Skin lesions in inflammatory bowel disease: effect of the disease or its modern treatment?

 CC BY 4.0
CC BY 4.0
Skin lesions in inflammatory bowel disease: effect of the disease or its modern treatment?
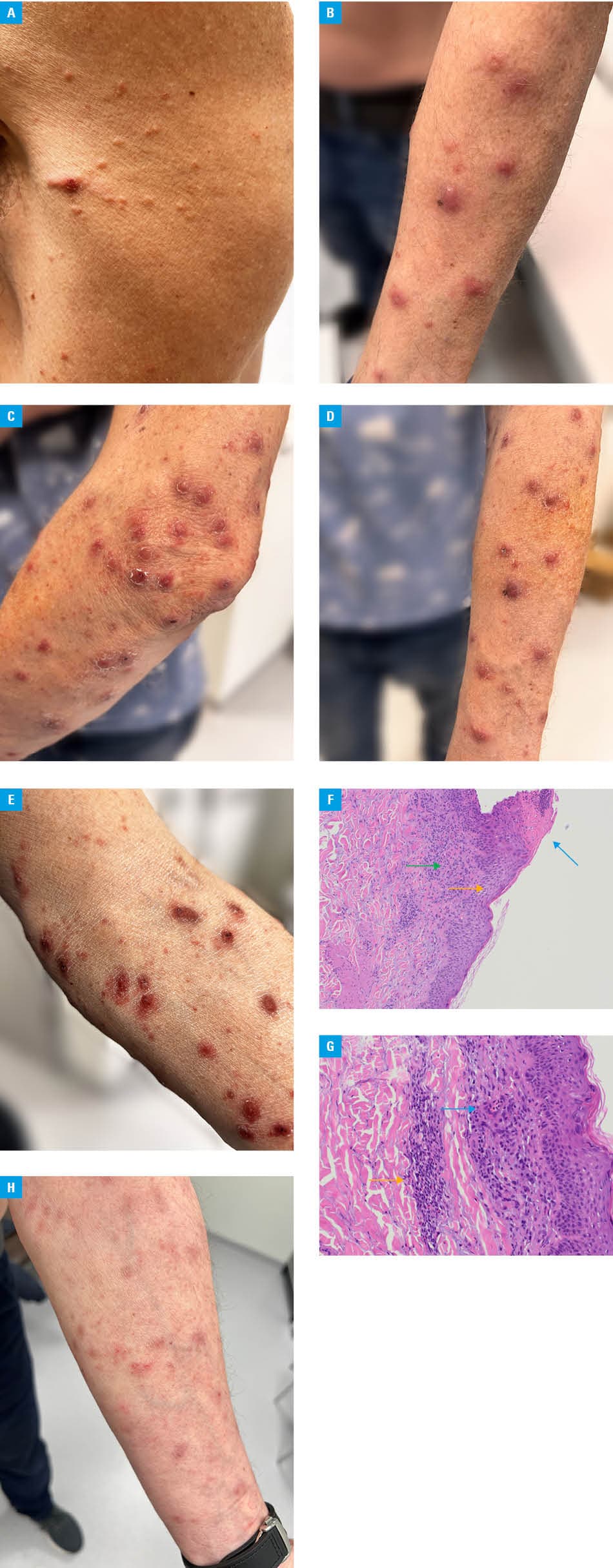
A 66‑year‑old man with inflammatory bowel disease (IBD) developed an unexpected dermatologic complication during infliximab therapy. The patient was diagnosed with IBD in 2009, first classified as ulcerative colitis, and in 2016 re‑evaluated as Crohn disease. Biologic therapy with infliximab (anti‑tumor necrosis factor α [TNF-α]) was initiated and well tolerated for 9 months. However, approximately 1 week after the seventh infliximab dose, a polymorphic rash developed on the trunk and extremities. The patient’s general physical condition remained good, with no fever or infection signs, and gastrointestinal symptoms in remission, although progressive peripheral joint pain was reported. Dermatologic examination showed small, linearly distributed papular lesions on the hips, thighs, and trunk (Figure 1A), as well as predominantly nodular lesions with scattered pustules on the forearms (Figure 1B). A history of intermittent erythematous, scaly facial lesions was noted, with prior improvement following topical tacrolimus use, and occurrence before the initiation of infliximab.
Given the clinical presentation, concerns arose regarding cutaneous lymphoma or lymphomatoid papulosis, a rare lymphoproliferative disorder. Laboratory findings showed no significant systemic inflammation or hematologic abnormalities.
Serum infliximab level was high (>20 μg/ml; reference range, 3–7 μg/ml) with no antidrug antibodies, though measured 3 weeks postdose. Awaiting the skin biopsy results, systemic corticosteroids were administered, with the lesions initially evolving in appearance (Figure 1C–1E). Histopathologic examination demonstrated atrophic epidermis with mild spongiosis, basal layer hyperpigmentation, and a perivascular lymphocytic infiltrate with scattered eosinophils and neutrophils. Direct immunofluorescence was negative for immunoglobulin deposits (Figure 1F and 1G).
Overall, the findings were most consistent with a drug‑induced reaction, with infliximab being the most probable causative agent. Importantly, TNF-α inhibitor therapy was suspended, while the patient’s concomitant medications were continued. This was accompanied by a gradual resolution of the lesions (Figure 1H) and no recurrence of cutaneous manifestations, further supporting infliximab as the likely trigger.
Although anti–TNF-α therapy in IBD has a relatively good safety profile, paradoxical autoimmune dermatological reactions are a known complication, including: psoriasiform eczema or dermatitis (ill‑defined itchy macules, papules, or squamous lesions; often with superinfection), psoriasis (typical plaque, guttate, and even pustular type), and cutaneous lupus.1 These reactions are frequently polymorphic and typically occur in the absence of systemic symptoms, whereas nodular lesions are distinctly uncommon. It is postulated that a possible etiology might be a result of imbalance between TNF and interferon-α, an important cytokine for induction of autoimmune skin conditions, produced by dermal plasmacytoid dendritic cells.2 Cutaneous manifestations may arise weeks to months after initiation of anti–TNF-α therapy.1 While some patients can be successfully managed with skin‑directed therapy without discontinuing the anti–TNF-α agent, extensive, refractory, or diagnostically concerning eruptions may necessitate temporary cessation of infliximab or switching to an alternative biologic agent.2
This case highlights the need for thorough differential diagnosis in TNF-α inhibitor recipients, especially when dermatologic findings mimic serious conditions, such as lymphoproliferative dermatoses. The emergence of extensive skin lesions may necessitate temporary discontinuation of therapy for the underlying disease, highlighting the importance of prompt diagnosis to minimize treatment delays.1,3,4 Early recognition and multidisciplinary collaboration were essential in establishing the correct diagnosis and guiding appropriate therapeutic decisions.
- Segaert S, Hermans C. Clinical signs, pathophysiology and management of cutaneous side effects of anti‑tumor necrosis factor agents. Am J Clin Dermatol. 2017; 18: 771‑787. | Crossref
- Au M, Heddle G, Young E, et al. Anti‑tumour necrosis factor‑induced skin rashes in inflammatory bowel disease: a systematic review and evidence‑based management algorithm. Intern Med J. 2023; 53: 1854‑1865. | Crossref
- Xie W, Xiao S, Huang H, et. al. Incidence of and risk factors for paradoxical psoriasis or psoriasiform lesions in inflammatory bowel disease patients receiving anti‑TNF therapy: systematic review with meta‑analysis. Front Immunol. 2022; 13: 847160. | Crossref
- D’Haens GR, van Deventer S. 25 years of anti‐TNF treatment for inflammatory bowel disease: lessons from the past and a look to the future. Gut. 2021; 70: 1396‐1405. | Crossref
ARTICLE INFORMATION