persistent AF.64
Limitations
This narrative review has several limitations. First, the synthesis relies predominantly on indirect comparisons between DOACs, given the lack of direct head‑to‑head trials. Second, special population data derive largely from post hoc analyses and observational studies rather than prospective randomized trials, limiting causal inference. Third, long‑term outcomes beyond 1–2 years remain incompletely characterized, particularly for reduced‑dose extended therapy regimens. Fourth, cost‑effectiveness analyses were not systematically addressed, though DOAC costs and insurance coverage significantly influence real‑world accessibility. Finally, as in a narrative rather than systematic review, potential for selection bias exists despite comprehensive search strategies.
Conclusions
DOACs have fundamentally transformed VTE management, offering efficacy comparable or superior to VKAs with practical advantages including predictable pharmacokinetics, fixed dosing, rapid onset, and elimination of routine monitoring. Current evidence robustly supports DOACs as first‑line therapy for most VTE patients. However, everyday clinical practice continues to present challenges requiring individualized decision‑making.
Special populations demand careful benefit‑risk assessment and familiarity with emerging evidence on dose modifications. Medication adherence critically influences outcomes, with consistently high adherence achieving maximal VTE prevention benefits. The availability of specific reversal agents addresses previous concerns about managing DOAC‑associated major bleeding, though thrombotic complications following reversal warrant vigilance.
Emerging evidence supports reduced‑dose DOAC regimens for extended VTE prophylaxis, potentially optimizing the benefit‑risk ratio in patients requiring prolonged anticoagulation. As real‑world data accumulate and randomized trials address remaining evidence gaps, clinicians gain increasing confidence managing DOACs across diverse patient populations. Continued emphasis on patient education, adherence optimization, and familiarity with reversal strategies will maximize the benefits of these transformative anticoagulants while minimizing the risks.
- Marschang P, Gerotziafas G, Kozak M, et al. Epidemiology of venous thromboembolism: implications for clinical practice. Pol Arch Intern Med. 2025; 135: 17105. | Crossref
- Kushner A, West WP, Khan Suheb MZ, Pillarisetty LS. Virchow Triad. In: StatPearls. Treasure Island (FL): StatPearls Publishing, 2025. | Crossref
- Krasiński Z, Undas A, Podolak‑Dawidziak M, et al. Thromboprophylaxis in medical patients: a 2025 update of Polish recommendations. Pol Arch Intern Med. 2025; 135: 17047. | Crossref
- Burnett AE, Mahan CE, Vazquez SR, et al. Guidance for the practical management of the direct oral anticoagulants (DOACs) in VTE treatment. J Thromb Thrombolysis. 2016; 41: 206‑232. | Crossref
- Cabral KP, Ansell J. The role of factor Xa inhibitors in venous thromboembolism treatment. Vasc Health Risk Manag. 2015; 11: 117‑123. | Crossref
ARTICLE INFORMATION