Increased cardiovascular mortality with single antiplatelet therapy in anticoagulation-treated chronic coronary syndrome patients: meta-analysis of randomized trials
Key words: antiplatelet therapy, cardiovascular mortality, chronic coronary syndrome, meta-analysis, oral anticoagulation

 CC BY 4.0
CC BY 4.0
Increased cardiovascular mortality with single antiplatelet therapy in anticoagulation-treated chronic coronary syndrome patients: meta-analysis of randomized trials
Introduction: The optimal antithrombotic regimen for chronic coronary artery disease (CAD) requiring long‑term anticoagulation remains uncertain.
Objectives: We aimed to determine the effects of oral anticoagulation (OAC) monotherapy in comparison with OAC plus single antiplatelet therapy (OAC+SAPT) on cardiovascular mortality in chronic CAD. The secondary objective was to assess the effects of both antithrombotic approaches on major bleeding, nonfatal ischemic events, and all‑cause death.
Patients and methods: We searched PubMed, Embase, and Cochrane CENTRAL (up to August 2025) for randomized trials comparing OAC alone vs OAC+SAPT in chronic CAD. Fixed‑effects models were used when heterogeneity was low (I² <50%); otherwise, random‑effects models were applied. Prespecified sensitivity analyses included a Bayesian meta‑analysis and trial sequential analysis (TSA). The primary outcome was cardiovascular death; secondary outcomes were all‑cause death, major bleeding, nonfatal myocardial infarction, and ischemic stroke.
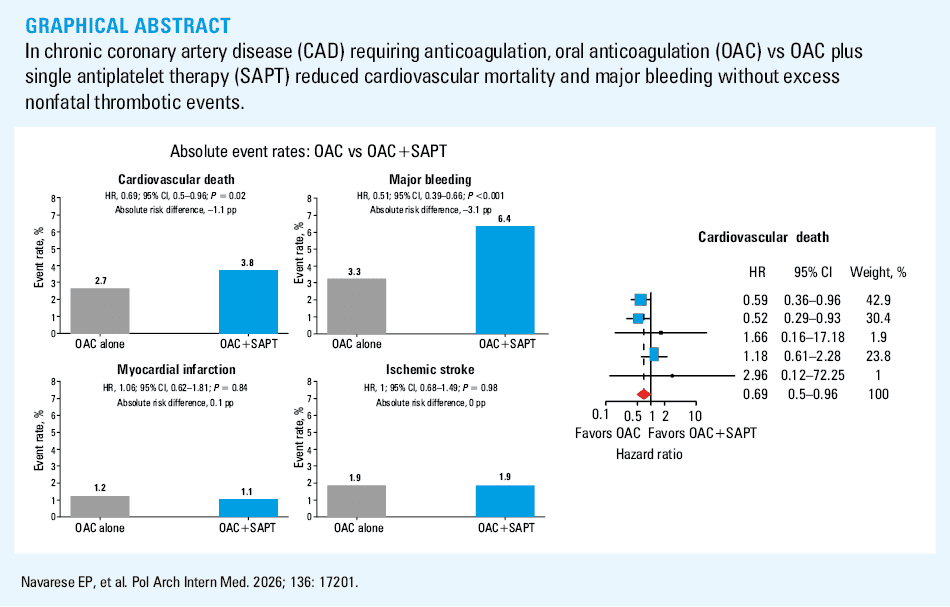
Results: Five trials (AFIRE, AQUATIC, EPIC‑CAD, OAC‑ALONE, and PRAEDO AF; n = 4964; follow‑up range, 12–30 mo) met the eligibility criteria. Cardiovascular death occurred in 2.7% of the patients on OAC alone vs 3.8% on OAC+SAPT (hazard ratio [HR], 0.69; 95% CI, 0.5–0.96; P = 0.02). The Bayesian analysis confirmed the result (HR, 0.75; 95% credible interval, 0.61–0.93). TSA crossed the efficacy boundary, supporting firm evidence for cardiovascular mortality reduction with OAC alone. All‑cause mortality was numerically, but not significantly, lower on OAC alone (4.9% vs 6.7%; HR, 0.79; 95% CI, 0.5–1.24; P = 0.3). Major bleeding was reduced on OAC alone (3.3% vs 6.4%; HR, 0.51; 95% CI, 0.39–0.66; P <0.001). Myocardial infarction and ischemic stroke incidence did not differ significantly in the treatment arms.
Conclusions: In chronic CAD requiring anticoagulation, OAC monotherapy vs OAC+SAPT reduced cardiovascular mortality and major bleeding without an excess in nonfatal thrombotic events, generally supporting OAC alone as the preferred long‑term strategy in this patient population.
What's new?
In patients with chronic coronary artery disease (CAD) requiring long‑term oral anticoagulation (OAC), the optimal long‑term antithrombotic regimen remains debated. This meta‑analysis of 5 randomized trials, including the recent European AQUATIC trial, shows that OAC monotherapy reduces cardiovascular mortality and major bleeding, as compared with OAC combined with a single antiplatelet agent, without increasing the incidence of nonfatal myocardial infarction or ischemic stroke over median follow‑up of 23 months. Bayesian and trial‑sequential analyses confirm that the evidence for cardiovascular mortality reduction is statistically robust. The reduction in cardiovascular mortality and major bleeding, without excess nonfatal thrombotic events, generally supports OAC alone as the preferred long‑term antithrombotic strategy for this patient population.
Introduction
Long‑term prescription of full‑dose oral anticoagulation (OAC) with an antiplatelet agent is not uncommon in clinical practice. Such dual antithrombotic therapy typically involves patients with atrial fibrillation (AF) and chronic coronary artery disease (CAD). Despite growing evidence suggesting that less is more,1,2 the recent AQUATIC trial (Aspirin in Patients with Chronic Coronary Syndrome Receiving Oral Anticoagulation) reported that 68% of patients receiving long‑term OAC, with a coronary stent implantation more than 6 months before, were receiving additional single antiplatelet therapy (SAPT) at trial enrollment.3
Combining OAC (to prevent systemic thromboembolism) and an antiplatelet agent (to mitigate atherothrombosis) has a rational basis. However, this strategy predictably increases bleeding without necessarily yielding ischemic protection after the acute or early‑intervention period.3-7 In the above settings, the effect of OAC alone vs OAC+SAPT on cardiovascular mortality remains uncertain. Individual trials3-7 and meta‑analyses8 have so far been underpowered for cardiovascular death, given low event rates, wide CIs, and noninclusion of the most recent evidence.
We performed a meta‑analysis of all available randomized controlled trials (RCTs) comparing OAC monotherapy against OAC+SAPT (as of August 2025), prespecifying cardiovascular mortality as the primary end point. Secondary end points included nonfatal ischemic or bleeding events and all‑cause death. To assess robustness and address residual uncertainty, we applied both frequentist and Bayesian random‑effects models.
Methods
Established methods recommended by the PRISMA statement were used.9,10 A systematic literature search of PubMed, Embase, and the Cochrane Central Register of Controlled Trials was conducted from inception through August 2025. The full electronic search string for PubMed, and the corresponding search combinations for Embase and Cochrane base, included the key words and MeSH/Emtree terms of “oral anticoagulants,” “coronary artery disease,” “atrial fibrillation,” “antiplatelet therapy,” and “randomized trial.” References of the included studies and reviews were searched for additional eligible trials. Two independent reviewers (EPN and FA) screened the titles, abstracts, and full‑text articles for eligibility. The studies were included when CAD patients with established indications for anticoagulation were randomly allocated to either OAC alone or OAC+SAPT. Observational studies or those comparing triple vs dual antithrombotic therapy were not included. No language restrictions were applied. The meta‑analysis is registered in the PROSPERO database (CRD420251167661).
Data extraction
Data extraction was performed using standardized forms that included study characteristics, patient demographics, intervention details, and clinical outcomes. The primary outcome was cardiovascular mortality. Main secondary outcomes included all‑cause mortality, major bleeding (as defined by each study), nonfatal myocardial infarction (MI), and nonfatal ischemic stroke (IS). Risk of bias was assessed using the Cochrane Risk of Bias tool 2.011 that considers randomization process, deviations from intended interventions, missing outcome data, outcome measurements, and selection of reported results. Overall risk of bias was defined as low, with some concerns, or high.
Statistical analysis
Trial‑level data were analyzed according to the intention‑to‑treat principle. Hazard ratios (HRs) with 95% CIs were abstracted from individual studies. A fixed‑effects model was used when between‑study heterogeneity was low to moderate (I2 <50%); otherwise, random‑effects models were applied.12,13 Publication bias was evaluated using funnel plots. Certainty in the body of evidence for each outcome was evaluated according to the Grading of Recommendations Assessment, Development and Evaluation approach, considering study limitations, inconsistency (I2), indirectness, imprecision, and publication bias. Certainty was rated as high, moderate, low, or very low (Supplementary material, Table S1). Exploratory absolute risk differences (ARDs) were calculated for each outcome. A random‑effects Bayesian meta‑analysis was performed for cardiovascular death to obtain posterior probability distributions of treatment effects.14 The overall effect was assigned a weakly informative normal prior on the logarithmic HR scale, reflecting a conservative relative difference. Between‑study heterogeneity τ followed a half‑normal prior, with scale 0.1, consistent with empirical heterogeneity for mortality outcomes. We report posterior HR medians with 95% credible intervals (CrIs) and the posterior probability of a cardiovascular‑mortality effect. Trial sequential analysis (TSA) was performed for the primary outcome to assess whether the cumulative sample size was sufficient to detect the observed treatment effect. TSA monitoring boundaries used a 2‑sided O’Brien–Fleming α-spending function (type I error 5%; type II error 20% [80% power]). The required information size was estimated from the control event rate and the anticipated relative risk reduction. Meta‑analyses were conducted in R (version 4.3.2; R Foundation for Statistical Computing, Vienna, Austria) with the meta and bayesmeta packages, and in Python (version 3.12; Python Software Foundation, Wilmington, Delaware, United States). We also prespecified a sensitivity analysis restricted to East‑Asian trials (AFIRE [Atrial Fibrillation and Ischemic Events with Rivaroxaban in Patients with Stable Coronary Artery Disease],4 EPIC‑CAD [Edoxaban vs Edoxaban with Antiplatelet Agent in Patients with Atrial Fibrillation and Chronic Stable Coronary Artery Disease],5 OAC‑ALONE [Optimizing Antithrombotic Care in Patients with Atrial Fibrillation and Coronary Stent],6 and PRAEDO‑AF [Prospective Randomized Study of Safety Outcomes Treated with Edoxaban in Patients with Stable Coronary Artery Disease and Atrial Fibrillation],7 excluding the European AQUATIC study,3 to explore whether regional setting, lower direct oral anticoagulant (DOAC) dosing, and nonexclusive use of aspirin could modify the treatment effect of OAC monotherapy vs OAC+SAPT. A 2‑sided P value below 0.05 was considered significant.
Results
Study selection and characteristics
The systematic search identified 2847 potentially relevant articles. After removing duplicates and screening titles and abstracts, 34 full‑text articles were assessed for eligibility. Five RCTs met the inclusion criteria,3-7 encompassing 4964 patients (Supplementary material, Figure S1).
The included trials were published between 2019 and 2025, with median follow‑up of 23 months (range, 12 to 30 mo). Most patients had AF and CAD requiring percutaneous coronary intervention (PCI), which was performed more than 6 months before enrollment. Three trials were discontinued prematurely: 2 for excess harm in 1 treatment arm (AFIRE4 and AQUATIC3), and 1 due to COVID‑19 pandemic (PRAEDO‑AF7). Baseline demographics, comorbidities, and risk scores were similar between treatment arms in each trial (Table 1). Anticoagulation was predominantly provided with DOACs, except in the OAC‑ALONE6 trial, where 75.2% of patients received warfarin. In the combination‑therapy arm, aspirin was administered overall in 68.3% and clopidogrel in 29.2% of cases.
Study / country / median follow‑up / design | Arm | Age, y, mean (SD) | Men, % | Diabetes, % | Prior MI, % | Prior PCI, % / time from PCI, mo | CHA2DS2-VASc, points | HAS‑BLED, points | OAC type / reason for OAC | SAPT in dual arm |
Mean values are provided with SD and median values with interquartile range in parentheses.
Abbreviations: AF, atrial fibrillation; approx., approximately; DOAC, direct oral anticoagulant; MI, myocardial infarction; NR, not reported; OAC, oral anticoagulant; PCI, percutaneous coronary intervention; PROBE, prospective randomized open‑label design with blinded end point adjudication; SAPT, single antiplatelet therapy; VKA, vitamin K antagonist | ||||||||||
AFIRE4 / Japan / 23 mo / PROBE | Rivaroxaban + SAPT (n = 1108) | 74.4 (8.2) | 79.1 | 42.1 | 35.5 | 70.7 / >12 | NR per arm | NR per arm | Rivaroxaban
(15 mg daily; 10 mg if dose‑reduced) / AF | Aspirin, approx. 70.2%; P2Y12, approx. 26.8% (mostly clopidogrel and rarely prasugrel) |
Rivaroxaban monotherapy (n = 1107) | 74.3 (8.5) | 79 | 41.6 | 34.7 | 70.6 / >12 | NR per arm | NR per arm | Rivaroxaban
as above / AF | – | |
AQUATIC3 / France / 26 mo / double‑blind | OAC + aspirin (n = 433) | 72.3 (9.3) | 85.5 | 38 | 71.5 | 100 / >6 | Median, 4 (3–5) | NR at baseline | DOAC, 89.7% (apixaban, 62.2%; rivaroxaban, 24.7%; dabigatran, 2.9%); VKA, 10.3% (overall) / AF in 89% | Aspirin 100 mg daily |
OAC + placebo (n = 439) | 71.1 (9.6) | 85.2 | 36.9 | 72.7 | 100 / >6 | Median, 4 (3–5) | NR at baseline | As above / AF in 89% | – | |
EPIC‑CAD5 / South Korea / 12 mo / PROBE | Edoxaban + SAPT (n = 516) | 72.5 (8.4) | 78.7 | 38.2 | 17.8 | NR (revascularization, 65.7% overall) / >6 | Mean, 4.4 (1.5); median, 4 (3–5) | Mean, 2.2 (0.8); Median, 2 (2–3) | Edoxaban dose adjusted for renal function and body weight / AF | Aspirin, 61.8%; clopidogrel, 37.8%; other, 0.4% |
Edoxaban monotherapy (n = 524) | 71.7 (8) | 75.6 | 42.7 | 15.1 | NR (revascularization, 65.7% overall) / >6 | Mean, 4.3 (1.6); median, 4 (3–5) | Mean, 2.1 (0.8); Median, 2 (2–3) | Edoxaban as above / AF | – | |
OAC‑ALONE6 / Japan / 30 mo / PROBE | OAC + SAPT (n = 346) | 75.2 (0.4) | 85 | 39.9 | 39.6 | NR / >12 | Mean, 4.6 (1.4); ≥3 in 94.8% | Categories: 1 approx. 3%, 2 approx. 52%, ≥3 approx. 44.8% | Warfarin, 76.3%; DOAC, 23.7% (dabigatran, 24.4%; rivaroxaban, 20.7%; apixaban, 45.1%; edoxaban, 9.8% among DOAC users) / AF | Aspirin, 86.4%; Clopidogrel, 13.9% |
OAC alone (n = 344) | 74.9 (0.4) | 85.5 | 44.2 | 37.5 | NR / >12 | Mean, 4.6 (1.4); ≥3 in 93.9% | Categories: 1 approx. 5%, 2 approx. 51%, ≥3 approx. 43.6% | As above / AF | – | |
PRAEDO AF7 / Japan / 21 mo / open label and adjudication | Edoxaban + clopidogrel (n = 73) | 74 (9) | 86 | 47 | NR | NR / >6 | Overall median, approx. 4 (per‑arm NR) | Overall median, approx. 3 (per‑arm NR) | Edoxaban dose adjusted for renal function and body weight / AF | Clopidogrel |
Edoxaban monotherapy (n = 74) | 74 (7) | 87 | 39 | NR | NR / >6 | Overall median, approx. 4 (per‑arm NR) | Overall median, approx. 3 (per‑arm NR) | Edoxaban / AF | – | |
Risk of bias assessment
Overall risk of bias was low in all 5 studies, with no bias component classified as high risk. All studies had adequate randomization procedures and low risk of attrition bias (Supplementary material, Table S2).
Primary outcome of cardiovascular death
Cardiovascular mortality data were available in all trials. This outcome occurred in 68 of 2488 patients in the OAC alone group vs 94 of 2476 patients in the OAC+SAPT group (2.7% vs 3.8%; I2 = 22.8%; HR, 0.69; 95% CI, 0.5–0.96; P = 0.03; Figure 1A). The Bayesian meta‑analysis confirmed a significant cardiovascular mortality reduction with OAC vs OAC+SAPT (HR, 0.75; 95% CrI, 0.61–0.93; Figure 1B). The TSA showed that the sample size of 4964 patients exceeded the required information size (approximately 4384 patients), indicating sufficient accrued evidence to demonstrate a cardiovascular mortality reduction with OAC alone (Figure 1C). The Bayesian probability density plot for the absolute difference indicated a 98.2% posterior probability of OAC alone reducing cardiovascular mortality, as compared with OAC+SAPT (Supplementary material, Figure S2).
Secondary outcomes
All‑cause mortality data were available in all trials. This outcome occurred in 123 of 2488 patients in the OAC arm and in 166 of 2476 patients in the OAC+SAPT arm, a large numerical difference that, however, did not achieve significance (4.9% vs 6.7%; I2 = 59.7%; HR, 0.79; 95% CI, 0.5–1.24; P = 0.3; Figure 1D).
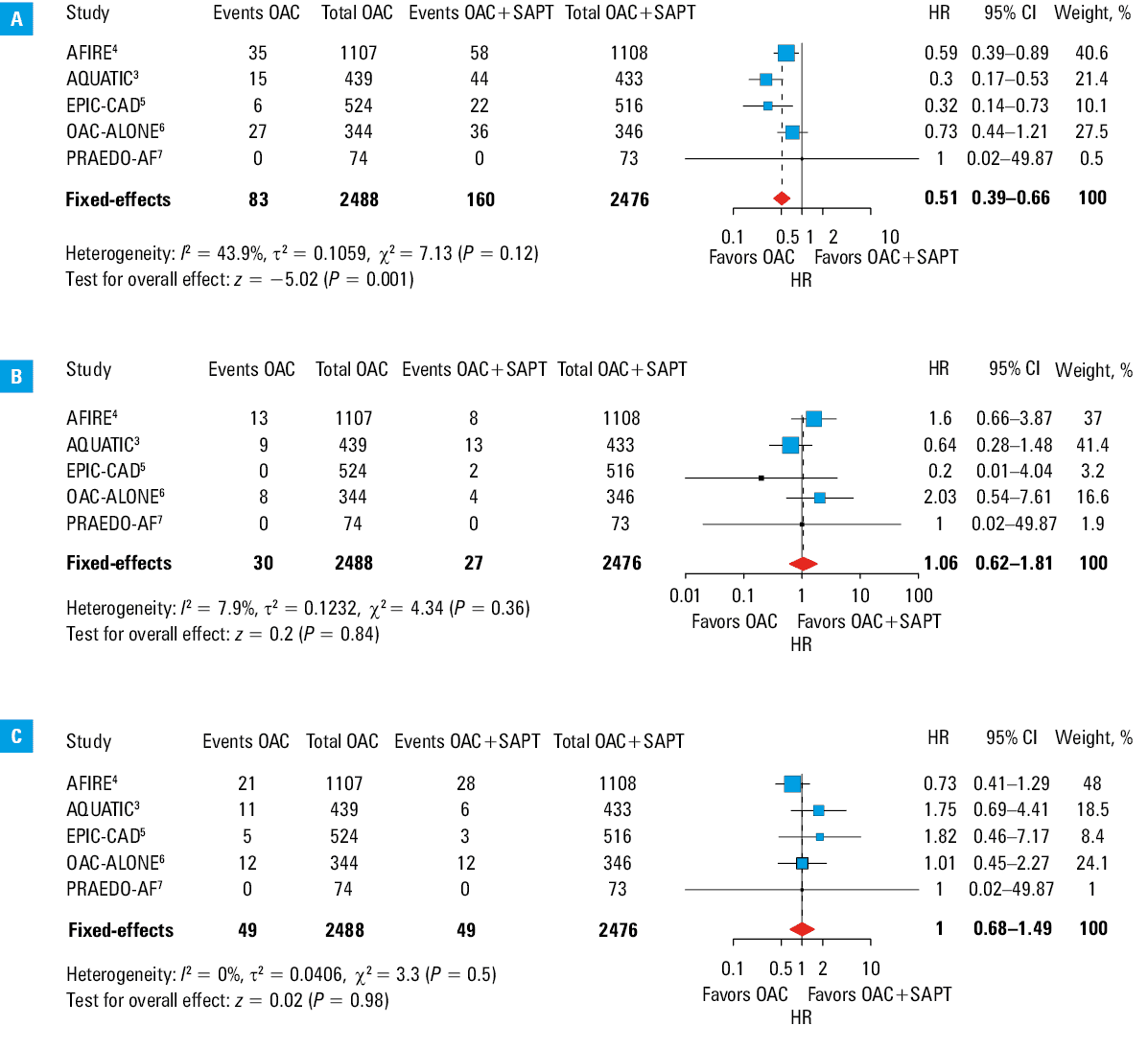
Data on major bleeding—defined in all trials according to the International Society on Thrombosis and Hemostasis—were available in all cases. Major bleeding occurred in 83 of 2488 patients in the OAC arm and in 160 of 2476 patients in the OAC+SAPT arm (3.3% vs 6.4%; I2 = 43.9%; HR, 0.51; 95% CI, 0.39–0.66; P <0.001; Figure 2A).
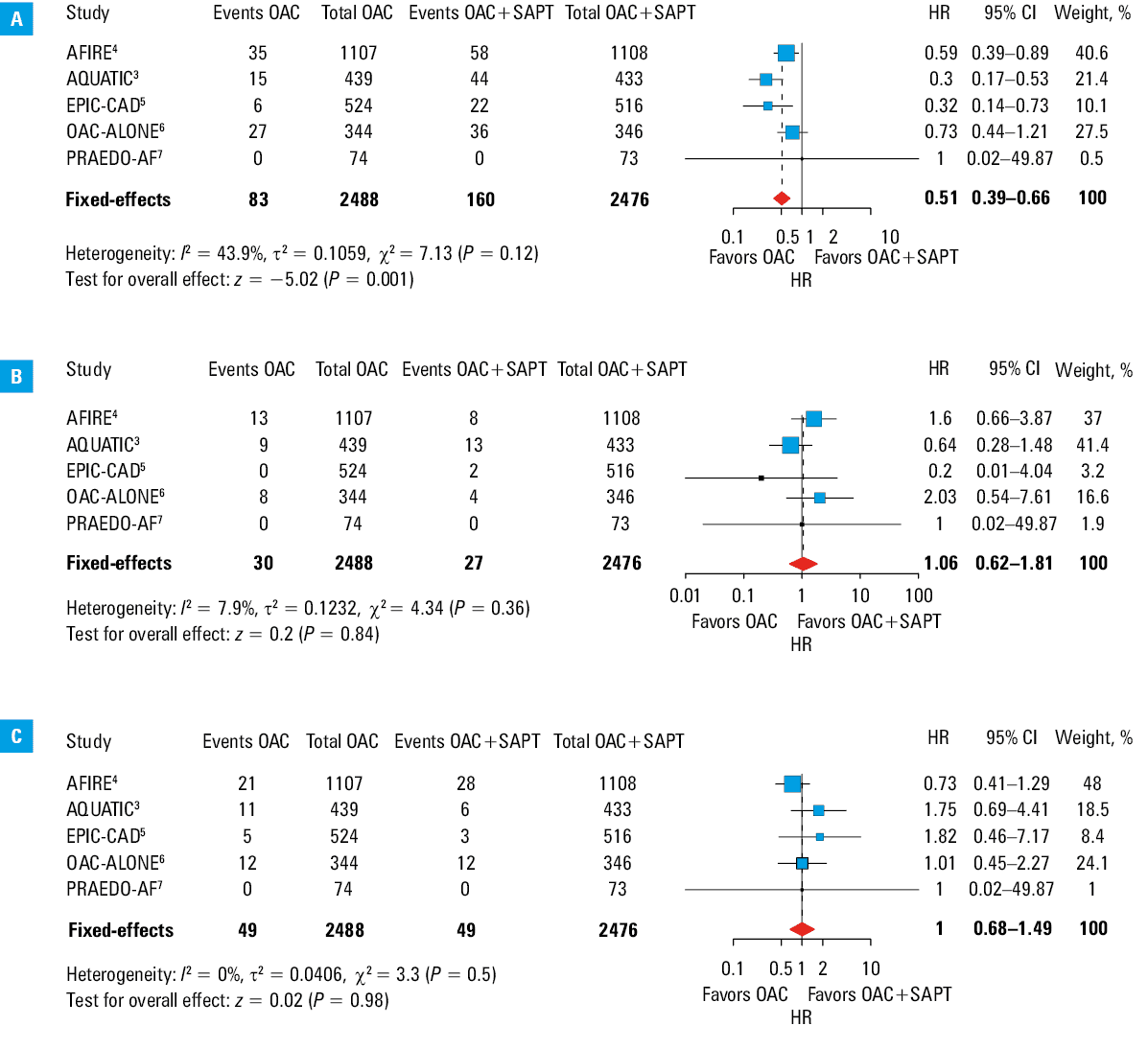
Nonfatal MI data were available in all trials. This outcome occurred in 30 of 2488 patients in the OAC arm and in 27 of 2476 patients in the OAC+SAPT arm, with a small difference (1.2% vs 1.1%; I2 = 7.9%; HR, 1.06; 95% CI, 0.62–1.81; P = 0.84; Figure 2B).
Nonfatal IS data were available in all trials. This outcome occurred in 49 of 2488 patients in the OAC arm vs 49 of 2476 patients in the OAC+SAPT arm (1.9% vs 1.9%; I2 = 0%; HR, 1; 95% CI, 0.68–1.49; P = 0.98; Figure 2C).
Publication bias and sensitivity analyses
Visual inspection of the funnel plots and Egger regression test (P = 0.34) suggested no significant publication bias for the primary outcome (Supplementary material, Figure S3) nor for any other outcome (Supplementary material, Figures S4–S8). A sensitivity analysis limited to the 4 East‑Asian trials,4-7 with exclusion of the AQUATIC trial,3 did not substantially change the HRs for cardiovascular death or major bleeding, which remained directionally and numerically similar to the overall estimates (Supplementary material, Table S3).
Discussion
This meta‑analysis is the first systematic evaluation to show reduced cardiovascular mortality, enhanced safety in terms of major bleeding, and no excess in major nonfatal ischemic events with OAC vs OAC+SAPT in patients with chronic CAD and a concomitant condition requiring long‑term anticoagulation. It differs from a previous work8 that summarized 4 randomized trials, by incorporating the more recent AQUATIC trial,3 by focusing a priori on cardiovascular mortality as the primary end point with time‑to‑event analyses, and by complementing conventional random‑effects pooling with the Bayesian and trial‑sequential methods, thereby narrowing the CIs for cardiovascular death and major bleeding, while confirming neutral effects on nonfatal MI and IS.
The reduction in cardiovascular mortality with OAC monotherapy is compelling, yielding a 31% relative risk reduction and an exploratory ARD of 1.1 percentage points over a median 2‑year follow‑up, resulting in a number needed to treat (NNT) of 94 to prevent 1 cardiovascular death (Figure 3). The findings, derived from the frequentist analyses and corroborated by the complementary Bayesian modeling to account for residual uncertainty, support the conclusions from recent trials that were underpowered to detect cardiovascular mortality as an individual end point. The concordance of the results across analytic paradigms increases confidence that the observed effect is not model‑dependent but reflects a true underlying effect.13 The Bayesian meta‑analysis indicates a 98.2% posterior probability that OAC alone reduces cardiovascular mortality, as compared with OAC+SAPT, complementing conventional CIs and providing useful information for patient‑centered discussions.14 The TSA further strengthened the validity of the finding. The cumulative Z‑score crossing the O’Brien–Fleming efficacy boundary provided evidence that sufficient statistical power was achieved to detect the observed treatment effect. TSA confirmation is particularly important in meta‑analyses, as it addresses concerns about random error and risks of false‑positive findings due to repeated testing across multiple studies.15 In the present analysis, TSA also addressed concerns about premature trial discontinuation. With the information‑size requirement exceeded, the conclusion that OAC monotherapy lowers cardiovascular mortality is unlikely to be significantly altered by further trials, supporting its translation into clinical practice and regulatory guidance.
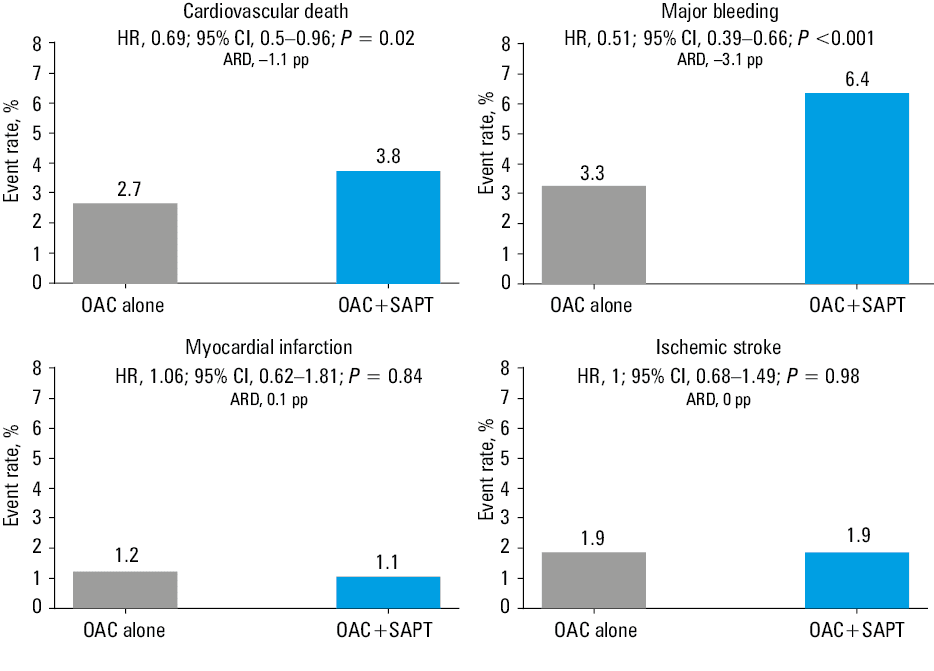
Abbreviations: ARD, absolute risk difference; CAD, coronary artery disease; pp, percentage points; others, see Table 1
The mechanism underlying the cardiovascular survival benefit with OAC alone appears multifactorial but is likely primarily driven by the substantial reduction in major bleeding observed in our analysis. The ARD of 3.1 percentage points for major bleeding—corresponding to 1 major bleeding event prevented for every 32 patients treated over the 2‑year period (Figure 3)—represents a substantial and meaningful reduction in bleeding risk across the trials. Major bleeding, especially intracranial and gastrointestinal, has consistently been associated with markedly increased short- and long‑term mortality across cardiovascular patient populations.16,17 Major bleeding may be directly fatal or—by triggering antithrombotic therapy discontinuation— may lead to fatal ischemic complications, supporting the concept that bleeding prevention translates directly into survival benefit.
The cardiovascular mortality benefit with OAC alone was achieved without any tradeoff in major nonfatal thrombotic events. The absence of significant differences in nonfatal MI (ARD, 0.1 percentage points) or nonfatal IS (ARD, 0 percentage points) rates between treatment strategies suggests that anticoagulant therapy alone provides adequate protection against both cardioembolic and atherothrombotic events in most patients (Figure 3). Indeed, historical evidence, accrued before the coronary intervention era, had demonstrated survival benefit of vitamin K antagonists over placebo,18 and comparable protection of OAC vs OAC+SAPT,2 in patients with previous MI. Importantly, the present data extend this concept to include DOACs.
Although the point estimate for all‑cause death favored OAC alone vs OAC+SAPT, the difference was not significant. The lack of significance may be related, at least in part, to competing causes of noncardiovascular deaths in older populations (eg, cancer, infections, frailty‑related cause, which are not uncommon in older patients and have grown over recent years). Competing risks of death can dilute the impact on all‑cause death of treatments directed specifically at cardiovascular mechanisms, blunting the observed differences and inflating the required sample size to detect a meaningful difference in all‑cause death rates.19 In comparison with a prior meta‑analysis,20 this one was prospectively centered on cardiovascular mortality as the primary end point and analyzed it as a time‑to‑event outcome using HRs rather than risk ratios (RRs). HRs leverage the full follow‑up, appropriately handling censoring and differing event times, whereas simple RRs on accrued counts can be biased when follow‑up durations vary or when early event timing is prognostically informative. This approach is consistent with established guidance for survival end points in meta‑analyses.21 The clinical relevance of modeling event time is underscored by the AFIRE4 and AQUATIC3 trials, which were stopped early for excess deaths in the antiplatelet arm during follow‑up—an example where early hazard separation matters and HRs are the appropriate effect measure. Of note, the inclusion of the AQUATIC trial,3 the largest European trial in this setting, importantly extended the previously entirely East‑Asian evidence base, and supported generalizability of our findings to European patients, despite differences in DOAC dosing patterns.
In the included RCTs, SAPT composition varied substantially across trials (Table 1): in AQUATIC trial,3 the dual‑therapy arm used aspirin 100 mg daily in all patients; in the AFIRE,4 EPIC‑CAD,5 and OAC‑ALONE6 studies, the OAC+SAPT arm received aspirin as the predominant agent, with clopidogrel (or other P2Y12 inhibitor) in a minority, whereas in the PRAEDO AF trial,7 the antiplatelet agent was clopidogrel. Despite this heterogeneity, the reduction in cardiovascular death and nonfatal major bleeding with OAC monotherapy was directionally consistent across SAPT regimens, and remained evident when the analysis was restricted to aspirin‑only dual‑therapy in the AQUATIC trial.3 These findings indicate that the cardiovascular death– and bleeding‑related benefits of OAC monotherapy are not confined to a specific SAPT agent. From an absolute‑risk perspective, cardiovascular death occurred in 2.7% of the patients assigned to OAC alone and 3.8% of those receiving OAC+SAPT, while major bleeding occurred in 3.3% and 6.4% of the patients, respectively. By contrast, the absolute risks of MI and IS were virtually identical in both groups (ARDs close to 0), indicating that the net clinical benefit of OAC monotherapy is driven by fewer fatal and major bleeding events without a loss of ischemic protection. In our study, the reduction in cardiovascular mortality with OAC alone was replicated in the Bayesian meta‑analysis (quantifying posterior uncertainty) and corroborated by TSA, where crossing of efficacy boundaries indicated that the evidence was conclusive rather than a product of random error.
Limitations
Several limitations of this study deserve consideration. Individual patient‑level data were not available for more detailed subgroup analyses. Four of 5 trials had an open‑label design and were conducted in Asian countries. On the other hand, clinical outcomes were adjudicated in a blind manner in all trials except PRAEDO AF,7 and the consistent mortality data between the Japanese AFIRE4 and the French AQUATIC3 trials support broad generalizability beyond East Asia.
Beyond corroborating current guidance, this analysis shows a cardiovascular survival advantage for OAC monotherapy, shifting the rationale from safety benefit alone to additional cardiovascular survival benefit. The quantitative risk‑benefit information provided by our analysis can inform shared decision‑making between patients and physicians.
Future research priorities should include defining the optimal time‑windows for transitioning to OAC alone from OAC plus antiplatelet therapy after acute coronary syndromes or PCIs, and confirming durability of the survival effect at longer follow‑up times.
Conclusions
In patients with AF or other indications for long‑term OAC and with concomitant chronic CAD in the absence of recent (<6 months) PCI, an OAC alone strategy is associated with a clear and consistent reduction in both cardiovascular death and nonfatal major bleeding, as compared with adding an antiplatelet agent. The reduced cardiovascular mortality signal is reproducible across randomized trials, robust at both frequentist and Bayesian analyses, and supported by trial sequential monitoring, indicating adequate information size for a stable inference. The findings support OAC monotherapy to reduce cardiovascular deaths and major bleeding without any substantial increase in nonfatal ischemic events for chronic CAD patients requiring long‑term anticoagulation.22-24
- Andreotti F, Geisler T, Collet JP, et al. Acute, periprocedural and longterm antithrombotic therapy in older adults: 2022 update by the ESC working group on thrombosis. Eur Heart J. 2023; 44: 262‑279. | Crossref
- Hurlen M, Abdelnoor M, Smith P, et al. Warfarin, aspirin, or both after myocardial infarction. N Engl J Med. 2002; 347: 969‑974. | Crossref
- Lemesle G, Didier R, Steg PG, et al. Aspirin in patients with chronic coronary syndrome receiving oral anticoagulation. N Engl J Med. 2025; 23: 1578‑1588. | Crossref
- Yasuda S, Kaikita K, Akao M, et al. Antithrombotic therapy for atrial fibrillation with stable coronary disease. N Engl J Med. 2019; 381: 1103‑1113. | Crossref
- Cho MS, Kang DY, Ahn JM, et al. Edoxaban antithrombotic therapy for atrial fibrillation and stable coronary artery disease. N Engl J Med. 2024; 39: 2075‑2086. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION