Mixed neuroendocrine–non-neuroendocrine neoplasm producing calcitonin: a diagnostic challenge



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Mixed neuroendocrine–non-neuroendocrine neoplasm producing calcitonin: a diagnostic challenge
A 78‑year‑old woman with no significant medical history was admitted to a department of internal medicine and endocrinology with a 2‑month history of progressive epigastric pain, watery diarrhea, fatigue, and unintended weight loss of 7 kg. Physical examination showed cachexia, muscle atrophy, and massive hepatomegaly extending to the right iliac fossa. There were no clinical signs of infection.
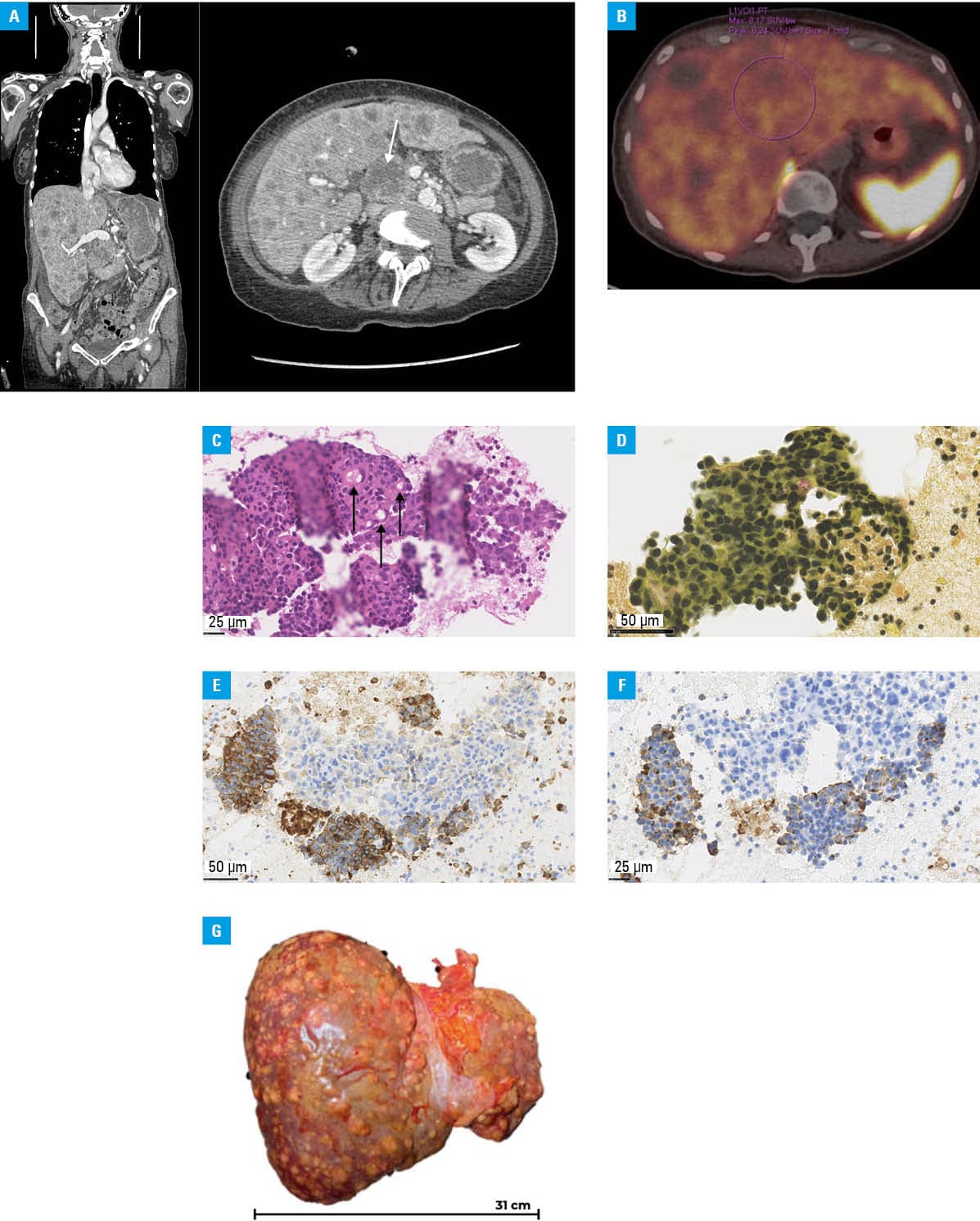
Abdominal ultrasound followed by contrast‑enhanced computed tomography (CT) identified a solid mass in the pancreatic head measuring 40 mm × 50 mm × 41 mm, with a 16‑mm dilatation of the pancreatic duct and multiple liver metastases (Figure 1A).
Laboratory test results indicated elevated aminotransferases (alanine aminotransferase, 176 U/l; reference range [RR], 7–30 U/l; aspartate aminotransferase, 155 U/l; RR, 5–40 U/l), and moderate hyperbilirubinemia (1.5 mg/dl; RR, 0.3–1 mg/dl). C‑reactive protein level was mildly increased (13.8 mg/l; RR <10 mg/l), and white blood cell count was elevated (17.01 × 109/l; RR, 4–10 × 109/l), without clinical evidence of infection. In contrast, procalcitonin concentration was markedly elevated at 108 ng/ml (RR <0.5 ng/ml).
Tumor markers showed a dual pattern: cancer antigen (CA) 19–9 at 800 U/ml (RR <34 U/ml) and carcinoembryonic antigen at 131 ng/ml (RR <4.9 ng/ml)—typical of non‑neuroendocrine malignancies—together with markedly increased chromogranin A (>900 µg/l; RR <100 µg/l) and neuron‑specific enolase at 710.3 ng/ml (RR, 9–12.4 ng/ml), suggesting neuroendocrine neoplasia. Given the considerably elevated CA 19–9 concentration, the subsequent histological diagnosis of adenocarcinoma was not unexpected. Serum calcium was at the upper limit of normal (2.57 mmol/l; RR, 2.15–2.6 mmol/l).
The discordantly elevated procalcitonin level in the absence of systemic inflammation suggested ectopic hormone production. Calcitonin concentration was profoundly increased at 1775 pg/ml (RR <5 pg/ml). As medullary thyroid carcinoma is the most frequent source of excessive calcitonin secretion, thyroid ultrasound was performed, demonstrating multiple partially confluent thyroid nodules. Ultrasound‑guided fine‑needle aspiration of the dominant lesion showed a benign thyroid nodule without cytological features of medullary thyroid carcinoma, thereby excluding the thyroid as the source of calcitonin hypersecretion.1
Short‑acting somatostatin analogues were administered but did not relieve the symptoms. Gallium‑68 DOTA‑D‑Phe1‑Tyr3‑octreotate positron emission tomography/CT showed no radiotracer uptake in the liver (Figure 1B), indicating low or absent somatostatin receptor expression, which may be consistent with poorly differentiated neuroendocrine carcinoma.
Endoscopic biopsy showed features of ductal adenocarcinoma (Figure 1C and 1D). During hospitalization, the procalcitonin level remained markedly elevated, reaching 141 ng/ml on day 2 and 145 ng/ml on day 9, and subsequently increasing to 487.5 ng/ml, paralleling clinical deterioration. The patient’s condition worsened rapidly, with progressive cholestasis and development of hepatic encephalopathy. Despite endoscopic retrograde cholangiopancreatography and supportive palliative care, the patient died on day 24 of hospitalization.
Autopsy confirmed mixed neuroendocrine–non‑neuroendocrine neoplasm (MiNEN) involving ductal adenocarcinoma and calcitonin‑positive neuroendocrine carcinoma components (Figure 1E–1G). The Ki‑67 proliferation index of the neuroendocrine component was 30%, determined manually by counting 1000 tumor cells in the region of highest nuclear labeling (hot spot). According to the World Health Organization, MiNENs are defined as tumors containing both components, each accounting for at least 30% of the tumor mass.2 Prognosis depends on tumor grade and is driven by the more aggressive component. Surgical resection remains the gold standard when feasible, and may be combined with systemic treatment.3
Calcitonin production by pancreatic neuroendocrine tumors is exceedingly rare, with only a limited number of cases reported. The most frequent symptoms include diarrhea, abdominal pain, and weight loss.4 This case highlights that markedly elevated serum procalcitonin and calcitonin concentrations in the absence of infection warrant consideration of malignancy. If medullary thyroid carcinoma is ruled out, neuroendocrine neoplasm should be taken into account.
- Bae YJ, Schaab M, Kratzsch J. Calcitonin as a biomarker for medullary thyroid carcinoma. Recent Results Cancer Res. 2025; 223: 155‑182. | Crossref
- de Mestier L, Cros J, Neuzillet C, et al. Digestive system mixed neuroendocrine‑non‑neuroendocrine neoplasms. Neuroendocrinology. 2017; 105: 412‑425. | Crossref
- La Rosa S, Sessa F, Uccella S. Mixed neuroendocrine‑non‑neuroendocrine neoplasms (MiNENs): unifying the concept of a heterogeneous group of neoplasms. Endocr Pathol. 2016; 27: 284‑311. | Crossref
- Döring A, Perren A, Pfarr N, et al. Whole exome sequencing of calcitonin‑producing pancreatic neuroendocrine neoplasms (CT‑pNENs): molecular characterization of a rare tumor entity. Front Oncol. 2023; 13: 1160921. | Crossref
ARTICLE INFORMATION