Breast metastases from extramammary malignancies are uncommon, accounting for 0.3%–2.7% of all breast tumors.1 The most frequent sources include melanoma, lymphoma, and lung carcinoma.1,2 Metastatic involvement of both breasts is even less frequent and often reported in small series / case reports.2 In pregnancy, physiological breast lesions can obscure radiological findings, while pregnancy‑associated breast cancer (PABC) itself carries unique diagnostic and therapeutic considerations.3 The distinction between BC and metastatic disease has critical therapeutic and prognostic implications, as treatment strategies differ considerably.1 We describe a unique case of bilateral breast metastases from lung adenocarcinoma diagnosed in the third trimester of pregnancy.
A 32‑year‑old woman, gravida 1 at 32+5 weeks of gestation, was admitted to our hospital with a suspicion of neoplastic disease. Her medical history included hypothyroidism diagnosed during pregnancy. Maternal history of breast carcinoma was reported. On admission, the patient complained of persistent lumbar pain. Neurological evaluation showed no focal deficits at presentation, though subsequent progression of neurological symptoms occurred during hospitalization. Physical breast examination demonstrated palpable, ill‑defined nodules in both breasts, without axillary lymphadenopathy. Given the pregnancy context and bilateral lesions, the differential diagnosis included PABC, multifocal primary BC, and metastases to the breast.1,2 The patient underwent cesarean section at 32+5 weeks due to oncologic indications.
Laboratory workup yielded normocytic anemia (hemoglobin, 8.9 g/dl; reference range [RR], 12–16 g/dl), elevated inflammatory markers (C‑reactive protein, 76–179 mg/l; RR <5 mg/l), and increased tumor markers (CA 19–9, 59.2 U/ml; RR <39 U/ml; AFP, 67.2 IU/ml; RR <5.8 IU/ml; CEA, 41.3 ng/ml; RR <5.2 ng/ml).
Computed tomography identified an infiltrative mass in the right upper lobe (31 mm × 74 mm), pleural effusion, as well as multiple bone metastases, multiple liver metastases, adrenal and renal lesions, and skeletal metastases. Mammography and breast ultrasound showed bilateral irregular, well‑defined, hypoechogenic breast nodules (14–19 mm; Breast Imaging Reporting and Data System, 4c). Such lesions can mimic primary BC, including triple‑negative phenotypes, which is why tissue diagnosis with immunohistochemistry is the golden standard.4 Figure 1A–1F shows the diagnostic imaging performed.
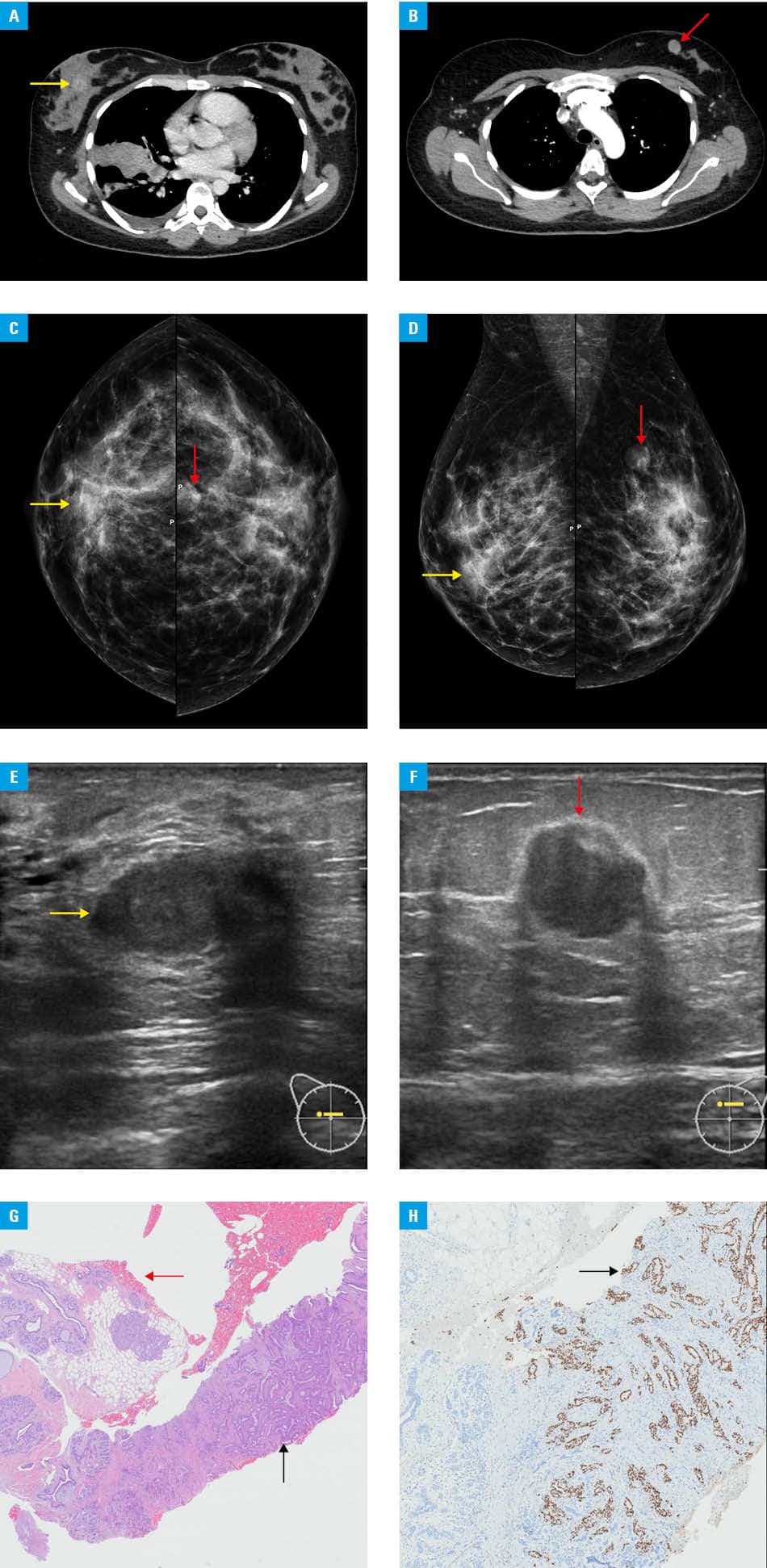
Liver biopsy demonstrated adenocarcinoma—CK7+, TTF1+, HER2–, and Ki67 of approximately 42%—consistent with pulmonary origin. Breast biopsies in both cases showed adenocarcinoma metastatis immunoprofile: CK7+/TTF1+/ER–/PR–/HER2–/GATA3–/GCDFP–/mammaglobin–. The result supported lung origin rather than primary breast carcinoma. Microscopic images of histology samples are presented in Figure 1G and 1H.
Key features that can distinguish between metastatic and primary breast carcinoma include: absence of an in‑situ component, multiplicity / bilaterality, and a lack of breast markers, such as ER/PR/HER2/GATA3/GCDFP/mammaglobin, with positive lung markers (TTF‑1).
The treatment proposed by a multidisciplinary board included stereotactic radiotherapy for brain metastases, brachytherapy for ocular metastasis, and systemic therapy (chemotherapy or immunotherapy) pending molecular testing (programmed cell death ligand 1 and next generation sequencing). The patient remained clinically stable and was discharged with follow‑up scheduled for oncology, ophthalmology, radiotherapy, and palliative care. The therapy consisted of paclitaxel, gemcitabine, and radiotherapy of the brain. The treatment followed current standards of care.5
Metastatic breast disease originating from lung cancer is a rare clinical condition, even rarer during pregnancy.1,2 Bilateral breast metastases are uncommon and may mimic primary BC, delaying correct diagnosis.4 This case illustrates that accurate immunohistochemistry is crucial: coexpression of CK7 and TTF‑1 with negativity for GATA3/ER/PR/HER2/GCDFP/mammaglobin is strong evidence of pulmonary origin rather than primary mammary carcinoma with matching clinical symptoms.6,7 Early multidisciplinary involvement is essential to balance maternal‑fetal considerations in pregnancy‑associated oncologic scenarios.3 Bilateral breast lesions in pregnancy can represent metastases from malignancies, such as lung adenocarcinoma. Immunohistochemistry is the golden standard to distinguish metastasis from primary breast carcinoma and select therapy. Multidisciplinary management according to current guidelines can individualize care in complex presentations.
- Picasso R, Pistoia F, Zaottini F, et al. Breast metastases: updates on epidemiology and radiologic findings. Cureus. 2020; 12: e12258. | Crossref
- Moreno‑Astudillo L, Villaseñor‑Navarro Y, Sánchez‑Goytia V, et al. A case series of breast metastases from different extramammary malignancies and their literature review. Case Rep Radiol. 2019; 2 019: 9454201. | Crossref
- Galati F, Magri V, Arias‑Cadena PA, et al. Pregnancy‑associated breast cancer: a diagnostic and therapeutic challenge. Diagnostics (Basel). 2023; 13: 604. | Crossref
- Ding J, Gu H, Yang Z, et al. Breast metastasis from lung adenocarcinoma: a case report and review of the literature. Front Oncol. 2024; 14: 1370453. | Crossref
- Politi K, Herbst RS. Lung cancer in the era of precision medicine. Clin Cancer Res. 2015; 21: 2213‑2220. | Crossref
ARTICLE INFORMATION