Acute kidney injury in the course of tubulointerstitial nephritis related to direct oral anticoagulants

 CC BY 4.0
CC BY 4.0
Acute kidney injury in the course of tubulointerstitial nephritis related to direct oral anticoagulants
Acute interstitial nephritis (AIN) is an inflammatory kidney disorder involving interstitial edema and leukocyte infiltration. This condition can lead to impaired renal function. Medications are among the most common causes of AIN, and, in rare cases, direct oral anticoagulants (DOACs) have been reported to trigger the condition.1-4
A 52‑year‑old man with hypertension, class II obesity, chronic obstructive pulmonary disease, and heart failure with preserved ejection fraction was admitted to a hospital with nephritic syndrome, hematochezia, and hemoptysis. He had no known allergies and had undergone prior pulmonary vein ostial cryoablation for paroxysmal atrial fibrillation. He had been on dabigatran for stroke prevention for 25 months. He had no fever or rash but had upper‑limb and truncal petechiae, which were attributed to dabigatran overexposure. Laboratory workup showed acute kidney injury (AKI) with elevated levels of serum creatinine (1810 µmol/l; reference range [RR], 44–124 µmol/l) and urea (41.9 mmol/l; RR, 2.76–8.07 mmol/l). The patient had normocytic anemia (hemoglobin, 11 g/dl; RR, 14–18 g/dl), mild thrombocytopenia, normal liver function parameters, a normal leukocyte count with eosinophilia, and markedly prolonged coagulation times: international normalized ratio of 1.65 (RR, 0.9–1.2) and activated partial thromboplastin time of 107.6 seconds (RR, 26–36 s). Urinalysis showed leukocyturia, hematuria, and proteinuria (proteins, 0.69 g/24 h; RR <0.15 g/24 h); eosinophiluria was not assessed. C‑reactive protein level was elevated at 113 mg/l (RR <5 mg/l). No inflammatory or infectious cause was identified. Gastroscopy showed no source of bleeding. Abdominal ultrasonography identified hepatomegaly with hepatic steatosis, as well as normal‑appearing kidneys without obstruction or stones, except for a 35‑mm left renal cortical cyst. Due to a strong indication of renal failure, renal replacement therapy (RRT) was initiated. Immunological testing was negative for antineutrophil cytoplasmic antibodies, antinuclear antibodies, and monoclonal proteins. Kidney biopsy demonstrated chronic interstitial lesions with mild active inflammation, and AIN was diagnosed (Figure 1A and 1B). Dabigatran was discontinued and low‑molecular‑weight heparin (LMWH) was introduced temporarily. Upon reviewing the patient’s history and recent modifications to long‑term therapy, dabigatran (150 mg twice daily) was identified as the newly introduced medication. Steroid treatment was included as therapy for AIN. The patient’s renal function gradually improved, and RRT was discontinued after 3 sessions. To enhance the nephroprotective therapy, an angiotensin II receptor blocker and a sodium‑glucose cotransporter 2 inhibitor were added. Steroid treatment was completed after 2 months of therapy. Subsequently, apixaban (5 mg twice daily) was initiated.
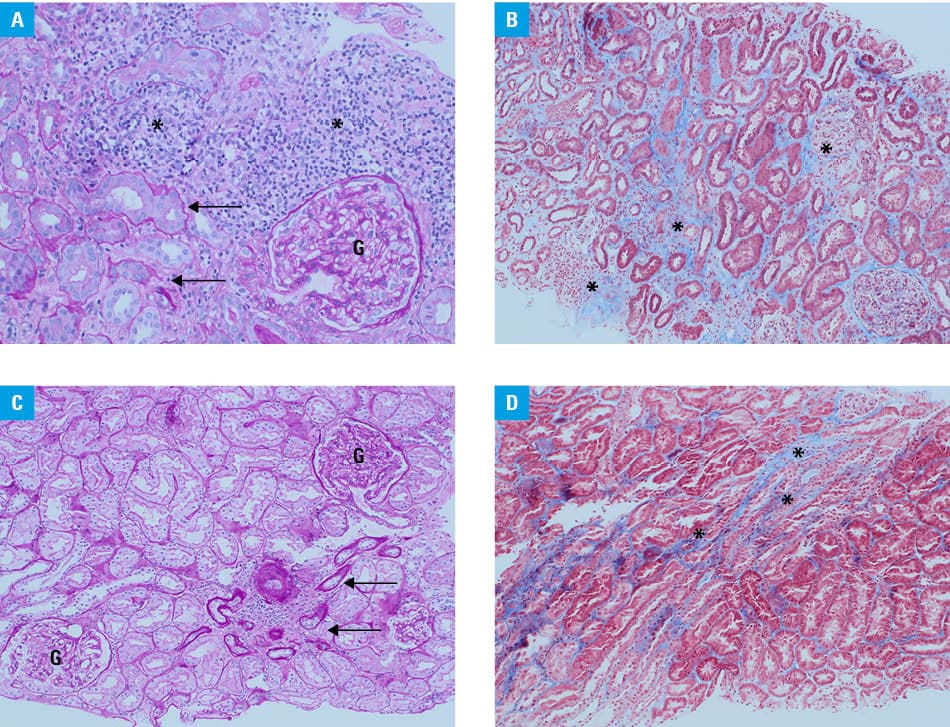
Four months later, the patient was readmitted due to persistent proteinuria, mild anemia, thrombocytopenia, and increased serum creatinine, indicating AKI. Repeat kidney biopsy showed findings comparable to those of the initial biopsy (Figure 1C and 1D). Due to the suspected association between DOACs and AIN, apixaban was discontinued and replaced with LMWH (enoxaparin, 60 mg daily). Steroid treatment was resumed according to the recommendations for the treatment of AIN. After 1 month of therapy, the urinalysis was normal. The patient was tapered off steroids after 2 months, and has remained in remission since then.
This case highlights the potential association between NOACs and AIN, involving dabigatran and apixaban. As these agents become more widely used, close monitoring of renal function is essential. Early recognition of AIN, prompt discontinuation of the offending agent, and steroid therapy may prevent irreversible kidney injury.1,5
- Abdulhadi B, Mulki R, Goyal A, Rangaswami J. Novel oral anticoagulant and kidney injury: apixban‑related acute interstitial nephritis. BMJ Case Rep. 2017: bcr2017221641. | Crossref
- Deng ZL, Yang WL, Zhao XY, et al. Simultaneous subacute interstitial nephritis and anticoagulant‑related nephropathy related to novel oral anticoagulants use. Ren Fail. 2022; 44: 30‑33. | Crossref
- Kodner CM, Kurdimoti A. Diagnosis and management of acute interstitial nephritis. Am Fam Physician. 2003; 67: 2527‑2534. | Crossref
- Iwafuchi Y, Ito Y, Imai N, et al. Dabigatran‑related nephropathy complicated by tubulointerstinal nephritis in a patient with a normal renal function and undiagnosed IgA nephropathy. Clin Exp Nephrol. 2024; 28: 1615‑1621. | Crossref
- Patel S, Hossain MA, Ajam F, et al. Dabigatran‑induced acute interstitial nephritis: an important complication of newer oral anticoagulation agents. Case Reh Nephrol. 2018; 10: 791‑794. | Crossref
ARTICLE INFORMATION