Hemophilia B (HB) is a congenital, X‑linked, bleeding disorder associated with IX clotting factor (FIX) deficiency. The standard of care is intravenous FIX replacement therapy, given on demand (for bleeds or before procedures) or as regular prophylaxis in patients with severe HB (FIX <1%). Replacement therapy, however vital, might predispose to thrombotic events,1 such as deep vein thrombosis and pulmonary embolism. Another thrombotic complication is central retinal vein occlusion (CRVO). Most common risk factors for CRVO are systemic, such as atherosclerosis, dyslipidemia, and arterial hypertension, but some ophthalmic diseases (glaucoma, hyperopia) may also contribute to CRVO pathogenesis.2 The role of hypercoagulable states is still under debate.2 CRVO management focuses on treating sight‑threatening complications, including macular edema, neovascularization, and secondary glaucoma; interventions reducing cardiovascular risk may be considered.2 To our knowledge, there is only 1 report of CRVO in a patient with HB, though with significant comorbidities (AIDS‑related cytomegalovirus retinitis).3
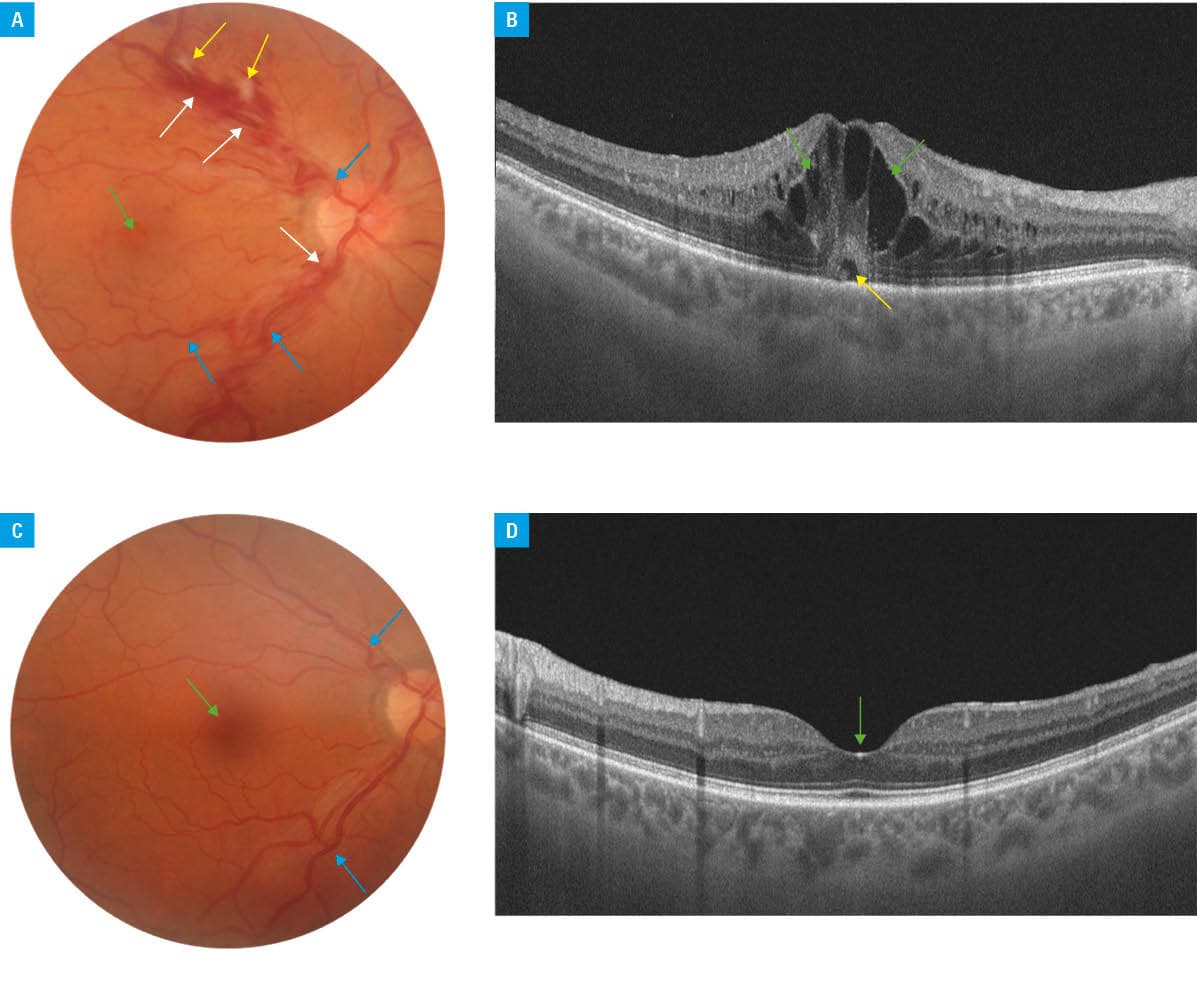
We present a case of a 51‑year‑old man with moderate HB (FIX activity, 6.5%; reference range, 65%–150%), who developed CRVO. Upon presentation, the patient complained of painless, sudden worsening of vision in the right eye. Ophthalmological examination demonstrated decreased best corrected visual acuity (BCVA) in the right eye (0.5 decimal) and normal BCVA in the left eye (1 decimal). Intraocular pressure was within normal limits bilaterally. Blood test results did not indicate hypercoagulability, showing normal activated partial thromboplastin time and prothrombin time. Since HB diagnosis at the age of 17, the patient had been experiencing bleeding events 2–3 times a year, including epistaxis and intra‑articular hemorrhages, and eventually developed hemophilic arthropathy. He was treated with FIX replacement therapy on demand. No FIX inhibitor developed. Recently, the patient was diagnosed with arterial hypertension and dyslipidemia that were treated with telmisartan, amlodipine, and rosuvastatin. Given the cardiovascular and ophthalmological presentation (Figure 1A–1D), a diagnosis of CRVO in the right eye was made. Hemophilia, though unlikely to cause CRVO, affected the treatment strategies through increasing the risk of hemorrhagic events following possible anticoagulant therapy. Multidisciplinary team (ophthalmologists and hematologists) abstained from such therapy, as its effectiveness in CRVO remains speculative.2,4 Intravitreal injection of an anti–vascular endothelial growth factor (VEGF) agent was recommended for macular edema, as a minimally‑invasive, effective, and low‑risk (in the general population) treatment option. As the exact incidence of hemorrhagic ocular complications of intravitreal injections in hemophiliacs is yet unknown, but a more severe course of bleeding has been reported,5 we implemented prophylaxis through administration of 7000 IU of FIX preceding the injection and 3500 IU daily on 2 following days. The patient required repeated injections of anti‑VEGF agents for recurrent cystoid macular edema, which were carried out under periprocedural FIX prophylaxis in the above‑described protocol without complications.
Anticoagulant therapy might be superior to antiplatelet therapy (acetylsalicylic acid) in achieving better BCVA and reducing recurrences with a similar risk of hemorrhagic complications, but the safety of prolonged anticoagulation is unknown and has not been assessed in hemostasis disorders.2 Interdisciplinary guidance and adequate prophylaxis with FIX replacement resulted in an uneventful invasive ophthalmic treatment course in our patient; however, clinical studies are needed to objectively assess this treatment strategy.
- Windyga J, Lassila R. Antithrombotic therapy in patients with inherited bleeding disorders: practical considerations. Pol Arch Intern Med. 2025; 135: 16993. | Crossref
- Valeriani E, Paciullo F, Porfidia A, et al. Antithrombotic treatment for retinal vein occlusion: a systematic review and meta‑analysis. J Thromb Haemost. 2023; 21: 284‑293. | Crossref
- Schiemann U, Steins M, Knospe V, et al. Coincidence of cytomegalovirus retinitis and central retinal vein occlusion in a patient with hemophilia B and AIDS. AIDS Patient Care STDs. 1999; 13: 7‑9. | Crossref
- Burggraaf JLI, Van Rein N, Klok FA, Cannegieter SC. How to predict recurrent venous thromboembolism and bleeding? A review of recent advances and their implications. Pol Arch Intern Med. 2023; 133: 16492. | Crossref
- Kesav N, Mehra AA, Schmaier AH, Sobol W. Severe subconjunctival hemorrhage after intravitreal injection in a patient with hemophilia A. J Vitreoretin Dis. 2023; 7: 333‑336. | Crossref
ARTICLE INFORMATION