How long does chronic thromboembolic pulmonary hypertension take to develop? Two cases of post-thrombotic complete occlusion of the left pulmonary artery

 CC BY 4.0
CC BY 4.0
How long does chronic thromboembolic pulmonary hypertension take to develop? Two cases of post-thrombotic complete occlusion of the left pulmonary artery
Chronic thromboembolic pulmonary hypertension (CTEPH) is a rare, long‑term complication of acute pulmonary embolism (APE) with a poor prognosis, if left untreated.1,2 Most published studies report the occurrence of CTEPH within 2 years after an episode of APE.3,4 However, the timing of CTEPH development is unknown; 2‑year follow‑up after APE may be too short, as some patients develop PH at a later time. We present a case of 2 women, who developed CTEPH 8 years after APE diagnosis.
The patients, born in 1987 and 1968, were diagnosed with APE in September 2010 and August 2011, respectively. Neither had been treated for chronic diseases prior to APE, and no thrombophilias were subsequently identified. In the case of the younger woman, the risk factors for thromboembolism included obesity and hormone therapy. The other patient sustained a patellar fracture in July 2011 with cast immobilization, and she was on oral contraceptives.
In accordance with recommendations valid in 2010–2011,5 both patients initially received body‑weight‑adjusted low‑molecular‑weight heparin followed by vitamin K antagonists. International normalized ratio (INR) monitoring was suboptimal: in the younger patient, it was measured only sporadically and was mostly nontherapeutic, while in the older woman, INR remained below the therapeutic range for the first 2 months. Despite prolonged anticoagulation therapy with acenocoumarol, both patients reported a marked reduction in exercise tolerance, and CTEPH workup was initiated. There was no evidence of recurrent PE.
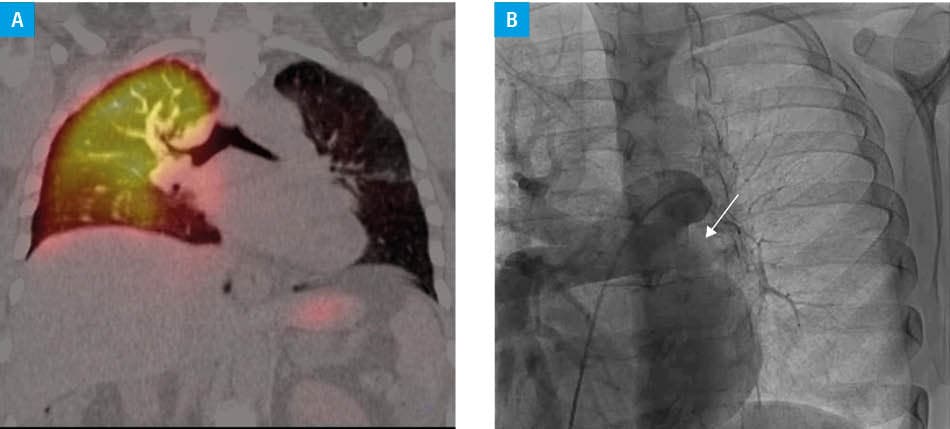
In 2012, echocardiography showed no abnormalities, including no signs of right ventricular pressure overload. N‑terminal pro–B‑type natriuretic peptide levels and 6‑minute walk test (6MWT) results were within normal limits. Nevertheless, both patients reported reduced exercise tolerance, which limited their return to normal social and professional activities. Lung perfusion scintigraphy was therefore performed, showing no perfusion in the left lung in either patient (Figure 1A). Complete occlusion of the left pulmonary artery (LPA) was later confirmed on computed tomography and invasive pulmonary angiography (Figure 1B). Right heart catheterization (RHC) demonstrated a hemodynamic profile considered normal according to the then‑current European Society of Cardiology / European Respiratory Society guidelines.1 Both women were evaluated by a cardiothoracic surgeon experienced in pulmonary endarterectomy (PEA), and were deemed unsuitable for surgery owing to procedural risk and World Health Organization functional class I.
Both patients were monitored regularly with functional and laboratory tests, including 6MWT and echocardiography, whose results remained within normal limits. However, in 2019, the clinical status of both women worsened and RHC was repeated. Based on its results, CTEPH was diagnosed, and both patients underwent PEA, which led to an improvement in functional and hemodynamic parameters (Supplementary material, Table S1).
These briefly described cases illustrate a clinical course in which CTEPH developed 8 years after APE, with RHC confirming a normal hemodynamic profile despite complete occlusion of the LPA. The period of PH development was oligosymptomatic, and most recommended diagnostic test results showed no abnormalities. As early as in 1976, Tilkian et al6 described chronic thromboembolic occlusion of the LPA. They also showed that most physical signs and laboratory workup yielded normal or nonspecific results, and that the perfusion lung scan was the best screening tool.6 Without lung perfusion scintigraphy, a misdiagnosis could have occurred, and our patients might have been considered cured of venous thromboembolism, with anticoagulation discontinued. Moreover, symptomatic APE survivors should undergo diagnostics for chronic thromboembolic pulmonary disease and be carefully monitored, as their follow‑up may need to be extended. It is worth emphasizing that, according to the current guidelines1, symptomatic patients with chronic thromboembolic pulmonary disease should undergo de‑obstructive treatment shortly after diagnosis.
- Humbert M, Kovacs G, Hoeper MM, et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: developed by the Task Force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS). Endorsed by the International Society for Heart and Lung Transplantation (ISHLT) and the European Reference Network on rare respiratory diseases (ERN‑LUNG). Eur Heart J. 2022; 43: 3618‑3731. | Crossref
- Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): the Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). Eur Heart J. 2020; 41: 543‑603. | Crossref
- Valerio L, Mavromanoli AC, Barco S, et al. Chronic thromboembolic pulmonary hypertension and impairment after pulmonary embolism: the FOCUS study. Eur Heart J. 2022; 43: 3387‑3398. | Crossref
- Durrington C, Hurdman JA, Elliot CA, et al. Systematic pulmonary embolism follow‑up increases diagnostic rates of chronic thromboembolic pulmonary hypertension and identifies less severe disease: results from the ASPIRE Registry. Eur Respir J. 2024; 63: 2300846. | Crossref
- Konstantinides SV, Torbicki A, Agnelli G, et al. 2014 ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2014; 35: 3033‑3069, 3069a‑3069k. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION