Clinical outcomes after percutaneous coronary intervention with rotational atherectomy: insights from the RA-BIA cohort
Key words: coronary artery disease, percutaneous coronary intervention, rotational atherectomy, severely calcified coronary lesion

 CC BY 4.0
CC BY 4.0
Clinical outcomes after percutaneous coronary intervention with rotational atherectomy: insights from the RA-BIA cohort
Introduction: Severe coronary calcification remains one of the major challenges in percutaneous coronary intervention (PCI). Rotational atherectomy (RA) facilitates calcium modification, improving stent delivery and expansion, and may therefore enhance both procedural and long‑term outcomes.
Objectives: We aimed to evaluate the temporal trends, procedural performance, and short- and long‑term clinical outcomes of RA in patients with heavily calcified coronary artery disease treated with PCI over a 15‑year period in a single high‑volume center.
Patients and methods: Baseline characteristics, procedural outcomes, in‑hospital complications, and follow‑up were assessed. The primary end point was procedural and clinical success; the secondary end point included major adverse cardiovascular and cerebrovascular events (MACCEs; cardiovascular death, myocardial infarction, target vessel revascularization, stroke) at 24 months.
Results: Among 1060 patients (median [interquartile range] age, 74 [66–80] y), diabetes and chronic kidney disease were present in 42% and 31.1%, respectively, and 63.8% had prior PCI. Multivessel disease was diagnosed in 36.4%, and 29.4% had the SYNTAX I value equal to or above 32. Technical and clinical success were 97.6% and 86.2%, respectively. Thirty‑day MACCE rate was 10.9%, while at 24 months the MACCE rate was 38.3% and all‑cause mortality rate was 19.4% (cardiovascular, 14.2%). Estimated glomerular filtration rate below 30 ml/min/1.73 m² (subdistribution hazard ratio [sHR], 1.61; 95% CI, 1.11–2.35; P = 0.01) and each 10‑point increase in the SYNTAX I score (sHR, 1.13; 95% CI, 1.04–1.23; P = 0.005) predicted higher MACCE rate, whereas higher left ventricular ejection fraction was protective (sHR, 0.984 per 5% increase; P <0.001). Isolated postprocedural troponin rise was not independently associated with outcomes (sHR, 1.22; P = 0.07).
Conclusions: RA provides high procedural success even in the most complex lesions and remains an essential tool in contemporary PCI.
What's new?
This 15‑year registry provides new insights into the real‑world use of rotational atherectomy (RA) in patients with severely calcified coronary artery disease. The study shows that early and long‑term outcomes are strongly influenced by patient frailty and renal impairment rather than procedural factors. Importantly, elevated troponin levels after RA were not linked to worse prognosis, while achieving full procedural success markedly improved survival. These findings suggest that careful patient selection and optimization of comorbid conditions may be as crucial as technical aspects of the procedure. In the era of expanding calcium‑modification technologies, RA remains an indispensable, safe, and effective option for treating complex calcified lesions, especially when guided by intravascular imaging.

Introduction
Severe coronary artery calcification is a strong, independent predictor of adverse cardiovascular outcomes.1 Although the risk factors and pathophysiological mechanisms underlying severe calcification are well established, effective treatment options remain limited.2,3
In the presence of heavy calcification, conventional percutaneous coronary intervention (PCI) is associated with suboptimal acute and long‑term results.4,5 Immediate procedural challenges include difficulty in achieving adequate vessel dilatation, delivering the stent, and ensuring optimal stent expansion and apposition. These technical complexities may lead to PCI‑related complications, such as coronary dissection, acute thrombosis, vessel perforation, and coronary flow disturbances. Early procedural risks and technical shortcomings translate into higher rates of adverse clinical events during follow‑up. Indeed, 1‑year rates of all‑cause death, cardiac death, definite stent thrombosis, and ischemic target lesion revascularization (TLR) increase proportionally with the severity of coronary calcification.6
To improve both procedural success and long‑term clinical outcomes, advanced lesion modification is essential. Specialized devices, either balloon- or ablation‑based, target calcified deposits with the aim of creating controlled cracks and fractures in the plaque, thereby enhancing vessel compliance and facilitating optimal stent deployment.7 In this regard, rotational atherectomy (RA) is the earliest and most extensively studied modality.8-12 However, RA has been evaluated in only 220 patients across 2 randomized clinical trials with only up to 9 months of follow‑up,11,12 which most likely contributes to the relatively weak strength of official guideline recommendations for its use.13,14 Conversely, large‑scale real‑world data involving substantial patient cohorts consistently indicate that RA is indispensable for achieving favorable clinical outcomes.
We present a single‑center, registry‑based prospective observational study of patients treated with PCI and RA between 2008 and 2022, with 24‑month follow‑up, aimed at describing temporal trends in RA utilization and associated clinical outcomes.
Patients and methods
Study cohort
This registry‑based prospective observational cohort comprised 1060 consecutive patients who underwent PCI with RA at the Department of Invasive Cardiology, Medical University of Białystok, Poland, between April 16, 2008 and December 28, 2022. Eligibility criteria required that the RA was performed or unequivocally attempted during PCI, and that key clinical / procedural data were available. The decision to perform RA was based on either angiographic evidence of moderate / severe calcification (the presence of radiopaque densities [visible calcium] on both sides of the arterial wall, apparent during the cardiac cycle or without cardiac motion before contrast injection) or the presence of undilatable calcified plaques. No restrictions were applied with respect to the initial patient clinical presentation. Every patient potentially eligible for surgery was discussed within the local heart team. The cohort was drawn predominantly from Podlaskie voivodeship (n = 872; 82.3%) and the adjacent Warmińsko‑Mazurskie voivodeship (n = 150; 14.2%).
Follow‑up was prespecified at 24 months for all participants and was administratively closed on June 26, 2025. Outcomes were ascertained using mixed methods: structured telephone interviews (where reachable), linkage to National Health Fund databases, and the Statistics Poland national mortality registry. All patients completed 24‑month follow‑up; therefore, no imputation or early censoring was required. Screening, exclusions, and patient flow are summarized in Figure 1.
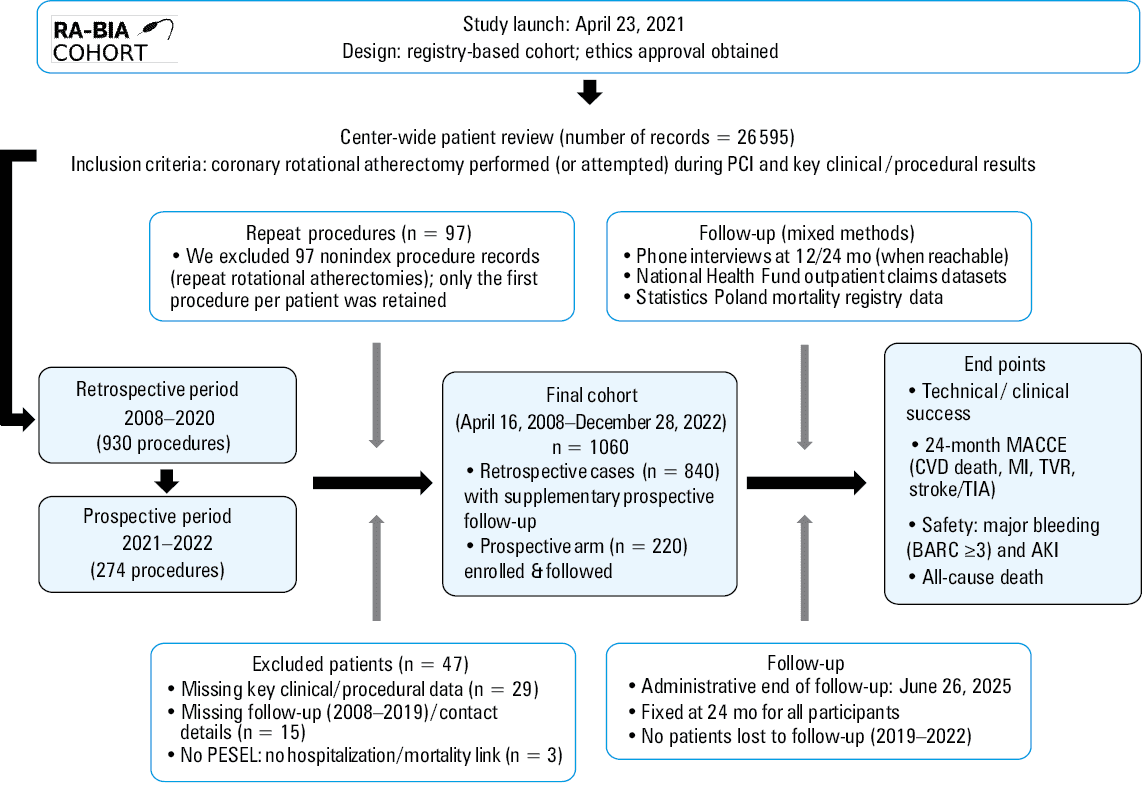
Abbreviations: AKI, acute kidney injury; BARC, Bleeding Academic Research Consortium; CVD, cardiovascular disease; MACCE, major adverse cardiovascular and cerebrovascular event; MI, myocardial infarction; PCI, percutaneous coronary intervention; PESEL, Polish national identification number; TIA, transient ischemic attack; TVR, target vessel revascularization
Study definitions
The anatomic SYNTAX I score was calculated from diagnostic coronary angiography by trained physicians using the official SYNTAX score online calculator. Prognostic estimates and surgical risk were obtained from the SYNTAX II score 2020 and the Society of Thoracic Surgeons Adult Cardiac Surgery Risk Calculator, respectively, using their official online calculators.
Periprocedural myocardial infarction (PMI) was defined according to the 2018 Fourth Universal Definition of Myocardial Infarction.15 In stable coronary artery disease (CAD), PMI required a rise in high‑sensitivity cardiac troponin I (hs‑cTnI) to at least 5 times the 99th‑percentile upper reference limit together with ischemic symptoms, new ischemic electrocardiographic (ECG) changes, or new regional wall‑motion abnormalities. In acute coronary syndromes (ACS), PMI was defined as a further at least 20% increase in troponin from an already elevated baseline, consistent with the Euro4C registry. All events were re‑evaluated according to the 2018 criteria.15 In practice, hs‑cTnI tests were routinely implemented in 2015, while previous hospitalizations were assessed using conventional troponin tests.
Baseline renal function was quantified as estimated glomerular filtration rate (eGFR) using the race‑free chronic kidney disease epidemiology collaboration 2021 creatinine equation (ml/min/1.73 m2). Chronic kidney disease (CKD) was defined as eGFR below 60 ml/min/1.73 m2. Acute kidney injury (AKI) was defined per Kidney Disease: Improving Global Outcomes 2012 guidelines as an increase in serum creatinine of at least 0.3 mg/dl within 48 hours or at least 1.5 times over the baseline value within the prior 7 days; urine‑output criteria were not applied due to data unavailability.
Abnormal liver function was defined as chronic liver disease or clinically significant biochemical derangement: total bilirubin over 2 times the upper limit of normal (ULN) in conjunction with alanine aminotransferase, aspartate aminotransferase, or alkaline phosphatase over 3 times the ULN. Anemia was considered present if baseline hemoglobin was below 13 g/dl in men or below 12 g/dl in women. Thrombocytopenia was considered present if the baseline platelet count was below 150 × 109/l (ie, <150 000/µl). Poor mobility was defined according to the European System for Cardiac Operative Risk Evaluation II (EuroSCORE II) criteria.
Major bleeding was defined according to the Bleeding Academic Research Consortium criteria, grades 3–5.
Interventional procedure
All PCIs with RA were performed by experienced operators, with the treatment strategy left entirely to their discretion. Following the publication of the first expert consensus on RA,16,17 the recommended standardized protocol for RA became the preferred approach. All RA procedures were performed using the Rotablator RA system (Boston Scientific, Marlborough, Massachusetts, United States). Antiplatelet therapy and periprocedural anticoagulation were used according to existing guidelines at the time of the procedure. All patients were recommended lifelong low‑dose aspirin and dual antiplatelet therapy for a minimum of 12 months after stent implantation.
Study outcomes and end points
The primary end point was the procedural and clinical success rate of the RA procedure. Technical success was defined as completing lesion modification with RA with subsequent stent placement with up to 20% residual stenosis on angiography. Clinical success was defined as the achievement of technical success in the absence of major in‑hospital complications, including PMI, AKI, cardiac tamponade, emergency surgery, major bleeding, atrioventricular block requiring temporary pacemaker implantation, coronary perforation requiring stent‑graft implantation, no‑flow phenomenon, in‑hospital stroke, or in‑hospital death.
The major secondary end point was the incidence of major adverse cardiovascular and cerebrovascular events (MACCEs) at 24 months, defined as a composite of cardiovascular death, MI, target vessel revascularization, and stroke.
Secondary analyses further evaluated the individual components of the secondary end point, as well as the occurrence of AKI and all‑cause mortality.
All secondary outcomes were reported across the following a priori defined strata: age (≥65 vs <65 y), clinical presentation (ACS vs chronic coronary syndrome [CCS]), operative risk (EuroSCORE II ≥5 vs <5), anatomic complexity (SYNTAX I score ≥32 vs <32), and use of intravascular imaging (IVI) guidance during the index PCI (yes vs no), with IVI defined as intravascular ultrasound (IVUS) or optical coherence tomography (OCT). Subgroup analyses were prespecified and considered exploratory.
Statistical analysis
Normality of distribution was assessed using the Kolmogorov–Smirnov test. Continuous variables were summarized as median with interquartile range (IQR) and categorical variables as counts (percentages). Comparisons between 2 groups were performed with the Mann–Whitney test. Categorical variables were compared using the χ2 test.
Temporal trends were evaluated with the nonparametric Mann–Kendall test using the Hamed–Rao variance correction for autocorrelation. Trend strength was summarized with Kendall τ, and magnitude by Sen’s slope. To aid visualization, we overlaid an exponential curve fit with its regression equation (for display only). For descriptive comparisons across calendar time, we also split the cohort into an early era (2008–2017) and a late era (2018–2022).
To estimate associations with time to first MACCE, we fitted multivariable Cox proportional hazards models (Breslow method for ties) and reported hazard ratios (HRs) with 95% CIs. Covariate selection was prespecified on clinical grounds and prior literature, and the same adjustment set was used in all Cox models to enable a fair comparison of coronary disease burden metrics. Missing covariates were handled using multiple imputations by chained equations under a missing‑at‑random assumption (40 imputations; seed = 7); continuous variables were imputed with linear regression and binary variables with logistic regression. Outcome status and follow‑up time were not imputed. Estimates and SEs were combined across imputations using the Rubin’s rules.
We compared 2 alternative encodings of coronary disease burden within otherwise identical adjustment sets, that is, Model A: SYNTAX I score, per 10‑point increase (continuous), Model B: 1-, 2-, or 3‑vessel disease (categorical; 1‑vessel as reference).
All Cox models were adjusted for sex, current smoking, poor mobility, anemia, atrial fibrillation, peripheral artery disease, diabetes, ACS at presentation, chronic total occlusion, age (per 10‑year increase), ejection fraction (per 5‑percentage‑point increase), body mass index (BMI, kg/m2), and kidney function by eGFR categories (<30, 30–44, 45–59, and ≥60 ml/min/1.73 m2). The proportional‑hazards assumption was assessed using the Schoenfeld residuals; the global proportional hazards test was not violated in either model (borderline variable‑specific signals only; in Model A: ejection fraction, P = 0.03; SYNTAX, P = 0.04). Discrimination and parsimony for the Cox models were summarized using the Harrell C and the Akaike information criterion (AIC): Model A with C = 0.67, AIC = 5166 and Model B with C = 0.64, AIC = 5334.
For prognostic interpretation, we used the Fine–Gray subdistribution model, restricting analyses to the patients discharged alive, so that the results reflect postdischarge outcomes. The subdistribution HRs (sHRs) with 95% CIs account for the competing risk of noncardiac death. Model performance was summarized with AIC and Harrell C derived from the linear predictor: AIC = 4917.4; Harrell C approximately 0.62. In the final Fine–Gray model, there were no missing values (complete‑case set).
Cumulative incidence functions were plotted to show event probabilities over time, and the Gray test was used for univariable comparisons of cumulative incidence functions between the groups.
All tests were 2‑sided with a P value below 0.05 considered significant. The analyses were performed in Stata software (version 19.5; StataCorp, College Station, Texas, United States).
The study is registered at ClinicalTrials.gov (NCT05787886). The protocol adhered to the 1975 Declaration of Helsinki and followed STROBE reporting guidelines; ethical approval was granted by the Bioethics Committee of the Medical University of Bialystok (APK.002.421.2022). Written informed consent was obtained from all prospectively enrolled participants.
Results
Baseline patient characteristics
Baseline characteristics of the study population are summarized in Table 1. The final cohort consisted of 1060 patients, at a median (IQR) age of 74 (66–80) years, of whom 358 were women (33.8%). CKD was present in 330 (31.13%), and diabetes mellitus in 437 (42.02%) of the patients. A history of prior PCI was reported in 663 cases (63.8%). Multivessel disease was observed in 386 patients (36.4%), and the SYNTAX I score of 32 or higher was documented in 306 individuals (29.39%). The presentation was stable for 899 patients (84.8%), while 26 (2.5%) presented with ST‑segment elevation myocardial infarction (STEMI), and 135 (12.7%) with non‑STEMI (NSTEMI). Almost one‑third (n = 302; 28.5%) had EuroSCORE II value of 5 or higher.
Parameter | N | Value | |
Data are presented as number (percentage) or median (interquartile range) unless indicated otherwise.
Abbreviations: 1VD, 1‑vessel disease; 2VD, 2‑vessel disease; ACS, acute coronary syndrome; BMI, body mass index; CABG, coronary artery bypass grafting; CCS, chronic coronary syndrome; DM, diabetes mellitus; eGFR, estimated glomerular filtration rate; EuroSCORE II, European System for Cardiac Operative Risk Evaluation II; LVEF, left ventricular ejection fraction; MVD, multivessel disease; NSTEMI, non–ST‑segment elevation myocardial infarction; STEMI, ST‑segment elevation myocardial infarction; STS, Society of Thoracic Surgeons (risk score); others, see Figure 1 | |||
Clinical characteristics | |||
Age, y | 1060 | 74 (66–80) | |
BMI, kg/m2 | 929 | 28 (25–31) | |
Men | 1060 | 702 (66.2) | |
Hypertension | 1042 | 975 (93.6) | |
DM | 1040 | 437 (42) | |
Insulin‑requiring DM | 1041 | 164 (15.7) | |
Chronic kidney disease | 1060 | 330 (31.1) | |
eGFR, ml/min/1.73 m² | 1060 | 71.3 (52.5–86.45) | |
Dialysis | 1060 | 29 (2.7) | |
Atrial fibrillation | 1042 | 289 (27.7) | |
Peripheral artery disease | 1041 | 223 (21.4) | |
Current smoker | 982 | 134 (13.6) | |
Poor mobility | 1060 | 156 (14.7) | |
Anemia | 1050 | 437 (41.6) | |
Thrombocytopenia | 1050 | 134 (12.9) | |
LVEF, % | 1060 | 48 (38–55) | |
LVEF subgroups | <35 | 1060 | 226 (21.3) |
35–49 | 345 (32.6) | ||
≥50 | 489 (46.1) | ||
Previous ACS | 1041 | 509 (48.9) | |
Previous PCI | 1039 | 663 (63.8) | |
Previous CABG | 1039 | 115 (11) | |
Previous ischemic stroke | 1040 | 97 (9.3) | |
Clinical presentation and angiographic characteristics | |||
CCS | 1060 | 899 (84.8) | |
NSTEMI | 135 (12.7) | ||
STEMI | 26 (2.5) | ||
1VD, % | 1060 | 334 (31.5) | |
2VD, % | 340 (32.1) | ||
MVD, % | 386 (36.4) | ||
EuroSCORE II | 1060 | 2.46 (1.25–5.49) | |
EuroSCORE II ≥5 | 1060 | 302 (28.49) | |
SYNTAX I | 1041 | 24 (17–34) | |
SYNTAX I ≥32 | 1041 | 306 (29.39) | |
SYNTAX 2020, 5 y MACCE for PCI | 1044 | 28.6 (18.4–43.2) | |
SYNTAX 2020, 10 y mortality for PCI | 1044 | 45.8 (26.7–70.1) | |
STS mortality | 857 | 1.59 (0.83–3.27) | |
STS mortality / morbidity | 857 | 7.86 (5.05–12.9) | |
Angiographic characteristics and rotablation procedure
Majority of the patients (n = 877; 82.7%) were qualified for RA based on angiographic evidence of moderate‑to‑severe coronary calcification. IVI was used infrequently, although its utilization increased substantially after 2016 (Supplementary material, Figure S1). RA was performed as a bailout strategy when the lesion could not be crossed with any balloon (9.2%) or when it remained inadequately dilatable (8%). The radial approach was employed in 853 procedures (80.5%). Target lesions were most frequently located in the left anterior descending artery (n = 532; 50.2%), with a substantial proportion involving the left main artery (LM; n = 167; 15.7%). Bifurcation lesions were present in 400 patients (37.7%), most commonly classified as Medina 1–1–1 (50.3%) or Medina 1–1–0 (23%). Glycoprotein IIb/IIIa inhibitors were used in 90 cases (8.49%). Temporal pacing was not planned in advance in any procedure. Detailed procedural characteristics are presented in Table 2.
Parameter | N | Value | |
Procedural indications | |||
Data are presented as number (percentage) or median (interquartile range).
Abbreviations: Cx, circumflex artery; Diag, diagonal branch; IVL, intravascular lithotripsy; IVUS, intravascular ultrasound; LAD, left anterior descending artery; LM, left main coronary artery; OM, obtuse marginal branch; OCT, optical coherence tomography; RA, rotational atherectomy, RCA, right coronary artery; TIMI, thrombolysis in myocardial infarction; others, see Figure 1 | |||
Calcification severity | Moderate | 1060 | 355 (33.5) |
Severe | 705 (66.5) | ||
Primary strategy | 1060 | 877 (82.7) | |
Secondary strategy, uncrossable lesion | 98 (9.2) | ||
Secondary strategy, undilatable lesion | 85 (8) | ||
Number of treated vessels | |||
1 | 1060 | 891 (84.1) | |
2 | 157 (14.8) | ||
3 | 12 (1.1) | ||
Treated vessels | |||
LM | 1060 | 15 (1.4) | |
LM/LAD | 57 (5.4) | ||
LM/Cx | 31 (2.9) | ||
LM/LAD/Cx | 82 (7.7) | ||
LAD | 532 (50.2) | ||
Diag | 89 (8.4) | ||
Cx | 120 (11.3) | ||
OM | 52 (5) | ||
RCA | 262 (24.7) | ||
Bifurcation | 400 (37.7) | ||
Chronic total occlusion | 88 (8.3) | ||
Procedural details | Radial | 1060 | 853 (80.5) |
Femoral | 204 (19.2) | ||
Other access | 3 (0.3) | ||
Wire delivery, n | Direct | 1060 | 926 (87.4) |
Microcatheter | 134 (12.6) | ||
Total number of stents | 1060 | 2 (1–2) | |
Stent diameter, mm | 3 (3–4) | ||
Total stent length, mm | 48 (33–64) | ||
Number of burrs | 1051 | 1 (1–1) | |
Escalation of burrs | 62 (5.89) | ||
Burr size, mm | 1052 | 1.5 (1.5–1.5) | |
Max burr speed, 1000 rpm | 551 | 176 (166–183) | |
TIMI post PCI | 1060 | 3 (3–3) | |
Time of RA, s | 511 | 62.5 (38–100) | |
Radiation dose, mGy | 652 | 1329 (845–2065) | |
Contrast volume, ml | 644 | 200 (170–250) | |
Imaging | IVUS | 1060 | 132 (12.5) |
OCT | 13 (1.26) | ||
Additional devices | Scoring balloon | 1060 | 43 (4) |
Cutting balloon | 42 (4) | ||
IVL | 4 (0.4) | ||
Procedural completeness and staging | Scheduled for staged RA | 1060 | 56 (5.3) |
Scheduled for staged PCI | 152 (14.3) | ||
Temporal trends across the study period
As compared with the early era (2008–2017), the patients treated in the late era (2018–2022) were older (median, 73 vs 74 years; P = 0.01) and presented with a higher baseline risk and anatomical complexity (EuroSCORE II, 2.2 vs 2.7; P <0.001; SYNTAX I, 23 vs 25; P = 0.049), with more frequent ACS presentations (11.9% vs 17.9%; P = 0.007), and a numerically greater chronic total occlusion burden (6.9% vs 9.5%; P = 0.14). The use of IVI increased substantially (IVUS/OCT, 8.8% vs 17.5%; P <0.001; Supplementary material, Figure S1 and Table S1).
Technical and clinical success with short‑term complications
The rate of technical success was 97.5%, while clinical success was achieved in 86.2% of the cases. Any postprocedural rise in hs‑cTnI was observed in as many as 434 patients (40.9%); however, per definition of MI, this required an accompanying clinical or diagnostic criterion. Accordingly, PMI was ultimately confirmed in 60 patients (5.66%), based on the presence of chest pain in 173 cases (16.3%), new ischemic ECG changes in 78 cases (7.4%), or new regional wall motion abnormalities in 39 cases (3.7%). At 30 days, the overall MACCE rate was 10.9%. EuroSCORE II of 5 or higher was associated with greater all‑cause and cardiovascular mortality (5.63% vs 1.45%; P <0.001; 4.3% vs 1.2%; P = 0.001, respectively) and more frequent AKI (8.94% vs 2.11%; P <0.001), while the SYNTAX I score equal to or higher than 32 indicated higher MACCE (14.7% vs 9.3%; P = 0.01) and all‑cause mortality rates (4.25% vs 1.77%; P = 0.02; Table 3, Supplementary material, Table S2).
Parameter | Entire cohort | EuroSCORE II <5 (n = 758) | EuroSCORE II ≥5 (n = 302) | P value | SYNTAX I <32 (n = 735) | SYNTAX I ≥32 (n = 306) | P value |
Data are presented as number (percentage).
| |||||||
Technical success | 1034 (97.5) | 738 (97.3) | 296 (98) | 0.54 | 718 (97.7) | 298 (97.4) | 0.77 |
Burr entrapment | 5 (0.5) | 4 (0.5) | 1 (0.3) | 0.67 | 1 (0.1) | 3 (0.9) | 0.04 |
Unsuccessful RA | 15 (1.4) | 12 (1.6) | 3 (0.9) | 0.46 | 12 (1.6) | 3 (0.9) | 0.42 |
Stent delivery failure | 26 (2.4) | 20 (2.6) | 6 (1.9) | 0.54 | 17 (2.3) | 8 (2.6) | 0.77 |
Clinical success | 914 (86.2) | 660 (87.1) | 254 (84.1) | 0.21 | 642 (87.3) | 256 (83.7) | 0.12 |
Periprocedural MI | 60 (5.7) | 53 (6.9) | 7 (2.3) | 0.003 | 40 (5.4) | 19 (6.2) | 0.63 |
Acute kidney injury | 39 (3.7) | 13 (1.7) | 26 (8.6) | <0.001 | 22 (2.9) | 16 (5.2) | 0.08 |
Tamponade | 5 (0.5) | 4 (0.5) | 1 (0.3) | 0.67 | 4 (0.5) | 1 (0.3) | 0.64 |
Emergency surgery | 6 (0.5) | 3 (0.4) | 3 (0.9) | 0.24 | 2 (0.3) | 3 (0.9) | 0.13 |
Major bleeding | 10 (0.9) | 6 (0.8) | 4 (1.3) | 0.42 | 5 (0.7) | 4 (1.3) | 0.32 |
AV block requiring temporary pacing | 6 (0.6) | 4 (0.5) | 2 (0.7) | 0.79 | 5 (0.7) | 1 (0.33) | 0.49 |
Perforation requiring stent‑graft) | 15 (1.4) | 13 (1.7) | 2 (0.7) | 0.19 | 12 (1.6) | 3 (0.9) | 0.42 |
No flow | 4 (0.4) | 3 (0.4) | 1 (0.3) | 0.88 | 4 (0.5) | 0 | 0.19 |
In‑hospital stroke / TIA | 2 (0.2) | 2 (0.3) | 0 | 0.37 | 1 (0.1) | 1 (0.3) | 0.52 |
In‑hospital death | 14 (1.3) | 4 (0.5) | 10 (3.3) | <0.001 | 7 (0.9) | 6 (1.9) | 0.18 |
Long‑term clinical outcomes and prognostic modelling
In the baseline Cox models for MACCE, multivessel disease was associated with a higher risk (HR, 1.404; 95% CI, 1.076–1.832; P = 0.01), whereas 2‑vessel disease showed only a borderline signal (HR, 1.295; 95% CI, 0.995–1.686; P = 0.05). When anatomical complexity was modeled with the SYNTAX I score, each 10‑point increase was related to a higher risk of MACCE (HR, 1.155; 95% CI, 1.059–1.26; P = 0.001). Severely reduced kidney function (eGFR <30 ml/min/1.73 m2) consistently predicted negative outcomes (model without SYNTAX I: HR, 1.639; 95% CI, 1.164–2.306; P = 0.005; SYNTAX I‑adjusted model: HR, 1.593; 95% CI, 1.124–2.256; P = 0.009). Poor mobility was significant in both specifications (HR, 1.402; 95% CI, 1.092–1.800; P = 0.008 without SYNTAX I and HR, 1.368; 95% CI, 1.044–1.793; P = 0.02 for SYNTAX I‑adjusted; Figure 2A and 2B).
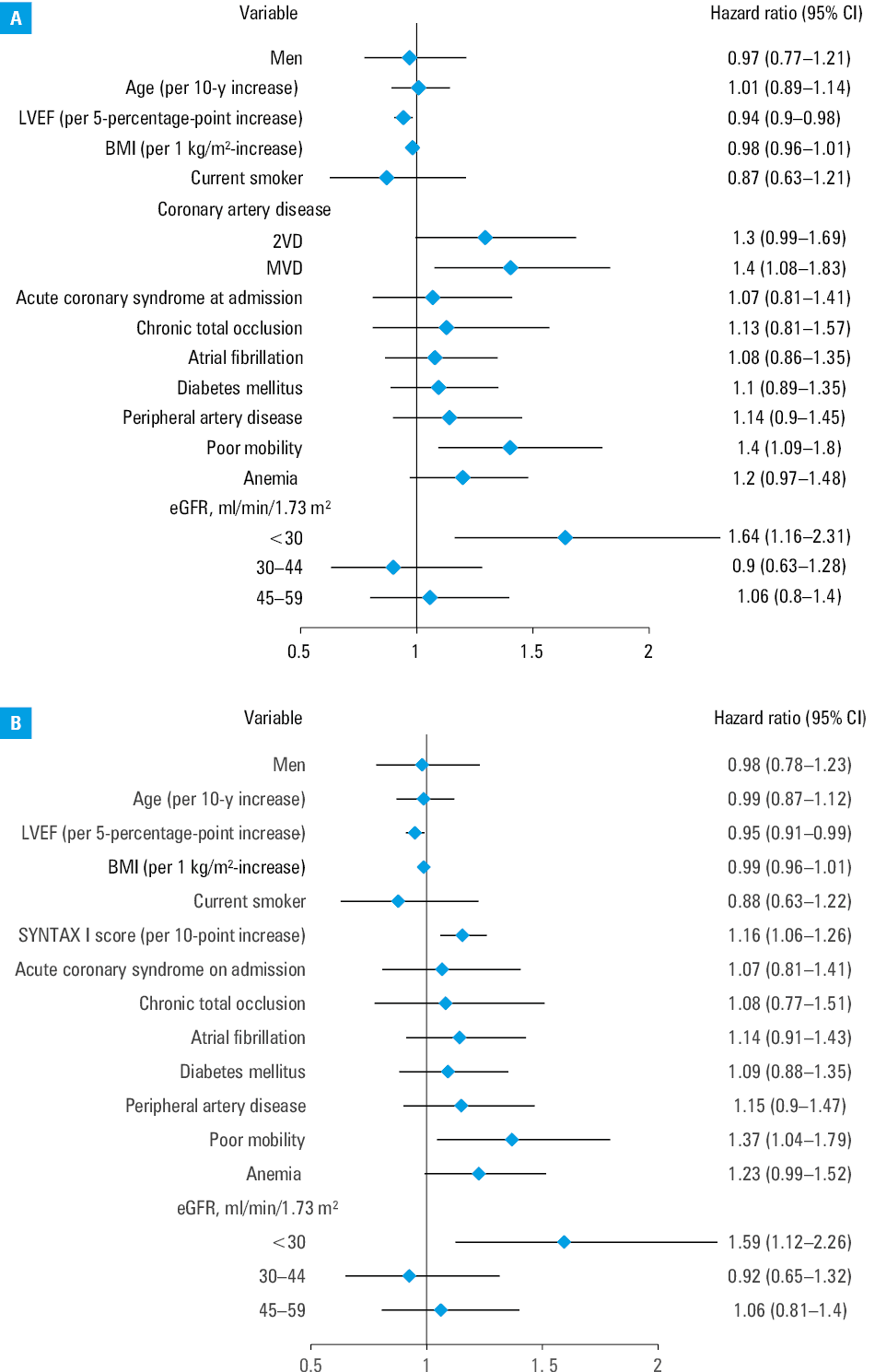
Abbreviations: see Table 1
In the Fine–Gray model for long‑term MACCE, the strongest independent predictors were again renal failure and anatomical / physiological complexity. eGFR value below 30 ml/min/1.73 m2 carried sHR of 1.612 (95% CI, 1.106–2.35; P = 0.01). Each 10‑point SYNTAX I increase was associated with a higher risk (sHR, 1.13; 95% CI, 1.037–1.231; P = 0.005), while higher left ventricular ejection fraction was modestly protective (sHR, 0.984 per 5‑percentage‑point increase; 95% CI, 0.976–0.993; P <0.001). Poor mobility (sHR, 1.336; 95% CI, 1.016–1.756; P = 0.04) and TIMI 0 preprocedure signaled worse outcomes (sHR, 1.753; 95% CI, 1.028–2.989; P = 0.04). Achieving clinical success was independently protective (sHR, 0.722; 95% CI, 0.557–0.937; P = 0.01). An isolated postprocedural hs‑cTnI rise showed only a weak, nonsignificant association with later MACCE (sHR, 1.224; 95% CI, 0.981–1.528; P = 0.07; Figure 3).
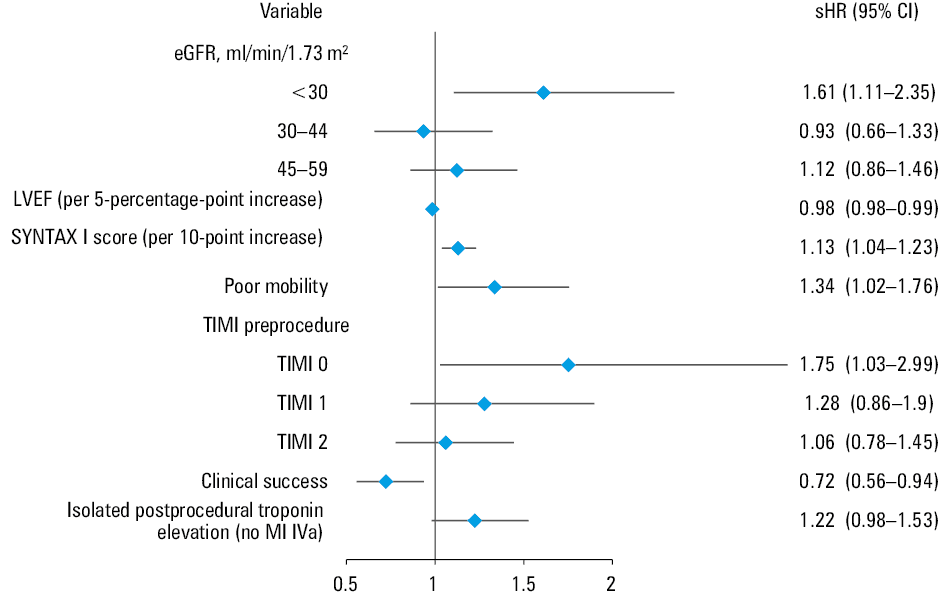
Abbreviations: sHR, subdistribution hazard ratio; others, see Figure 1 and Table 1
At 30‑day follow‑up, the patients with EuroSCORE II of 5 or above had higher rates of cardiovascular death (4.3% vs 1.2%; P = 0.001), all‑cause death (5.6% vs 1.5%; P <0.001), and AKI (8.9% vs 2.1%; P <0.001). Similarly, in the patients with SYNTAX I score of 32 or higher, MACCE (14.7% vs 9.3%; P = 0.01), all‑cause death (4.3% vs 1.8%; P = 0.02), and cardiovascular death (3.3% vs 1.4%; P = 0.04) occurred more frequently.
At 2 years, EuroSCORE II of at least 5 was associated with higher rates of MACCE (48.3% vs 34.3%; P <0.001), cardiovascular death (28.2% vs 8.6%; P <0.001), all‑cause death (35.1% vs 13.2%; P <0.001), and AKI (11.9% vs 5.7%; P <0.001). In the patients with SYNTAX I score of 32 or above, a higher incidence of MACCE (46.1% vs 35%; P <0.001), MI (22.9% vs 15.4%; P = 0.004), ischemic stroke / transient ischemic attack (3.9% vs 1.2%; P = 0.005), and all‑cause death (24.8% vs 16.9%; P = 0.003) was observed.
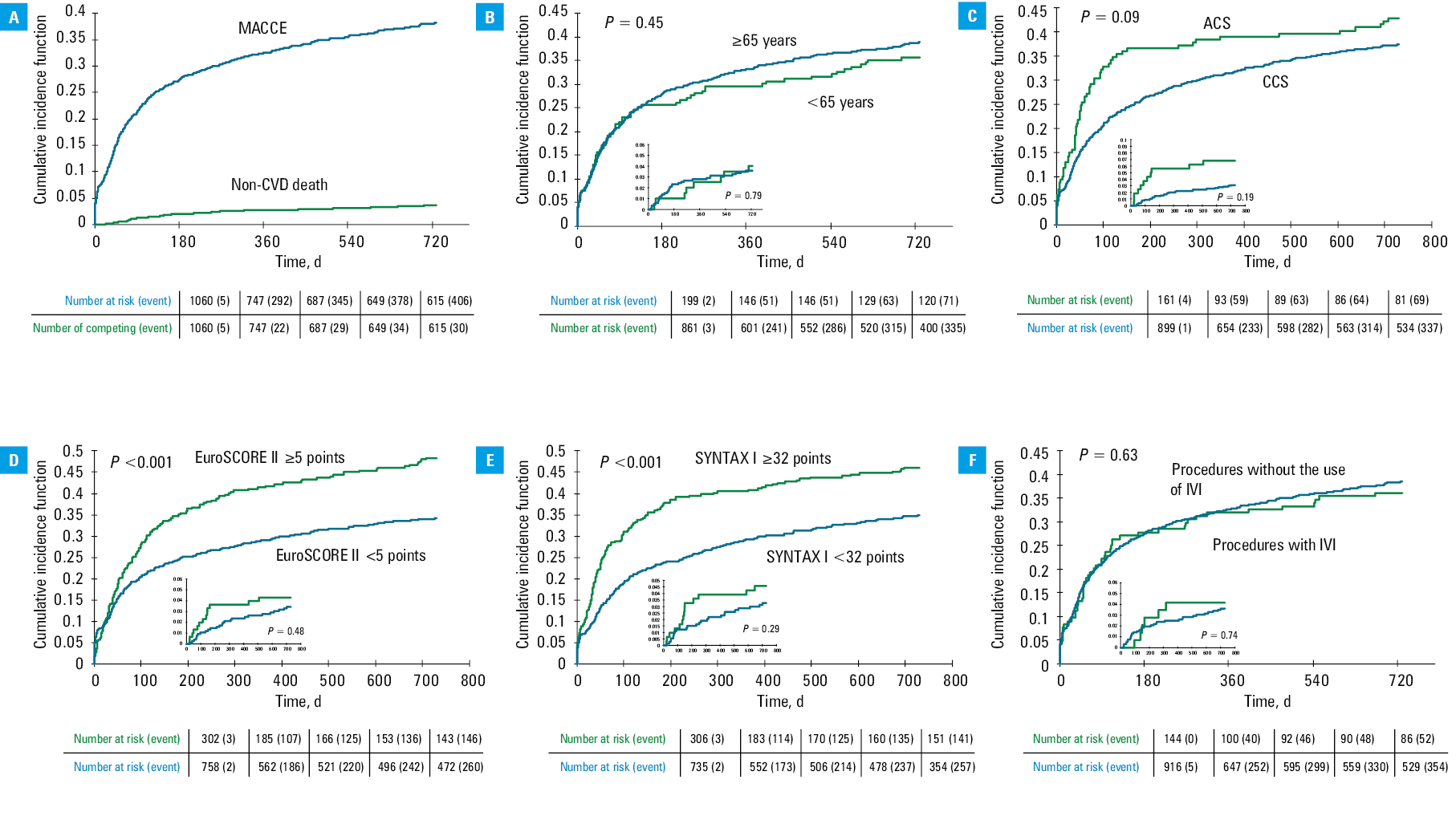
In competing‑risk cumulative incidence analyses, the patients with EuroSCORE II of 5 and above and SYNTAX I score of 32 or above had a significantly higher risk of MACCE (both P <0.001), whereas age (P = 0.45), clinical presentation (ACS vs CCS; P = 0.09), and the use of IVI (IVUS/OCT; P = 0.63) were not significantly associated with the risk; the cumulative incidence of noncardiovascular death remained low in relation to MACCE (Table 4, Figure 4).
Parameter | Entire cohort | EuroSCORE II <5 (n = 758) | EuroSCORE II ≥5 (n = 302) | P value | SYNTAX I <32 (n = 735) | SYNTAX I ≥32 (n = 306) | P value |
Data are presented as number (percentage).
Abbreviations: see Figure 1 | |||||||
30 days of follow‑up | |||||||
MACCE | 116 (10.9) | 81 (10.7) | 35 (11.6) | 0.67 | 68 (9.3) | 45 (14.7) | 0.01 |
CVD death | 22 (2.1) | 9 (1.2) | 13 (4.3) | 0.001 | 10 (1.4) | 10 (3.3) | 0.04 |
MI | 87 (8.2) | 69 (9.1) | 18 (5.9) | 0.09 | 54 (7.2) | 31 (10.1) | 0.14 |
Ischemic stroke / TIA | 5 (0.5) | 2 (0.3) | 3 (1) | 0.12 | 4 (0.5) | 1 (0.3) | 0.64 |
TVR | 9 (0.8) | 5 (0.7) | 4 (1.3) | 0.28 | 4 (0.5) | 5 (1.6) | 0.08 |
All‑cause death | 28 (2.6) | 11 (1.4) | 17 (5.6) | <0.001 | 13 (1.8) | 13 (4.2) | 0.02 |
Major bleeding | 12 (1.1) | 6 (0.8) | 6 (2) | 0.1 | 6 (0.8) | 5 (1.6) | 0.24 |
AKI | 43 (4.1) | 16 (2.1) | 27 (8.9) | <0.001 | 25 (3.4) | 17 (5.6) | 0.11 |
2 years of follow‑up | |||||||
MACCE | 406 (38.3) | 260 (34.3) | 146 (48.3) | <0.001 | 257 (35) | 141 (46.1) | <0.001 |
CVD death | 150 (14.1) | 65 (8.6) | 85 (28.1) | <0.001 | 90 (12.2) | 55 (18) | 0.02 |
MI | 187 (17.6) | 141 (18.6) | 46 (15.2) | 0.19 | 113 (15.4) | 70 (22.9) | 0.004 |
Ischemic stroke / TIA | 23 (2.2) | 15 (2) | 8 (2.6) | 0.49 | 9 (1.2) | 12 (3.9) | 0.005 |
TVR | 145 (13.7) | 99 (13.1) | 46 (15.2) | 0.35 | 104 (14.1) | 37 (12.1) | 0.38 |
All‑cause death | 206 (19.4) | 100 (13.2) | 106 (35.1) | <0.001 | 124 (16.9) | 76 (24.8) | 0.003 |
Major bleeding | 34 (3.2) | 21 (2.8) | 13 (4.3) | 0.2 | 20 (2.7) | 13 (4.2) | 0.2 |
AKI | 79 (7.4) | 43 (5.7) | 36 (11.9) | <0.001 | 52 (7.1) | 26 (8.5) | 0.47 |
Discussion
Our study represents the largest Polish, comprehensive investigation of RA for heavily calcified coronary lesions, providing immediate, short- and long‑term follow‑up data. It is a retrospective, single‑center registry spanning 15 years of clinical practice. Over this period, patient selection criteria evolved, and the therapeutic options for managing severe coronary calcification expanded substantially. The results demonstrate high technical and clinical success rates despite the increasing complexity of treated patients and lesions. Consistent with prior reports, long‑term clinical outcomes were largely determined by the high‑risk clinical profile and angiographic severity of this population.
Role of rotational atherectomy
In 2024, approximately 2500 RA procedures were performed in Poland and around 40 000 across Europe (data courtesy of Boston Scientific). When combined with the increasing use of intravascular lithotripsy and orbital atherectomy, these Figures highlight the widespread yet still insufficient adoption of calcium‑modifying techniques, reflecting the unmet clinical need in this field. Importantly, the growing demand for these methods has been driven predominantly by real‑world practice rather than robust scientific evidence. The use of calcium‑modifying techniques should be considered as part of a comprehensive and individualized decision‑making process that takes into account all available options. This approach is supported by recent expert consensus,21 which emphasizes the importance of stenosis morphology, calcification distribution, and safety profiles of individual devices. RA remains central in the management of uncrossable lesions, while nodular calcification is more appropriately approached with a multidevice strategy. To date, only 2 randomized controlled trials, including just over 200 patients, have specifically evaluated RA. These studies demonstrated comparable acute lumen gain and stent expansion between RA and balloon‑based lesion preparation, with no excess late lumen loss at 9 months.11,12 Similarly, rates of target vessel failure and MACCE at 2 years did not differ significantly between the strategies.18 At 5 years, outcomes remained broadly similar, although a significant reduction in TLR was observed in the RA arm.19 Additional insights come from secondary analyses of these trials, particularly in the patients who crossed over from the balloon arm to the RA one. These individuals typically presented with tighter, longer, and more tortuous stenoses, frequently located at bifurcation sites—precisely the subset of lesions in which RA continues to be considered indispensable.20 Notably, registry data, arguably more reflective of real‑world practice, show that such complex lesions constitute the majority of cases in which RA is applied.
Role of intravascular imaging
Currently, the qualification and choice of strategy for the treatment of severe coronary calcification rely predominantly on IVI.21 IVI provides detailed information on calcium burden and distribution, enabling operators to determine the need for calcium modification devices. Achieving controlled fractures within calcified plaques facilitates optimal stent expansion, thereby improving both early and long‑term outcomes.22 Although its use increased substantially during the latter half of the study period, IVI remained infrequent in our registry, representing an important limitation of the analysis. In contrast, in our current clinical practice, IVI is performed in approximately 80% of the RA procedures, reflecting the contemporary shift toward imaging‑guided PCI. Nevertheless, angiography itself demonstrates very high specificity (98.7%), and may be sufficiently sensitive to detect clinically relevant calcification requiring plaque modification.23 Furthermore, in up to 60% of lesions, the IVI catheter cannot initially cross the target segment, which may unnecessarily increase the number of manipulations within the vessel.7 On the other hand, current evidence consistently supports the superiority of IVI over angiography for guiding PCI in patients with CAD. This appears particularly relevant in the setting of severe coronary calcification, where multiple studies have demonstrated higher rates of stent underexpansion, malapposition, target vessel failure, stent thrombosis, mortality, and MACCE.4,24,25 However, data specifically addressing severe coronary calcification remain inconclusive.12,26
Temporal trends and clinical implications
Over the years, the RA procedure itself has undergone little change from a technical standpoint, both in our data and in previously published registries. The instrumentation—specifically the burr as the modifying element—has remained essentially unchanged since the introduction of the method. Standardized practice has consistently emphasized a cautious and deliberate technique, including the use of nitroglycerin in the flush solution, careful burr advancement, the preferred “pecking” motion, limited ablation runs of 15–20 seconds, and maintaining burr speeds between 140 000 and 180 000 rpm. This well‑established strategy effectively minimizes complications, which explains why the rates of immediate adverse events in our registry were comparable to those reported in other large‑scale registries.8-10 This applies particularly to complications such as flow disturbances, perforation, tamponade, and stroke. The incidence of dissection and PMI was also comparable; however, comparisons are more difficult in the latter case due to variability in diagnostic definitions.
The observed increase in adverse events and reduction in clinical success over time should be interpreted in the context of a progressively higher‑risk patient population. Compared with previously published studies, the patients in our registry presented with greater clinical and angiographic complexity. In particular, the prevalence of comorbidities strongly associated with adverse prognosis—such as CKD, diabetes mellitus, reduced left ventricular ejection fraction, prior acute coronary syndromes, and previous PCI—was clearly high. With advances in PCI techniques and adjunctive devices, RA has increasingly been reserved for the most complex subsets, including LM, multivessel, and bifurcation lesions with heavy calcification.
Chronic kidney disease and outcomes after rotational atherectomy
In our registry, renal dysfunction emerged as one of the strongest predictors of periprocedural complications and adverse long‑term outcomes. This finding is consistent with prior evidence showing that CKD confers a markedly elevated risk of CAD, while also complicating invasive treatment due to multiple comorbidities and the heightened susceptibility to procedural complications and contrast‑induced nephropathy. Despite the clinical relevance, there is a striking paucity of dedicated trials addressing the management of CAD in patients with advanced CKD. Optimal treatment strategies in this population, therefore, remain uncertain and are largely guided by low‑quality evidence.
The ISCHEMIA‑CKD trial27 provided the most robust data to date, demonstrating that an initial invasive strategy was associated with higher rates of PMI, which in turn translated into an increased risk of subsequent death. At 3 years, the composite outcome of all‑cause death or nonfatal MI did not differ between invasive and conservative strategies (HR, 1.01; 95% CI, 0.79–1.29). Similarly, there was no improvement in the secondary composite outcome of death, nonfatal MI, or hospitalization for unstable angina, heart failure, or resuscitated cardiac arrest (HR, 1.02; 95% CI, 0.79–1.29). Of note, the invasive strategy was associated with a nearly 4‑fold higher risk of stroke (HR, 3.76; 95% CI, 1.52–9.52), with most events occurring several months or years after the index procedure.27
These data underscore the unmet need for prospective studies focusing on patients with advanced CKD undergoing PCI, particularly with adjunctive calcium‑modifying techniques such as RA. As a next step, we plan to perform a dedicated analysis of RA‑treated patients with impaired renal function within our registry, aiming to provide novel insights into this high‑risk population.
Strengths and limitations
The main strength of this analysis is the large, consecutive, real‑world cohort with long‑term follow‑up, reflecting daily clinical practice in a high‑volume center. However, the retrospective single‑center design and lack of systematic IVI limit the generalizability of the findings. No pre- or postprocedural systematic quantitative coronary angiography analysis was performed. In addition, evolving definitions of MI and changes in clinical practice over 15 years introduce heterogeneity that must be considered when interpreting outcomes.
Conclusions
RA remains a cornerstone technique for the treatment of heavily calcified coronary lesions, ensuring high procedural success even in the most complex patient subsets. Our study highlights temporal shifts in patient selection and procedural practice in Poland and reinforces the indispensable role of RA in contemporary PCI.
- Copeland‑Halperin RS, Baber U, Aquino M, et al. Prevalence, correlates, and impact of coronary calcification on adverse events following PCI with newer‑generation DES: findings from a large multiethnic registry. Catheter Cardiovasc Interv. 2018; 91: 859‑866. | Crossref
- Arad Y, Goodman KJ, Roth M, et al. Coronary calcification, coronary disease risk factors, C‑reactive protein, and atherosclerotic cardiovascular disease events: the St. Francis Heart Study. J Am Coll Cardiol. 2005; 46: 158‑165. | Crossref
- Mori H, Torii S, Kutyna M, et al. Coronary artery calcification and its progression: what does it really mean? JACC Cardiovasc Imaging. 2018; 11: 127‑142. | Crossref
- Guedeney P, Claessen BE, Mehran R, et al. Coronary calcification and long‑term outcomes according to drug‑eluting stent generation. JACC Cardiovasc Interv. 2020; 13: 1417‑1428. | Crossref
- Kobayashi Y, Okura H, Kume T, et al. Impact of target lesion coronary calcification on stent expansion. Circ J. 2014; 78: 2209‑2214. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION