We present an echocardiographic examination of a 20‑year‑old patient with an unusual left ventricular (LV) tumor. The patient was asymptomatic, but echocardiography showed an additional structure in the LV. The N‑terminal pro–B‑type natriuretic peptide concentration was not elevated (100 pg/ml; reference range <125 pg/ml). Transthoracic echocardiography identified a tumor measuring approximately 17 mm × 11 mm, within the chordae tendineae of the mitral valve (Figure 1A and 1B).
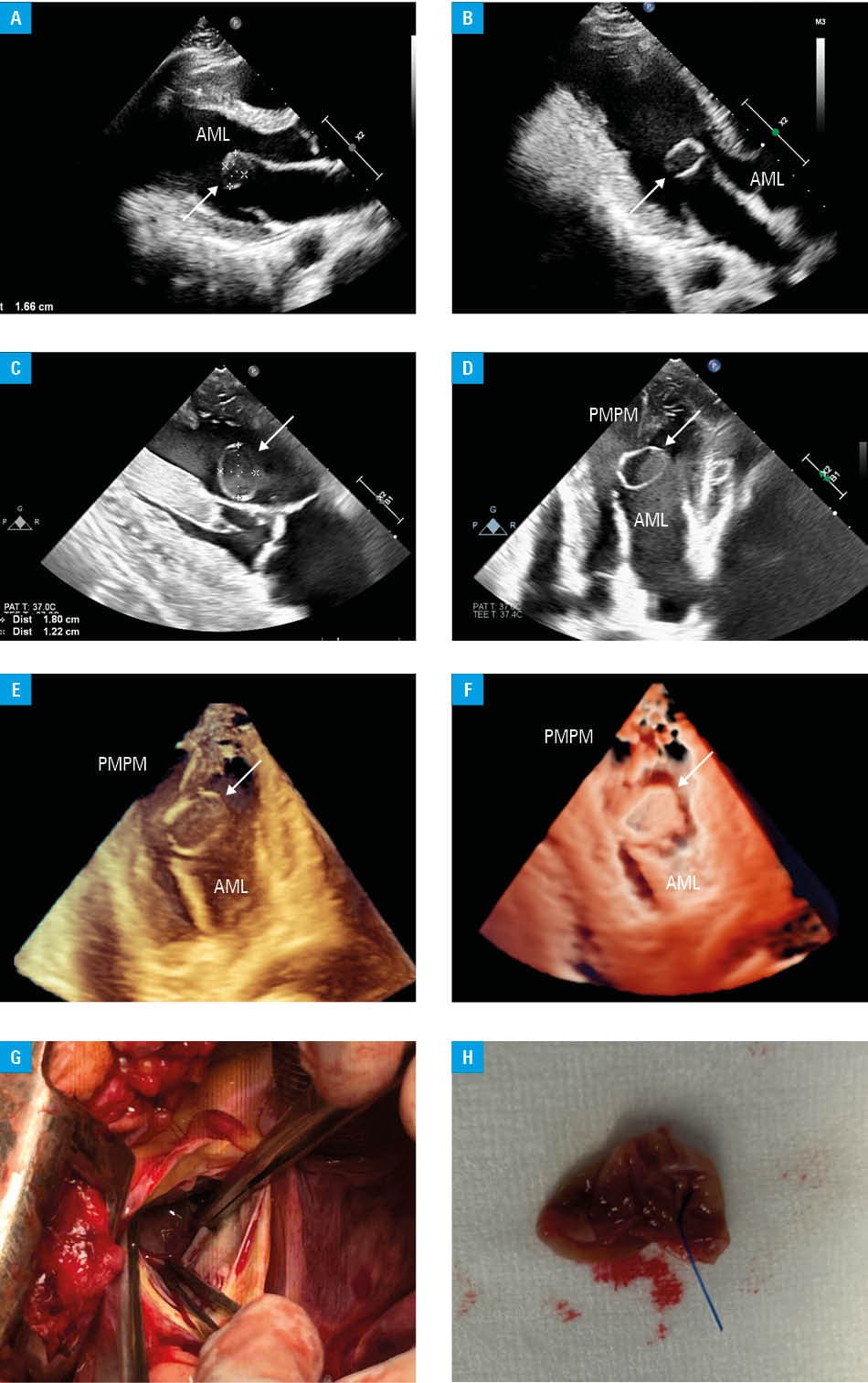
Abbreviations: AML, anterior mitral leaflet; PMPM, posteromedial papillary muscle
Transesophageal echocardiography confirmed the presence of a tumor measuring 18 mm × 12 mm. The tumor was attached to the chordae tendineae near the posteromedial papillary muscle, which connects with the anterior leaflet of the mitral valve (Figure 1C and 1D). Three‑dimensional (3D) imaging allowed for precise localization of the tumor and assessment of its morphology. The lesion was round, surrounded by a thin wall, highly mobile in synchrony with the heart’s movements, but did not cause narrowing of the LV outflow tract or pseudostenosis of the mitral valve (Figure 1E and 1F).
Owing to concerns regarding the risk of thromboembolic complications in a young, active, athletic man, a decision was made to perform cardiac surgery to remove the tumor. Intraoperative 3D echocardiography enabled precise localization and characterization of the tumor, and the surgery was performed without complications via ministernotomy and access through the aortic valve (Figure 1G and 1H).
Histopathological examination showed that the tumor was a blood cyst—an extremely rare benign tumor of the heart in adults.
Although cardiac blood cysts are rare in adults, they should be considered in the differential diagnosis of cardiac tumors. It is challenging to distinguish cardiac blood cysts from other cardiac tumors, such as myxomas, fibroelastomas, fibromas, hemangiomas, vegetations, or thrombi. Echocardiography is the first and most important tool in diagnosing a tumor, which usually occurs in the atrioventricular valves of the heart but can also be found in other locations. As a congenital malformation, cardiac blood cysts are common in infancy, regress with time, and are very rare in adults.1 Furthermore, according to some studies, apart from congenital cases, intracardiac cysts may be acquired as a result of trauma or surgery.2
Owing to their rarity, no guidelines exist for their management. It appears that due to the potential for thromboembolic complications in large tumors located in the left heart cavities, surgical removal of the tumor should be considered in such cases.3 Furthermore, surgery allows for histopathological examination and exclusion of malignancy.
- Kühn A, Schreiber C, Weirich G, Vogt M. Intracardiac blood cyst: rare finding in a complex congenital heart lesion. Eur Heart J. 2012; 33: 229. | Crossref
- Ramírez‑Mesías, Contreras‑Valero J, Pinilla‑Monsalve G, Vesga‑Reyes C. Blood cyst of the mitral valve diagnosed in an adult after systemic thrombolysis. Case Rep Cardiol. 2020; 2 020: 4320269. | Crossref
- Bortolotti U, Vendramin I, Lechiancole A, et al. Blood cysts of the cardiac valves in adults: review and analysis of published cases. J Card Surg. 2021; 36: 4690‑4698. | Crossref
ARTICLE INFORMATION