Cat scratch disease (CSD), caused by Bartonella henselae, is a worldwide zoonotic disease that typically peaks in the fall and winter. It is more prevalent in warm, humid areas. Cats are the primary reservoirs and often asymptomatic bacteremic carriers. Human infection typically follows a cat scratch or bite. The reported incidence is 6.4 per 100 000 adults. CSD usually causes benign, self‑limited regional lymphadenitis. However, in immunocompromised individuals, it may progress to disseminated disease involving the liver, spleen, eyes, or skin.1-4 In these cases, diagnosis is often delayed, and prompt, targeted antimicrobial therapy is crucial to prevent clinical deterioration.
We present a case of a 43‑year‑old man with end‑stage kidney disease, who underwent a deceased‑donor kidney transplant. Maintenance immunosuppression consisted of tacrolimus, mycophenolate mofetil, and prednisone. Approximately 4 months after the transplant, the patient was admitted to a hospital with high‑grade fever (up to 39 °C), drenching night sweats, and exertional dyspnea. Physical examination showed enlarged lymph nodes in the right cubital fossa and axilla, as well as multiple nonspecific nodular cutaneous lesions on the right hand (Figure 1A and 1B). Laboratory workup yielded markedly elevated inflammatory markers (C‑reactive protein [CRP], 105 mg/l; reference range [RR] <5 mg/l), leukopenia (leukocytes, 2.9 × 10³/µl; RR, 4–10 × 10³/µl), and serum creatinine level of 91 µmol/l (RR, 62–106 µmol/l). Microbiological investigations, including QuantiFERON‑TB test (QIAGEN, Venlo, the Netherlands), and serologies for Toxoplasma gondii, cytomegalovirus, Epstein–Barr virus, HIV, and SARS‑CoV‑2, were negative. Serial blood cultures were negative. Serum Candida mannan antigen testing yielded a borderline‑positive result. Color Doppler ultrasound identified hypervascular right axillary lymphadenopathy (Figure 1C and 1D). The epitrochlear (cubital) lymph nodes exhibited a comparable ultrasound pattern.
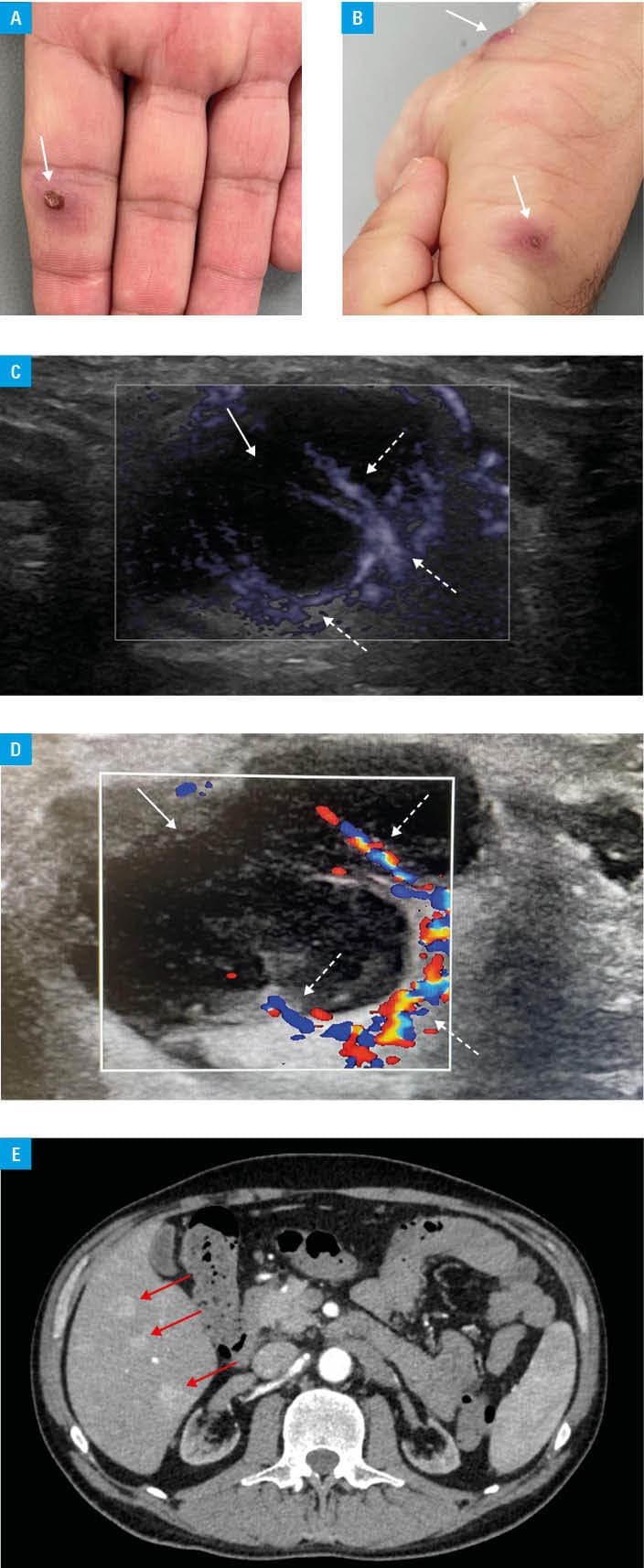
Arterial‑phase contrast‑enhanced computed tomography showed multiple sharply marginated hepatic lesions with pronounced arterial hyperenhancement (Figure 1E). Abdominal magnetic resonance imaging (MRI) corroborated these findings by demonstrating numerous contrast‑enhancing focal lesions accompanied by splenomegaly. During hospitalization, bilateral conjunctivitis developed.
Given the patient’s history of being scratched by a cat approximately 2 months before the symptom onset, together with the clinical presentation and imaging features, disseminated bartonellosis was strongly suspected.1-4 Unfortunately, polymerase chain reaction (PCR) blood testing was unavailable, precluding molecular confirmation of the infection. We initiated empiric doxycycline treatment (100 mg twice daily). Persistent fever prompted the addition of rifampin (300 mg/day). Mycophenolate mofetil was discontinued. Optimizing tacrolimus trough levels proved particularly challenging due to profound pharmacokinetic interaction with rifampin.
The patient exhibited gradual clinical improvement: fever and night sweats subsided, and CRP levels normalized. Rifampin was prescribed for a 14‑day course, whereas doxycycline was continued for 3 months due to the disseminated and severe nature of the infection, as well as the patient’s immunocompromised status.1,2 MRI performed after completing therapy demonstrated regression of the previously described hepatic lesions and resolution of splenomegaly.
This case highlights the difficulty of diagnosing fever of unknown origin in immunosuppressed patients. In solid organ transplant recipients, bartonellosis can closely resemble fungal or neoplastic disease.4,5 Hepatic lesions in a disseminated B. henselae infection most often reflect granulomatous (often necrotizing) inflammation with microabscesses. In immunocompromised hosts, however, they may also represent vasoproliferative / angioproliferative lesions related to an endothelial infection and an angiogenic response.2 Because culture confirmation is rare, and serologic assays are often unreliable in immunosuppressed patients, the absence of available PCR test limited diagnostic accuracy. Consequently, a meticulous exposure history, high clinical suspicion, and multimodal imaging were critical for the diagnosis. Early empiric treatment with doxycycline, with or without rifampin, combined with judicious modification of immunosuppression, may be lifesaving.1,2
- Puspitasari Y, Khairullah AR, Raharjo HM, et al. Uncovering the truth about cat‑scratch disease. Open Vet J. 2025; 15: 1895‑906. | Crossref
- Mikes BA, Zulfiqar H, Joel Chandranesan AS. Bartonellosis. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025 Jan. https://www.ncbi.nlm.nih.gov/books/NBK430874/. Accessed December 13, 2025.
- Shamekhi Amiri F. Bartonellosis in chronic kidney disease: an unrecognized and unsuspected diagnosis. Ther Apher Dial. 2017; 21: 430‑440. | Crossref
- Bos F, Chauveau B, Ruel J, et al. Serious and atypical presentations of Bartonella henselae infection in kidney transplant recipients. Open Forum Infect Dis. 2022; 9: ofac059. | Crossref
- Boyle EM, Baillet C, Dupré C, et al. Bartonellosis mimicking post‑transplant lymphoproliferative diseases. Nephrol Dial Transplant. 2022; 37: 599‑601. | Crossref
ARTICLE INFORMATION