We report a case of a 63‑year‑old man who underwent lung transplantation 2.5 years earlier due to fibrosing hypersensitivity pneumonitis. The surgery was performed at another center, where he subsequently received follow‑up care. Standard immunosuppressive therapy was administered: tacrolimus, mycophenolate mofetil, and prednisone. The early post‑transplant period was uneventful. In the second year after transplant, the patient developed skin nocardiosis, which was successfully treated. Twenty‑eight months after surgery, the patient began to experience pain in the right subcostal area, radiating to the right upper abdomen and right shoulder. He was initially assessed in an outpatient setting, with back pain misattributed to radicular pain or gallstone‑related cholecystitis, leading to ineffective antibiotic treatment.
The patient presented to our clinic on his own initiative 3 weeks later. Physical examination showed swelling of the subcutaneous tissue on the right side of the chest and tenderness on palpation of the upper right quadrant of the abdomen. Auscultation demonstrated dullness over the lower and middle fields of the right lung. Baseline laboratory tests showed moderate anemia (hemoglobin, 9.2 g/dl; reference range [RR]; 14–17 g/dl and elevated C‑reactive protein levels (60 mg/l; RR <5 mg/l), while polymerase chain reaction serum tests for Epstein–Barr virus (EBV) and cytomegalovirus were negative. Ultrasound examination identified extensive consolidation in the lower part of the right lung, lacking a bronchial pattern and exhibiting abnormal vascularity (Figure 1A). Computed tomography showed an atelectatic lower lobe of the right lung with heterogeneous infiltration of the pleura and increased vascularity extending into the paravertebral muscles and subcutaneous tissue (Figure 1B–1D). No significant endobronchial or microbiological abnormalities were found on bronchoscopy. Transthoracic ultrasound‑guided core needle biopsy of the lung was performed. Histopathological examination demonstrated malignant tumor infiltration with cell morphology requiring differentiation between the plasmablastic form of plasmocytoma and aggressive terminal B‑cell lymphoma with massive plasmablastic differentiation (Figure 1E–1H).
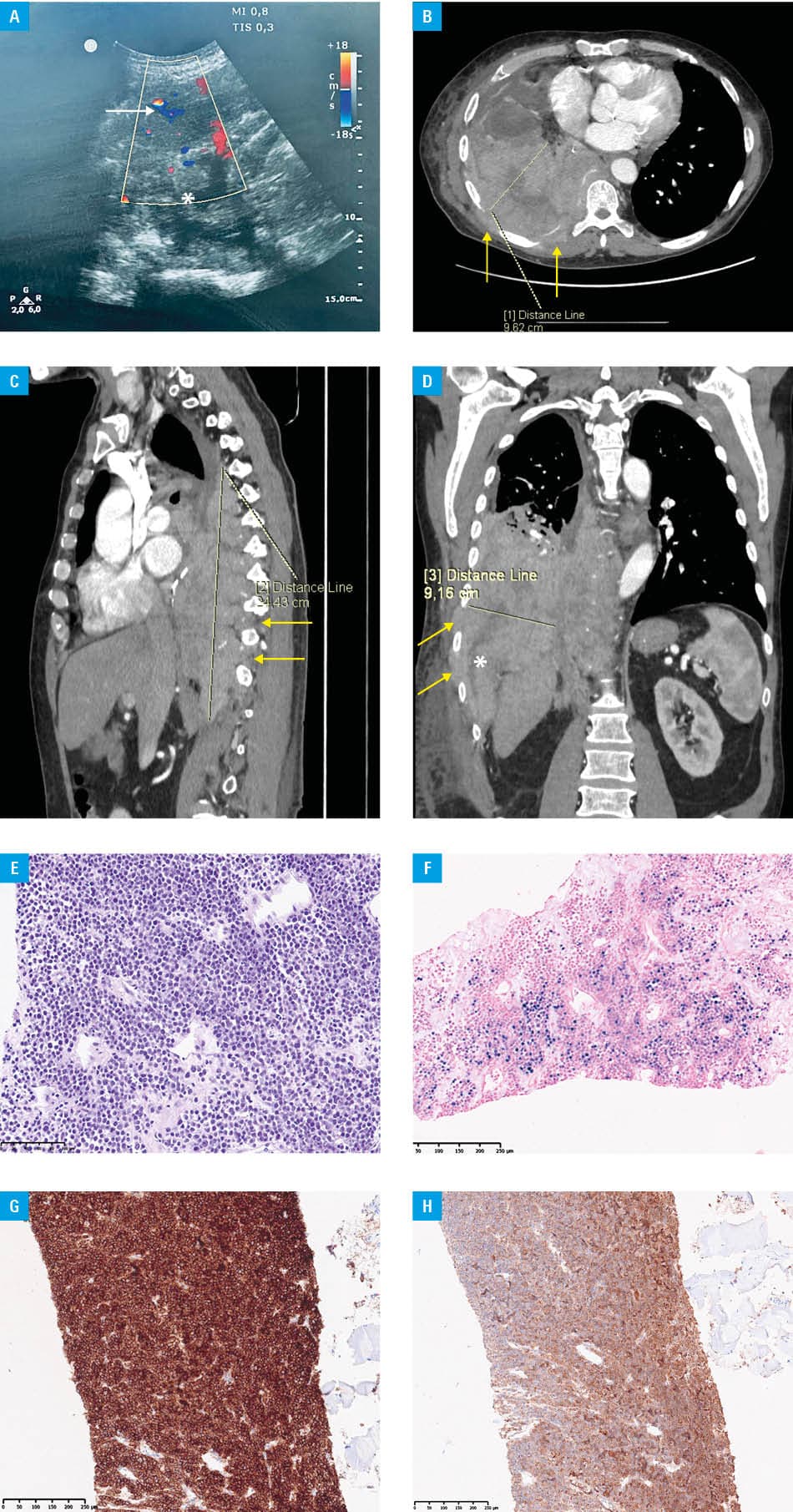
Correlation of clinical, histopathological, and immunohistochemical findings allowed for the final diagnosis of aggressive EBV‑positive extraosseous plasmablastic plasmacytoma in the post‑transplant lung setting. According to the latest 2022 World Health Organization classification of lymphomas, this entity is categorized within a newly defined subgroup of lymphomas arising in the setting of immune deficiency / dysregulation after lung transplant.1 The previous nomenclature of such tumors as monomorphic post‑transplant lymphoproliferative disorders is no longer recommended.
Due to severe pain, the patient required high doses of opioids and coanalgesics. His condition rapidly deteriorated, and he developed respiratory failure (initially treated with high‑flow oxygen therapy, followed by invasive ventilation, and ultimately extracorporeal membrane oxygenation), followed by multiorgan failure. Given his general condition at the time of diagnosis, causal treatment could not be initiated, and the patient died 19 days after the biopsy.
Organ recipients have approximately a 1.8‑fold increased risk of developing plasma cell neoplasms.2 Extramedullary plasmocytoma or multiple myeloma in the lung is an unusual condition.3,4 The presented case of aggressive, extramedullary EBV‑positive plasmablastic plasmocytoma in a transplanted lung is exceptionally rare and underscores the potential for lymphoma / plasmocytoma transformation in the setting of post‑transplant immunosuppression. To our knowledge, this is the first description of such neoplasm in a transplanted lung, and the only previously documented case involved a transplanted kidney.5
This case highlights the resistance and high mortality associated with this specific form of extramedullary plasma cell neoplasm in an immunocompromised patient population.
- Naresh KN, Bhagat G, Bowe M, et al. Lymphomas arising in immune deficiency / dysregulation. In: WHO Classification of Tumours Editorial Board. Haematolymphoid tumours. 5th ed. IARC: Lyon, France. 2024: 568‑572. | Crossref
- Engels EA, Clarke CA, Pfeiffer RM, et al. Plasma cell neoplasms in U.S. solid organ transplant recipients. Am J Transplant. 2013; 13: 1523‑1532. | Crossref
- Friedberg JW, Aster JC. Epidemiology, clinical manifestations, and diagnosis of post‑transplant lymphoproliferative disorders. UpToDate. Literature review current through: Sep. 2025. https://www.uptodate.com/contents/epidemiology‑clinical‑manifestations‑and‑diagnosis‑of‑post‑transplant‑lymphoproliferative‑disorders/print. Accessed October 28, 2025.
- Ayeboa‑Sallah B, Qutab S, Grace R, Sharma N. Rare case of plasmablastic myeloma diagnosed on lung biopsy. BMJ Case Reports. 2021; 14: e240998. | Crossref
- Bi L, Bai Y, Li J, Chen W. Multiple myeloma with extramedullary plasmacytoma in a renal transplant recipient: a case report and review of literature. Int J Clin Exp Med. 2018; 11: 12693‑12697. | Crossref
ARTICLE INFORMATION