Drug-induced hyponatremia associated with sodium-glucose cotransporter 2 inhibitors, immune checkpoint inhibitors, and targeted anticancer agents
Key words: adrenal insufficiency, hyponatremia, immune checkpoint inhibitors, sodium-glucose cotransporter 2 inhibitors, syndrome of inappropriate antidiuresis

 CC BY 4.0
CC BY 4.0
Drug-induced hyponatremia associated with sodium-glucose cotransporter 2 inhibitors, immune checkpoint inhibitors, and targeted anticancer agents
Hyponatremia is the most common electrolyte disorder and a frequent trigger for urgent assessment in internal medicine. Beyond classic culprits, such as thiazide diuretics and antidepressants, clinicians increasingly face hyponatremia in the setting of modern metabolic and oncologic therapies. Sodium‑glucose cotransporter 2 inhibitors (notably empagliflozin and dapagliflozin) promote glucosuria‑driven osmotic diuresis and electrolyte‑free water clearance, and (based on emerging evidence) may mitigate dilutional hyponatremia in selected patients with the syndrome of inappropriate antidiuresis. At the same time, glucosuria can confound urine indices, and the diuretic effect may unmask occult hypovolemia. Immune checkpoint inhibitors (eg, nivolumab, pembrolizumab, ipilimumab) may cause hyponatremia through immune‑related endocrinopathies (secondary or primary adrenal insufficiency, thyroid dysfunction) and through nonendocrine toxicities leading to salt and water losses. In a large real‑world cohort of patients receiving immune checkpoint inhibitors, hyponatremia occurred in roughly two‑thirds, and severe hyponatremia (serum sodium <124 mmol/l) in 6%; endocrine causes accounted for a small but pivotal fraction. Targeted anticancer agents (eg, vascular endothelial growth factor receptor–directed multikinase tyrosine kinase inhibitors and mammalian target of rapamycin inhibitors) add further complexity, often via gastrointestinal toxicity, renal tubular dysfunction, or inappropriate antidiuresis. We provide a bedside diagnostic algorithm and pragmatic monitoring recommendations aimed at preventing neurological harm from overly rapid correction. This narrative review summarizes contemporary mechanisms of drug‑related hyponatremia, highlights therapy‑specific diagnostic pitfalls, and proposes a practical framework for prevention, monitoring, and treatment that prioritizes neurological safety and avoidance of overcorrection.
Introduction
Hyponatremia (serum sodium level <135 mmol/l) is common in both inpatient and outpatient care and remains a frequent trigger for internal medicine consultation. In hospital cohorts, admission hyponatremia is consistently associated with excess mortality; in a study of 98 411 inpatients, it conferred a 47% higher odds of in‑hospital death (adjusted odds ratio [OR], 1.47; 95% CI, 1.33–1.62), with increased risk evident even in mild hyponatremia (130–134 mmol/l; OR, 1.37; 95% CI, 1.23–1.52).1 Across broader clinical settings, a meta‑analysis of 81 studies similarly demonstrated higher mortality among hyponatremic patients (relative risk [RR], 2.6; 95% CI, 2.31–2.93).2 Although severe acute hyponatremia can cause life‑threatening cerebral edema and seizures, chronic mild‑to‑moderate hyponatremia is not benign and has been associated with gait instability, attention deficits, falls, and fractures, particularly in older adults.3,4 For pragmatic communication, biochemical severity is often classified as mild (130–134 mmol/l), moderate (125–129 mmol/l), and profound (<125 mmol/l). Importantly, treatment urgency is determined primarily by symptom severity and the estimated acuity of onset rather than by the sodium concentration alone. In this review, we use the term “severe symptomatic hyponatremia” to denote hyponatremia with seizures, coma, or cardiorespiratory compromise requiring immediate hypertonic therapy.
Conceptually, hyponatremia is primarily a disorder of water balance rather than a true deficit of total body sodium. Serum sodium reflects the relationship between total body solute and total body water; therefore, diagnosis and management should focus on factors that limit renal electrolyte‑free water excretion, most commonly arginine vasopressin (AVP)-mediated water retention, as well as on determinants of water intake (thirst and access).5-7
Drug‑associated hyponatremia is often under‑recognized, because it develops in the context of multimorbidity and polypharmacy, and because “medication effect” can mimic common clinical phenotypes. Medications may lead to hyponatremia through several distinct pathways, including the syndrome of inappropriate antidiuresis (SIAD), renal salt wasting, hypovolemia with nonosmotic AVP release, and endocrine dysfunction.8
In recent years, modern therapies have introduced new mechanisms and crucial new diagnostic pitfalls. Sodium‑glucose cotransporter 2 inhibitors (SGLT2is) may confound urine indices through glucosuria‑driven osmotic diuresis and changes in volume status, yet emerging evidence suggests they may also be used as off‑label adjunctive therapy in selected patients with SIAD.9-11 Immune checkpoint inhibitors (ICIs) increase the likelihood of endocrine causes of “SIAD‑like” hyponatremia, especially adrenal insufficiency and hypophysitis, where delayed recognition can be fatal.12 Targeted anticancer agents and chemotherapy add further heterogeneity, commonly via gastrointestinal toxicity, renal tubular injury, and multifactorial inpatient illness.13,14 Key mechanisms and modern therapy–specific diagnostic pitfalls are summarized in Table 1. For bedside completeness, other commonly implicated medications (stratified by strength of association and typical clinical phenotype) are summarized in Supplementary material, Table S1 (eg, thiazide / thiazide‑like diuretics, selective serotonin reuptake inhibitors / serotonin‑norepinephrine reuptake inhibitors, antiepileptic drugs such as carbamazepine / oxcarbazepine, and desmopressin / vasopressin analogues). In contrast to classic drug‑focused reviews, we center this article on practical diagnostic traps that now drive real‑world errors: urine indices distorted by SGLT2i‑related glucosuria and “SIAD‑like” biochemical patterns in ICI‑treated patients, in whom adrenal insufficiency must be ruled out urgently. We therefore adopt a phenotype‑based approach, integrate drug timing into interpretation of urine osmolality (Uosm) / urine sodium concentration (UNa), and provide a ward‑ready algorithm with monitoring guidance to support safe correction.
Therapeutic agents (examples) | Predominant mechanism(s) | Typical context / timing | Key clinical clues and pitfalls | Practical prevention / monitoring |
Abbreviations: ↑, increase; ACTH, adrenocorticotropic hormone; AKI, acute kidney injury; AVP, arginine vasopressin; CTLA‑4, cytotoxic T‑lymphocyte–associated protein 4; GI, gastrointestinal; PD‑1, programmed cell death 1; PD‑L1, programmed death‑ligand 1; SIAD, syndrome of inappropriate antidiuresis; SGLT2, sodium‑glucose cotransporter 2; T4, thyroxine; TSH, thyroid‑stimulating hormone | ||||
SGLT2 inhibitors (empagliflozin, dapagliflozin) | ↑ Glucosuria resulting in osmotic diuresis; ↑ electrolyte‑free water clearance; may raise serum sodium in SIAD (off‑label, emerging evidence); may also unmask hypovolemia |
|
|
|
ICIs (anti–PD‑1/PD‑L1, anti–CTLA‑4) | Immune‑related endocrinopathies (secondary / primary adrenal insufficiency, thyroid dysfunction); GI losses; nephritis; multifactorial; sometimes paraneoplastic SIAD | Weeks to months after start, may be delayed and can occur after discontinuation |
|
|
Targeted anticancer agents and chemotherapy (various) | GI toxicity (vomiting / diarrhea), poor intake; renal tubular dysfunction / salt wasting; AKI; drug‑induced SIAD; complex multimorbidity |
|
|
|
The aim of this review is to provide a practical, clinically actionable framework for hyponatremia associated with modern therapies by 1) linking drug classes to pathophysiological mechanisms, 2) outlining a stepwise diagnostic approach that highlights drug‑specific diagnostic pitfalls, and 3) summarizing treatment and prevention strategies that prioritize neurological safety and avoidance of overly rapid correction and osmotic demyelination.15-17
Methods
This article is a pragmatic narrative review focused on drug‑associated hyponatremia in the era of modern therapies. To identify relevant evidence, we performed targeted literature searches in PubMed / MEDLINE, Embase, and the Cochrane Library from January 2000 through January 15, 2026. The full database search strategies are provided in Supplementary material, Table S2. Search terms were combined using Boolean operators and included (with synonyms and controlled vocabulary where applicable): hyponatremia / hypernatremia, drug‑induced, SIAD/ SIADH or inappropriate antidiuresis, arginine vasopressin, adrenal insufficiency or hypophysitis, immune checkpoint inhibitor (including specific agents), SGLT2i (including specific agents), targeted therapy, tyrosine kinase inhibitor, mTOR inhibitor, CDK4/6 inhibitor, CAR‑T, and chemotherapy. Reference lists of key clinical practice guidelines, systematic reviews / meta‑analyses, and high‑impact clinical studies were additionally hand‑searched to capture relevant publications not retrieved in database searches.
We prioritized clinical practice guidelines, systematic reviews / meta‑analyses, and randomized controlled trials when available; otherwise, we included observational studies, pharmacovigilance reports, and well‑documented case series. Single case reports and small case series were used selectively to illustrate rare mechanisms or newly recognized associations, and were interpreted as low‑certainty evidence. We focused on studies involving human participants and clinically relevant outcomes; preclinical‑only reports were not used to support clinical recommendations. Evidence was synthesized narratively and organized around clinically meaningful diagnostic phenotypes (eg, inappropriate antidiuresis, renal salt wasting, hypovolemia with nonosmotic AVP release, and endocrine dysfunction). To minimize overinterpretation, we avoided causal claims when data were limited, clearly separated established evidence from emerging signals, and highlighted areas of uncertainty and research gaps.
Conceptual framework for drug‑related hyponatremia
Effective plasma osmolality (tonicity) is tightly regulated by thirst, renal water handling, and AVP secretion. Osmoreceptors and neural circuits generate both homeostatic and anticipatory responses that shape water intake and thus serum sodium level.6,7,18 In healthy individuals, suppression of AVP allows for excretion of large volumes of dilute urine; sustained hyponatremia therefore almost always implies either 1) impaired free water excretion or 2) excessive water intake, or 3) both.9
Drug‑related hyponatremia can be organized along 4 practical axes: 1) nonhypotonic hyponatremia (hyperglycemia or pseudohyponatremia); 2) hypovolemic hypotonic hyponatremia (true salt and water losses with nonosmotic AVP release); 3) hypervolemic hyponatremia (low effective arterial blood volume due to heart failure, cirrhosis, nephrotic syndrome); and 4) euvolemic hypotonic hyponatremia, most commonly SIAD but also adrenal insufficiency and (rarely) severe hypothyroidism.5,15,19
SIAD is characterized by inappropriately concentrated urine and natriuresis in the absence of hypovolemia, adrenal insufficiency, or hypothyroidism.15,20 In practice, the “classic” SIAD pattern—hypotonic hyponatremia with Uosm above 100 mOsm/kg and UNa above 30 mmol/l—should be treated as a syndrome rather than a final diagnosis, because several modern drug–related states mimic SIAD biochemically.
Modern therapies create 2 recurring pitfalls. First, they may change urine indices without directly changing AVP biology. For example, glucosuria induced by SGLT2is increases Uosm independently of AVP, potentially masking an otherwise dilute urine pattern. Second, they increase the pretest probability of endocrine etiologies. In patients receiving ICIs, secondary adrenal insufficiency can present with euvolemic hypotonic hyponatremia and urine findings indistinguishable from SIAD; however, management differs fundamentally, and urgent glucocorticoid replacement may be lifesaving.12,21
Finally, oncology patients represent a high‑risk group where hyponatremia is often multifactorial. Underlying malignancy (including paraneoplastic SIAD), chemotherapy‑associated toxicity, infections, antiemetic and analgesic comedications, and treatment‑related endocrine dysfunction frequently overlap.13,14 A pragmatic approach that repeatedly reassesses volume status, treatment timing, and evolving laboratory patterns is therefore essential.
Sodium‑glucose cotransporter 2 inhibitors: from confounder to potential therapy
SGLT2is reduce renal glucose reabsorption in the proximal tubule, producing glucosuria and osmotic diuresis. By increasing urinary water excretion, they can increase electrolyte‑free water clearance and thereby raise serum sodium level in selected patients with dilutional hyponatremia.6,10,11 This profile has led to interest in SGLT2is as “aquaretic‑like” agents, albeit via a different mechanism than vasopressin receptor antagonists.
In a double‑blind randomized trial of hospitalized patients with SIAD‑induced hyponatremia, empagliflozin added to fluid restriction increased plasma sodium level more than placebo over 4 days.10 A subsequent randomized, double‑blind, placebo‑controlled crossover trial in chronic SIAD demonstrated that empagliflozin improved serum sodium level over 4 weeks, and was associated with improvements in patient‑relevant end points.11 Although the available trials are modest in size, they provide proof‑of‑concept that an SGLT2is can correct hyponatremia in SIAD.
In guidelines and practice, the first‑line therapy for chronic SIAD is fluid restriction; second‑line options include increasing solute intake (eg, oral urea), loop diuretics with salt supplementation, and vasopressin receptor antagonists, such as tolvaptan.8,15,22,23 An SGLT2is may be considered as an adjunct in selected chronic SIAD scenarios, when fluid restriction is ineffective or poorly tolerated, particularly when urea is unavailable or unacceptable and when tolvaptan is constrained by cost, access, or the need for close monitoring.
Evidence for SGLT2i efficacy in SIAD is based on a limited number of studies (including a short‑term randomized trial), and remains insufficient to position them as the first‑line therapy. In practice, their use is best restricted to stable, nonacute euvolemic SIAD as an off‑label adjunct, with structured monitoring and clear stopping rules if sodium level fails to improve or if volume depletion occurs. Evidence to date pertains mainly to empagliflozin 25 mg daily; the use for hyponatremia remains off‑label and should be individualized.10,11 Candidates should have stable hemodynamics, no severe acute symptoms, and an SIAD phenotype that has been reasonably established (including exclusion of adrenal insufficiency and hypothyroidism). Clinicians should consider renal function, frailty, concomitant diuretics, and the risk of dehydration. A pragmatic strategy is to initiate therapy under conditions where sodium level and volume status can be monitored closely and to reassess serum sodium level within several days to 1–2 weeks, depending on baseline severity.24
Glucosuria and urine osmolality
Glucosuria can increase urine osmolality independent of AVP. Therefore, in patients taking SGLT2is, a single Uosm value may be less informative for classifying hypotonic hyponatremia. Whenever urine indices appear discordant with the clinical picture, repeat measurements after stabilization of volume status or temporary discontinuation of the SGLT2is may help clarify the phenotype.19
The osmotic diuretic effect can unmask or worsen hypovolemia, particularly when combined with loop diuretics or during intercurrent illness. Hypovolemia itself can trigger nonosmotic AVP release and thus aggravate hyponatremia. In any hyponatremic patient receiving an SGLT2i, clinicians should actively assess for dehydration, hypotension, and acute kidney injury (AKI), and apply sick‑day guidance (temporary discontinuation during acute illness or reduced intake).
Immune checkpoint inhibitors: when “syndrome of inappropriate antidiuresis–like” hyponatremia may be adrenal failure
ICIs are increasingly used across cancer types and are associated with a broad spectrum of immune‑related adverse events. Hyponatremia is common among ICI‑treated patients, and is often multifactorial.13,25 The clinical challenge is to promptly identify endocrine causes, especially adrenal insufficiency, because treatment is urgent and differs fundamentally from standard SIAD management.
In a real‑world cohort including 2458 patients treated with ICIs, hyponatremia occurred in 62% and severe hyponatremia (serum sodium level <124 mmol/l) in 6% within the first year. Median time to severe hyponatremia was approximately 5–6 months. Endocrine causes accounted for only a minority of severe cases, but represent a high‑risk diagnosis given the risk of adrenal crisis.25 These estimates come from a retrospective real‑world cohort and reflect hyponatremia occurring during ICI exposure, not necessarily ICI‑caused events. Hyponatremia was defined biochemically by serum sodium level below the prespecified cutoff(s), and the observed rates are likely influenced by comorbid illnesses, concomitant medications, and intercurrent complications in oncology patients.
ICIs can trigger hypophysitis with secondary adrenal insufficiency, primary adrenalitis leading to primary adrenal insufficiency, and thyroid dysfunction (often destructive thyroiditis). Adrenal insufficiency contributes to hyponatremia through a loss of cortisol‑mediated suppression of AVP; in primary adrenal insufficiency, concomitant mineralocorticoid deficiency leads to renal salt wasting and often hyperkalemia.12,21,26
Nonendocrine mechanisms and confounding factors
Hyponatremia can also result from ICI‑related colitis (salt and water loss), nausea and poor intake, sepsis, kidney injury, and comedications (eg, opioids, antiemetics). Paraneoplastic SIAD remains an important alternative explanation, particularly in small‑cell lung cancer and other malignancies traditionally associated with SIAD.13,14
A practical endocrine rule‑out strategy in acute hyponatremia
In any hypotonic hyponatremia occurring in a patient on ICIs—especially when accompanied by hypotension, profound fatigue, anorexia, nausea, headache, unexplained eosinophilia, or hypoglycemia—obtain early morning serum cortisol and adrenocorticotropic hormone (ACTH) levels, and asses thyroid function (thyroid‑stimulating hormone [TSH] and free thyroxine [fT4] levels). If adrenal crisis is suspected, treat immediately with stress‑dose intravenous hydrocortisone and isotonic fluids without waiting for confirmatory results.12,21
Primary adrenal insufficiency more often features hyperkalemia, and may require mineralocorticoid replacement. Secondary adrenal insufficiency may coexist with other pituitary deficits, and often presents with headache or visual symptoms in hypophysitis. While definitive endocrine testing (eg, corticotropin stimulation) is important for long‑term management, it should not delay acute stabilization.21
An important iatrogenic pitfall is initiating levothyroxine before glucocorticoid replacement in a patient with combined adrenal insufficiency and hypothyroidism, as thyroid hormone can precipitate adrenal crisis. Therefore, when both are suspected, treat adrenal insufficiency first and then address thyroid dysfunction.12
Although uncommon, ICIs may also precipitate posterior pituitary involvement with AVP deficiency (central diabetes insipidus), typically in the context of panhypophysitis. A recent case study described AVP deficiency developing after combined nivolumab / ipilimumab therapy in a man with disseminated melanoma, underscoring the breadth of ICI‑related pituitary toxicity and the need for early endocrine involvement.27
Follow‑up and coordination
Endocrinopathies can occur weeks to months after ICI initiation and occasionally after discontinuation. Shared‑care pathways between oncology, endocrinology, and internal medicine should define baseline and periodic laboratory monitoring, patient education, and escalation routes for acute presentations.12,28-30
Targeted anticancer agents and chemotherapy: a brief mechanistic overview
Beyond ICIs, targeted anticancer agents and conventional chemotherapy can contribute to hyponatremia through several mechanisms, including nausea and reduced solute intake, diarrhea, renal tubular dysfunction (including salt wasting), kidney injury, and SIAD‑like inappropriate antidiuresis. At the bedside, it is often helpful to start by identifying the dominant phenotype (gastrointestinal loss / hypovolemia, renal tubular / salt wasting, or SIAD‑like inappropriate antidiuresis), recognizing that overlap is common in oncology inpatients.8,13 A detailed class‑by‑class overview of anticancer agents associated with hyponatremia (including proposed mechanisms and practical clinical notes) is provided in Table 2. This Table lists representative agents by class (eg, vascular endothelial growth factor receptor–directed multikinase tyrosine kinase inhibitors, mammalian target of rapamycin inhibitors, epidermal growth factor receptor / anaplastic lymphoma kinase inhibitors, cyclin‑dependent kinases 4 and 6 inhibitors, Bruton tyrosine kinase inhibitors, venetoclax, and chimeric antigen receptor T‑cell therapies) to facilitate medication review on admission.
Therapy (class and common examples) | Most likely mechanism / clinical phenotype of hyponatremia | Practical monitoring (minimum on an inpatient ward) |
a Examples are nonexhaustive. In oncology inpatients, hyponatremia is commonly multifactorial. A phenotype‑first approach is usually helpful (GI losses / hypovolemia, renal tubular salt wasting/AKI, or SIAD‑like inappropriate antidiuresis). Always review comedications and intravenous fluids, and reassess after clinical changes.
Abbreviations: ALL, acute lymphoblastic leukemia; BCL2, B‑cell lymphoma 2; BTK, Bruton tyrosine kinase; CAR‑T, chimeric antigen receptor T‑cell therapy; CDK, cyclin‑dependent kinase; CLL, chronic lymphocytic leukemia; CML, chronic myeloid leukemia; CRS, cytokine release syndrome; DLBCL, diffuse large B‑cell lymphoma; DTC, differentiated thyroid carcinoma; eGFR, estimated glomerular filtration rate; EGFR, epidermal growth factor receptor; FLT3, Fms‑related tyrosine kinase 3; HCC, hepatocellular carcinoma; ICU, intensive care unit; IV, intravenous; MCL, mast cell leukemia; mTOR, mammalian target of rapamycin; NET, neuroendocrine tumor; NSCLC, non–small‑cell lung cancer; RCC, renal cell carcinoma; SNRI, serotonin‑norepinephrine reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor; TKI, tyrosine kinase inhibitor; TLS, tumor lysis syndrome; VGEFR, vascular endothelial growth factor receptor; WM, Waldenström macroglobulinemia; others, see Table 1 | ||
Multikinase inhibitors / VEGFR‑directed TKIs: axitinib, cabozantinib, lenvatinib, pazopanib, sunitinib, sorafenib (RCC, HCC, DTC, etc.) |
|
|
mTOR inhibitors: everolimus, temsirolimus (RCC, NET, etc.) |
|
|
EGFR TKI (3rd generation): osimertinib (EGFR‑mutant NSCLC) |
|
|
ALK inhibitors (± ROS1): alectinib, ceritinib, brigatinib, lorlatinib, crizotinib |
|
|
CDK4/6 inhibitors (particularly abemaciclib; also palbociclib, ribociclib) |
|
|
BCR‑ABL TKIs (CML/ALL): imatinib, dasatinib, nilotinib, bosutinib |
|
|
Proteasome inhibitor: bortezomib (multiple myeloma, lymphoma) |
|
|
BTK inhibitors: ibrutinib, acalabrutinib (CLL, MCL, WM, etc.) |
|
|
PI3Kδ inhibitor: idelalisib (CLL, lymphoma) |
|
|
BCL‑2 inhibitor: venetoclax (CLL/AML; TLS ramp‑up and prophylaxis) |
|
|
FLT3 inhibitor: gilteritinib (FLT3‑mutated AML) |
|
|
Cellular therapies (hematology): CD19 CAR‑T (DLBCL/ALL, etc.) |
|
|
Chemotherapy‑associated toxicity and complications, such as infections, frequently coexist and may dominate the etiology of hyponatremia in oncology inpatients. In this setting, “drug‑associated” hyponatremia should not be equated with “drug‑caused” hyponatremia, as supportive medications, intravenous fluids, infections, reduced intake, and the underlying malignancy (including paraneoplastic SIAD) commonly contribute in parallel.31 Practical management therefore requires treating the patient’s evolving physiology (volume depletion, inflammation, kidney injury) in parallel with review of the oncologic regimen, supportive medications, and intravenous fluids, with repeated reassessment over time.14
Some targeted agents may also alter hemodynamics and neurohormonal signaling (including the renin‑angiotensin‑aldosterone system), which can blur bedside volume assessment and contribute to mixed phenotypes.32 For this reason, close sodium monitoring, repeated reassessment, and collaboration with oncology specialists are central to safe correction of hyponatremia in this setting.
Diagnostic approach: a stepwise strategy with modern therapy–specific pitfalls
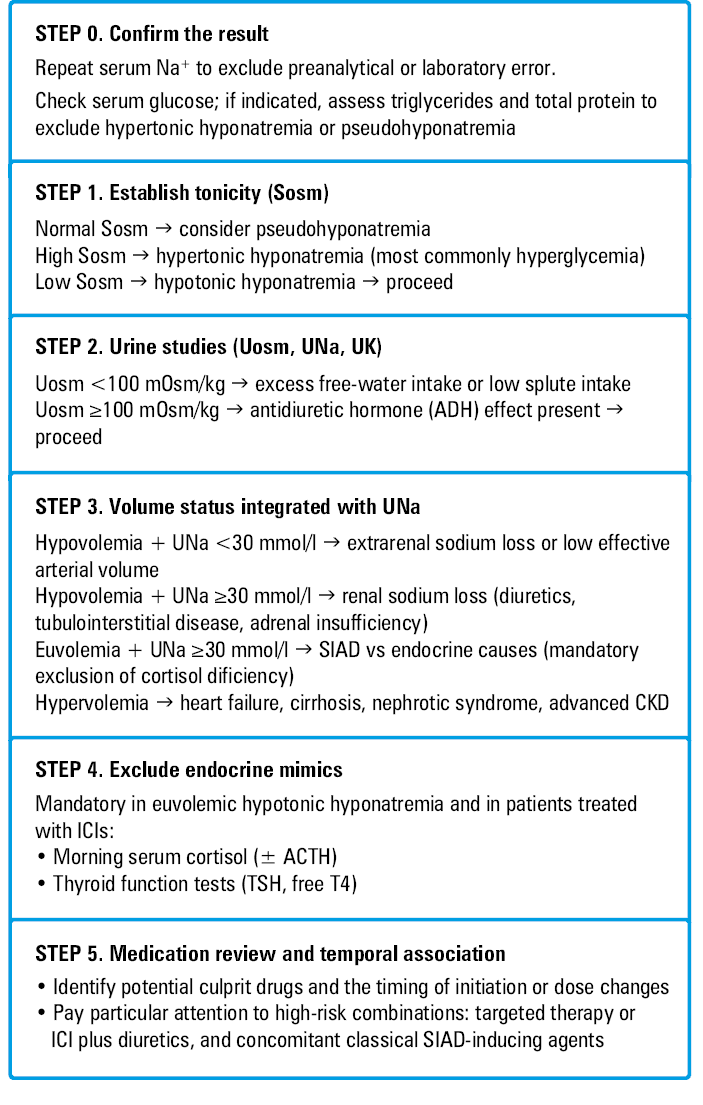
A pragmatic inpatient diagnostic flow is summarized in Figure 1. Table 3 is intentionally designed as a 1‑page bedside checklist highlighting modern therapy–specific caveats and common points of misinterpretation rather than duplicating the full algorithm. The steps below should be applied iteratively, as volume status and urine indices may change over time particularly in frail and oncology inpatients.
Abbreviations: Sosm, serum osmolality; UK, urine potassium; others, see Tables 1 and 3
Step | What to do | Notes for modern therapies |
Step 1: confirm hypotonicity and exclude artefacts | Obtain serum osmolality in all patients with hyponatremia. If serum osmolality is normal or high, exclude hypertonic (eg, hyperglycemic) hyponatremia and pseudohyponatremia (severe hyperlipidemia or hyperproteinemia) before applying SIAD treatment. | Hyperglycemia may coexist with SGLT2i therapy or immune‑mediated diabetes (ICIs). In oncology inpatients, repeat sodium / serum osmolality if results do not fit the clinical picture. |
Step 2: interpret urine studies in context | Measure Uosm and UNa, ideally before IV fluids or major diuretic changes. Use Uosm to determine whether electrolyte‑free water excretion is appropriately dilute (<100 mOsm/kg) vs impaired (≥100 mOsm/kg). Interpret UNa together with the clinical picture and recent therapies rather than as stand‑alone cutoffs. | SGLT2is can increase Uosm via glucosuria (osmotic diuresis) independent of AVP. Diuretics, recent IV fluids, CKD, and low‑solute intake commonly confound UNa/Uosm; practical pitfalls and responses are summarized in Table 4. |
Step 3: prioritize endocrine exclusion in euvolemic patterns | In euvolemic hypotonic hyponatremia with inappropriately concentrated urine and higher UNa (SIAD‑like pattern), obtain early morning serum cortisol (±ACTH) and thyroid tests (TSH, free T4) promptly. If adrenal crisis is suspected, treat immediately with stress‑dose glucocorticoids and isotonic fluids without waiting for confirmatory testing. | Mandatory in patients receiving ICIs, where delayed recognition of adrenal insufficiency / hypophysitis may be life‑threatening; use Table 5 as a bedside checklist. If both adrenal insufficiency and hypothyroidism are suspected, treat adrenal insufficiency first. |
Step 3.1: consider adjunct tests and the response to therapy (optional) | When SIAD is suspected or urine indices are confounded, consider adjunct markers (eg, low serum uric acid and high fractional excretion of urate) as supportive evidence. In selected stable inpatients, a cautious isotonic saline challenge with close sodium monitoring may help distinguish hypovolemia (sodium rises with volume repletion) from SIAD (limited rise with persistently concentrated urine). | Adjunct markers are influenced by kidney function and comorbidity and should complement (not replace) clinical judgement. Avoid saline‑challenge approaches in unstable patients or when overcorrection risk is high. |
Step 4: recognize that volume status is dynamic (iterate with Steps 2–3) | Reassess volume status frequently, recognizing that bedside assessment is imperfect (especially in older / frail patients). Integrate examination with trends in weight, orthostatic blood pressure, BUN/creatinine, and the evolving clinical course. Repeat urine studies after major physiological changes (fluids, diarrhea, sepsis, AKI), because phenotypes and indices can shift over time. | SGLT2‑induced diuresis can worsen hypovolemia; targeted therapy / chemotherapy often adds GI losses, infection and AKI, producing mixed phenotypes. Frequent reassessment is particularly important in oncology inpatients. |
Step 5: medication review and temporal association | Review all medications (including supportive drugs) and the timing of initiation / dose changes. Stop or adjust likely contributors when feasible. Treat the dominant pathophysiological phenotype and monitor sodium correction closely to avoid overcorrection; escalate / consult (endocrinology / oncology / nephrology) when uncertainty persists. Use a structured checklist of classic hyponatremia‑inducing drugs (Table 1), with particular attention to thiazide / thiazide‑like diuretics, SSRIs/SNRIs, carbamazepine / oxcarbazepine, desmopressin / vasopressin, and antipsychotics. |
|
Step 1: Confirm hypotonicity and exclude artefacts. Serum osmolality should be obtained in all patients with hyponatremia. Nonhypotonic hyponatremia due to hyperglycemia (translocational) or pseudohyponatremia due to severe hyperlipidemia or hyperproteinemia should be excluded before proceeding with SIAD algorithms.15,19 This initial triage is shown in Step 1 of the algorithm (Figure 1).
Step 2: Interpret urine studies in context. In confirmed hypotonic hyponatremia, Uosm indicates whether the kidneys are appropriately excreting electrolyte‑free water (appropriately dilute urine suggests suppressed AVP, whereas inappropriately concentrated urine suggests impaired water excretion, most commonly AVP‑mediated). UNa then helps distinguish low effective arterial blood volume states (typically lower UNa) from euvolemic patterns compatible with SIAD (typically higher UNa), but both indices must be interpreted alongside the clinical picture and recent therapies rather than as stand‑alone cutoffs. Urine indices are frequently confounded by diuretics, recent intravenous fluids, glucosuria, and osmotic diuresis in patients receiving SGLT2is, with reduced renal concentrating / diluting capacity in chronic kidney disease, and low solute intake. Common situations in which urine indices mislead and practical responses are summarized in Table 4.
Diuretics (especially thiazides; loop diuretics also confound) | |||||
Trap | UNa may be high despite low effective arterial blood volume; classic SIAD criteria become unreliable. | ||||
What to do | Check timing and dose; if clinically safe, hold the diuretic and repeat urine studies. Consider uric acid/FEUA as supportive clues, not a definitive test. | ||||
Recent intravenous fluids (ED/early admission) | |||||
Trap | UNa and Uosm can look “mixed” for several hours after isotonic orhypotonic fluids. | ||||
What to do | Do not anchor on a single urine sample; repeat after hemodynamic stabilization and interpret alongside the sodium trend and clinical course. | ||||
SGLT‑2is (glucosuria‑driven osmotic diuresis) | |||||
Trap | Uosm can be high mainly because of glucosuria, not because of AVP‑driven antidiuresis; volume status may shift with osmotic diuresis. | ||||
What to do | Look for glucosuria; interpret Uosm in context. If the pattern does not fit, repeat urine indices after stabilization (and consider temporary interruption only when clinically appropriate). | ||||
Chronic kidney disease | |||||
Trap | Impaired concentrating / diluting capacity produces “intermediate” values that do not map neatly onto classic phenotypes. | ||||
What to do | Lean more on tonicity, volume assessment, sodium trajectory, and response to therapy than on rigid cutoffs. | ||||
Low solute intake (tea‑and‑toast diet, alcoholism, malnutrition) | |||||
Trap | Urine may be very dilute, yet free‑water excretion is limited by low osmolar load; hyponatremia worsens with excess free water. | ||||
What to do | Take a dietary history; treat with solute repletion (protein / salt) plus fluid guidance, and monitor closely for overly rapid correction once intake improves. | ||||
Step 3: Prioritize endocrine exclusion in euvolemic patterns. Euvolemic hypotonic hyponatremia with inappropriately concentrated urine and an elevated UNa is compatible with SIAD, but an identical biochemical pattern can be seen in secondary adrenal insufficiency (and, less commonly, severe hypothyroidism). Therefore, serum cortisol level should be obtained early in all unexplained euvolemic hypotonic hyponatremia and is mandatory in patients receiving ICIs. In ICI‑treated patients, endocrine causes of SIAD‑like hyponatremia must be actively excluded, as delayed recognition of adrenal insufficiency may be life‑threatening. A bedside checklist for ICI‑treated patients is provided in Table 5.
When to think “adrenal crisis / hypophysitis” |
Abbreviations: see Table 1 |
|
What to draw early (if this does not delay treatment) |
|
When not to wait for results |
|
Step 3.1: Consider adjunct tests and the response to therapy. When SIAD is suspected, additional clues, such as low serum uric acid and high fractional excretion of urate may support the diagnosis and can be helpful when UNa is confounded by diuretics. However, these markers are influenced by kidney function and comorbidities, so they should complement and not replace clinical judgement. In selected stable patients, a cautious isotonic saline challenge (with close sodium monitoring) may help distinguish hypovolemia (sodium rises with volume repletion) from SIAD (limited rise and persistent urine concentration), but this approach is not appropriate in all settings.15,19,20 Clinical volume assessment should be interpreted together with urinary sodium as outlined in Step 3 (Figure 1).
Step 4: Recognize that volume status is dynamic. In older or frail patients, clinical assessment of volume status is imperfect. Trends in weight, orthostatic blood pressure, blood urea nitrogen / creatinine, and response to cautious isotonic fluid challenge may help, but must be integrated with the clinical context and evolving course. Frequent reassessment is particularly important in oncology inpatients, where diarrhea, sepsis, and nephrotoxic exposures can rapidly change volume status.14
Step 5: Medication review and temporal association. Review all medications (including supportive drugs) and the timing of initiation or dose changes. Identify and stop or adjust likely contributors when feasible, and pay particular attention to high‑risk combinations (eg, targeted therapy or ICIs plus diuretics, and concomitant classic SIAD‑inducing agents). Medication review should be repeated as the clinical course evolves, alongside close monitoring of sodium correction to avoid overcorrection.
Special considerations for sodium‑glucose cotransporter 2 inhibitors
If Uosm is unexpectedly high in a patient taking an SGLT2i, consider glucosuria as a major contributor. Repeat urine studies after stabilization of hemodynamics and / or temporary discontinuation may clarify whether AVP‑mediated antidiuresis persists. A careful history of fluid intake, vomiting, diarrhea, and concomitant diuretic therapy remains indispensable.
Special considerations for immune checkpoint inhibitors
In any ICI‑treated patient presenting with hyponatremia, clinicians should obtain endocrine testing early in the evaluation and treat suspected adrenal crisis immediately with stress‑dose steroids. If the clinical picture suggests hypophysitis (headache, visual symptoms, multiple pituitary deficits), urgent endocrine consultation and pituitary imaging may be indicated.12,29
Clinical vignettes: applying the algorithm at the bedside
The following 2 vignettes are illustrative composites based on patterns repeatedly reported in the literature and encountered in routine inpatient care. They are intended to translate the diagnostic steps (Figure 1) into practical management decisions in patients treated with modern therapies.
Vignette 1: Syndrome of inappropriate antidiuresis–like urine indices driven by an sodium‑glucose cotransporter 2 inhibitor
A 74‑year‑old man with type 2 diabetes and heart failure treated with dapagliflozin is admitted with pneumonia and reduced oral intake. Serum sodium level is 123 mmol/l with low serum osmolality (hypotonic hyponatremia). Urine indices appear SIAD‑like (Uosm, 600 mOsm/kg; UNa, 55 mmol/l), yet dipstick shows marked glycosuria. Clinically, he is mildly volume‑depleted (orthostasis, rising urea / creatinine ratio).
Bedside interpretation
In the setting of SGLT2 inhibition, glycosuria can substantially increase Uosm and distort the usual inference that a high Uosm necessarily reflects inappropriate antidiuretic hormone (ADH)-mediated water retention. Mixed phenotypes are common: osmotic diuresis and poor intake may coexist with nonosmotic ADH release from infection and nausea.
Management
Dapagliflozin is withheld and isotonic fluids are given with close monitoring. Serum sodium level is rechecked every 2–4 hours during active correction; urine studies are repeated after holding the SGLT2i. With restoration of effective circulating volume and clinical improvement, Uosm decreases and sodium rises in a controlled manner without hypertonic therapy. The key practical step is to avoid premature labelling as SIAD solely on the basis of a high Uosm in a patient on a flozin.
Vignette 2: Immune checkpoint inhibitor–related adrenal insufficiency masquerading as syndrome of inappropriate antidiuresis
A 62‑year‑old woman receiving nivolumab for metastatic lung cancer presents with progressive fatigue, nausea, dizziness, and new confusion. Serum sodium level is 118 mmol/l with hypotonicity. Urine is concentrated (Uosm, 520 mOsm/kg), with UNa of 70 mmol/l, and the patient appears clinically euvolemic, initially suggesting SIAD. However, blood pressure is low‑normal with postural drop, and she reports headache.
Bedside interpretation
In ICI‑treated patients, euvolemic hypotonic hyponatremia with concentrated urine must prompt mandatory exclusion of adrenal insufficiency (with or without hypophysitis) before SIAD is confirmed.
Management
A morning cortisol level (with or without ACTH level) is obtained urgently, but treatment is not delayed: intravenous hydrocortisone is administered (stress‑dosing), alongside isotonic fluids if hypotensive. Cortisol returns very low with inappropriately low / normal ACTH, consistent with secondary adrenal insufficiency. Thyroid function tests are checked, and levothyroxine is deferred until glucocorticoid replacement is established if central hypothyroidism is suspected. Serum sodium level improves after steroid replacement and supportive care. Ongoing endocrine follow‑up and shared‑care planning with oncology are arranged; decisions regarding continuation of ICI are individualized based on oncologic benefit and endocrine stability.
Treatment principles: prioritizing neurological safety and cause‑directed therapy
The above vignettes highlight why correction strategy and cause‑directed therapy must be tailored to symptom severity, acuity, and therapy‑specific pitfalls. Initial risk stratification should distinguish between acute and chronic hyponatremia and between symptomatic and asymptomatic presentations.The urgency of treatment depends on symptoms and the acuity of onset. Acute symptomatic hyponatremia is a medical emergency; chronic hyponatremia requires slower correction to reduce the risk of osmotic demyelination.5,15,16
Symptom‑based correction targets
In symptomatic hyponatremia, the immediate goal is neurological stabilization rather than normalization of sodium. An initial increase of 4–6 mmol/l (or clear clinical improvement) is usually sufficient; subsequent correction should proceed slowly within daily limits to minimize osmotic demyelination risk.
Practical symptom categories
Severe symptoms include seizure, coma, and impending respiratory failure. Moderately severe symptoms include confusion, persistent vomiting, marked headache, or severe agitation. Patients without significant neurological symptoms are managed with cause‑directed therapy and controlled correction.
Hypertonic saline (3% NaCl): bolus‑first strategy
For severe symptoms, administer 100–150 ml of 3% NaCl intravenously over 10–20 minutes, reassess clinically, and recheck serum sodium level after 20–30 minutes; repeat up to 2 additional boluses if symptoms persist, aiming for a 4–6 mmol/l rise. For moderately severe symptoms, a single bolus with reassessment is often sufficient; further boluses should be guided by symptom persistence and sodium trajectory.15,33 A ward‑ready protocol for hypertonic saline administration and monitoring is summarized in Table 6.
Abbreviations: see Table 2 |
|
When continuous infusion is used
If bolus therapy is impractical, or symptoms persist with an inadequate response, 3% NaCl may be given as a controlled continuous infusion (eg, approximately 0.5–1 ml/kg/h) with sodium level checks every 2–4 hours and frequent dose adjustment. Infusion should be reduced or stopped once the initial target increment is achieved to avoid overshoot.
Cause‑directed therapy for common phenotypes
In hypovolemic hyponatremia (eg, due to diarrhea, vomiting, diuretics), isotonic saline and correction of volume depletion are fundamental. In adrenal insufficiency, glucocorticoid replacement is causal therapy, and it typically results in rapid improvement in serum sodium level; primary adrenal insufficiency also requires mineralocorticoid replacement.21
Treatment of syndrome of inappropriate antidiuresis: from first‑line restriction to second‑line solute and aquaretics
In chronic SIAD, fluid restriction remains the first‑line therapy. If ineffective or not feasible, second‑line options include increasing solute intake with oral urea (supported by systematic review evidence), loop diuretics with oral salt supplementation, and vasopressin receptor antagonists, such as tolvaptan.8,15,22,23 Each approach requires monitoring to prevent overly rapid correction, particularly when the underlying stimulus for SIAD resolves (eg, discontinuation of the culprit drug, improvement of pain / nausea).
Where sodium‑glucose cotransporter 2 inhibitors may fit in treatment
In 2 randomized trials by Refardt et al,10,11 empagliflozin demonstrated efficacy as an off‑label adjunct for SIAD‑induced hyponatremia. When used off‑label, it should be positioned as an option for stable chronic SIAD under close monitoring, not as an emergency therapy for severe symptomatic hyponatremia. Because SGLT2is can worsen volume depletion, clinicians should avoid their use when hypovolemia is suspected or when frequent monitoring is not possible.
Avoiding overcorrection: prevention and rescue
Regardless of the hypertonic saline strategy, the major practical hazard is an abrupt transition to water diuresis with rapid overcorrection. Patients at the highest risk of osmotic demyelination include those with very low baseline sodium, malnutrition, alcoholism, liver disease, and hypokalemia. Correction limits are typically up to 10 mmol/l in the first 24 hours and up to 18 mmol/l in 48 hours; in high‑risk patients, stricter targets are often used.15,16 During active correction, the frequency of sodium monitoring should be tailored to neurological risk and the likelihood of a sudden water diuresis. In patients at a high risk of osmotic demyelination or when serum sodium level is changing rapidly, it should be rechecked every 4–6 hours, whereas in stable, lower‑risk patients, a 12–24‑hour interval is usually sufficient. A proactive strategy of desmopressin (1‑desamino‑8‑D‑arginine vasopressin [DDAVP]) clamp should be considered in high‑risk patients in whom a brisk aquaresis is anticipated (eg, reversal of the underlying trigger, abrupt diuretic withdrawal) or when serum sodium is rising faster than intended and urine output increases markedly. When there is concern for overcorrection, strategies include proactive or reactive desmopressin (DDAVP clamp) to stabilize water diuresis and, if needed, relowering of serum sodium level with hypotonic fluids.16,34
Treatment nuances in immune checkpoint inhibitor–related adrenal insufficiency
In suspected adrenal crisis, administer stress‑dose intravenous hydrocortisone immediately and treat hypotension with isotonic fluids; defer definitive endocrine confirmation until after stabilization. Once stable, coordinate longer‑term endocrine management (taper to physiological replacement; assess the need for mineralocorticoid replacement; address concurrent thyroid dysfunction) in alignment with endocrine and oncology guidance.12,21,28 Suggested baseline assessment, follow‑up timing (outpatient vs inpatient), and red flags prompting urgent reassessment for key modern therapies are summarized in Table 7. These intervals should be individualized to baseline sodium level, comorbidity burden, and the pace of change.
Therapy | Baseline (before start / early in therapy) | Planned follow‑up (typical timing) | Red flags → check sodium urgently / same day |
a Monitoring intervals should be individualized to baseline sodium, comorbidity burden, and the pace of change; symptomatic hyponatremia is a clinical emergency.
| |||
SGLT2is | Serum sodium in patients at risk; creatinine/eGFR; brief volume assessment (orthostasis, weight); review concomitant diuretics, low‑solute diet, recent GI losses |
| New / worsening dizziness or orthostasis; poor intake, vomiting / diarrhea; rising creatinine/AKI; marked polyuria / volume depletion; confusion, falls |
ICIs | Serum sodium; morning cortisol ± ACTH; TSH and free T4 (and symptom screen for hypophysitis); document baseline fatigue / headache; patient education on warning symptoms | Routine endocrine surveillance aligned with oncology pathway (commonly every 4–6 weeks early, then per protocol). If hyponatremia occurs: endocrine workup immediately and repeat Na+ measurement based on severity (symptomatic or inpatient → every 4–6 h during active management) | Hypotension, syncope, shock; persistent vomiting; hypoglycemia; altered mental state; severe new fatigue “out of proportion”; new headache / visual symptoms → treat as possible adrenal crisis; do not delay steroids in unstable patient |
Targeted anticancer agents / chemotherapy | Serum sodium, potassium, glucose; creatinine/eGFR; baseline GI status (diarrhea / vomiting risk); medication review (opioids, antiemetics, SSRIs, diuretics); assess nutritional / solute intake | Outpatient on treatment: electrolytes at each cycle and whenever toxicity develops (diarrhea, vomiting, fever). Inpatient oncology: reassess frequently; if Na+ changing, AKI, sepsis, large IV fluid shifts, or active correction → every 4–6 h until stable | Any acute deterioration (sepsis, AKI, escalating diarrhea / vomiting); rapid weight change / volume shifts; new neuro symptoms; “mixed” patterns after fluids / diuretics → repeat urine / Na+ when physiology changes |
Prevention and monitoring: practical recommendations
Prevention starts with identifying vulnerable patients (older age, frailty, low solute intake, concurrent diuretics, baseline borderline sodium) and with baseline electrolyte assessment before initiating therapies that can influence water balance.8 In hospitalized patients, routine medication reconciliation is a high‑yield intervention to identify potential contributors.
Although SGLT2is are being explored as therapy for SIAD, their diuretic effect can precipitate volume depletion in susceptible patients. After initiation, monitor volume status and renal function and consider repeating serum sodium assessment in patients with baseline hyponatremia, concomitant diuretics, or poor oral intake. Provide clear sick‑day guidance (temporary discontinuation during dehydration, vomiting / diarrhea, or reduced intake) to reduce the risk of hypovolemia and AKI.
Immune checkpoint inhibitors
Baseline and periodic assessment of serum sodium level and endocrine function (morning cortisol with or without ACTH, TSH, fT4) is advisable and should be aligned with oncology toxicity management pathways. Patients and clinicians should be alerted that new fatigue, nausea, dizziness, headache, or hypotension may signal adrenal insufficiency and warrant urgent evaluation. Clear escalation pathways reduce delays to stress‑dose steroids in suspected crisis.12,28,29
Oncology inpatients receiving targeted therapies or chemotherapy
Monitoring should be intensified during toxicity episodes (diarrhea, vomiting, mucositis), infections, and AKI. Because hyponatremia is often multifactorial, prevention requires both supportive care (managing gastrointestinal losses, ensuring adequate solute intake) and repeated reassessment as the clinical picture evolves.13,14
Research gaps
For SGLT2is in SIAD, larger pragmatic trials are needed to define which phenotypes benefit most, and how this approach compares with urea or tolvaptan with regard to efficacy, safety, patient‑reported outcomes, and cost‑effectiveness.10,11,22,23
For ICIs, improved shared‑care protocols are needed to streamline endocrine testing in acute presentations and to quantify the frequency with which endocrine causes are missed in routine practice. Standardized monitoring may reduce morbidity from preventable adrenal crisis.12,25
Conclusions
Modern therapies have reshaped the differential diagnosis of drug‑related hyponatremia. SGLT2is can confound urine indices and may be therapeutically useful in selected chronic SIAD cases, whereas ICIs raise the risk by increasing the likelihood of adrenal insufficiency, a reversible but potentially fatal cause of SIAD‑like hyponatremia. A structured diagnostic approach that integrates medication timing and early endocrine testing, combined with neurological safety–focused correction strategies, can improve outcomes in this increasingly prevalent clinical scenario.
- Waikar SS, Mount DB, Curhan GC. Mortality after hospitalization with mild, moderate, and severe hyponatremia. Am J Med. 2009; 122: 857‑865.
- Corona G, Giuliani C, Parenti G, et al. Moderate hyponatremia is associated with increased risk of mortality: evidence from a meta‑analysis. PLoS One. 2013; 8: e80451.
- Corona G, Norello D, Parenti G, et al. Hyponatremia, falls and bone fractures: a systematic review and meta‑analysis. Clin Endocrinol (Oxf). 2018; 89: 505‑513.
- Renneboog B, Musch W, Vandemergel X, et al. Mild chronic hyponatremia is associated with falls, unsteadiness, and attention deficits. Am J Med. 2006; 119: 71.e1‑71.e.718.
- Adrogué HJ, Madias NE. Hyponatremia. N Engl J Med. 2000; 342: 1581‑1589.
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION