Fibroblast growth factor 21: a useful surrogate marker of cardiovascular risk in rheumatoid arthritis
1 ,
,

 CC BY 4.0
CC BY 4.0
Fibroblast growth factor 21: a useful surrogate marker of cardiovascular risk in rheumatoid arthritis
Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune disorder marked by progressive joint destruction and systemic inflammation. It is associated with a significantly elevated risk of cardiovascular disease (CVD).1,2 According to the current European Society of Cardiology (ESC) guidelines,3 cardiovascular morbidity and mortality are increased by up to 50% in patients with RA. Furthermore, CVD has emerged as the leading cause of premature death in this population.2
The development of premature atherosclerosis in RA is multifactorial, driven by both traditional and disease‑specific factors. RA‑specific mechanisms, such as chronic systemic inflammation, oxidative stress, endothelial dysfunction, and glucocorticoid therapy, play a pivotal role in accelerating vascular damage and atherogenesis.1,2,4
Traditional cardiovascular risk models, such as Systematic Coronary Risk Evaluation 2 (SCORE2), SCORE2–Older Persons, or LIFEtime‑perspective Cardiovascular Disease 2 (LIFE‑CVD2), tend to underestimate cardiovascular risk in patients with RA. To address this limitation, current ESC guidelines recommend multiplying the calculated total CVD risk by a factor of 1.5 in this population.3 In response to this discrepancy, certain risk prediction tools, including the Cardiovascular Disease Risk Prediction Algorithm (QRISK3), have incorporated RA, systemic lupus erythematosus, and chronic glucocorticoid use as independent variables.5 However, the development of RA‑specific tools remains essential for more accurate cardiovascular risk assessment. The Expanded Cardiovascular Risk Prediction Score for Rheumatoid Arthritis (ERS‑RA) was designed to address this need. ERS‑RA integrates conventional cardiovascular risk factors with disease‑specific variables, such as patient‑reported health status, RA activity and duration, and glucocorticoid use.6
Early identification of RA phenotypes associated with an elevated cardiovascular risk—despite an absence of clinically detectable atherosclerosis—is essential for implementing effective preventive measures. In line with this, the European League Against Rheumatism (EULAR) recommends regular cardiovascular risk assessment in all patients with RA.7
Current research efforts are directed toward identifying biomarkers that characterize disease phenotypes linked to a heightened cardiovascular risk. Among these, C‑reactive protein (CRP) has been evaluated for its utility in estimating cardiovascular risk in RA patients.4 Increasing attention has also been paid to organokines—a diverse group of signaling molecules, including hepatokines, myokines, adipokines, and osteokines—that mediate interorgan and systemic communication. Emerging evidence indicates that organokines contribute to the persistence of systemic inflammation, immune dysregulation, stimulation of angiogenesis, and cartilage degradation, all of which lead to pronounced radiographic damage in RA.8 Adipokines, in particular, have been studied in relation to RA pathogenesis and progression.8,9 Some studies indicate that adipokines may function not only as prognostic biomarkers of disease severity,9 but also as predictors of heart failure hospitalizations and CVD‑related mortality in patients with RA.10
Fibroblast growth factor 21 (FGF21) is an adipokine expressed in response to emotional stress, physical exercise, cold exposure, and nutrient excess or deficiency, in adipose tissue, liver, and muscles. It also regulates lipid and glucose metabolism.8 The protective effect of FGF21 against atherosclerosis is driven by alleviation of endothelial dysfunction, inhibition of macrophage‑derived foam cell formation, and suppression of migration and proliferation of vascular smooth muscle cells. The beneficial influence of FGF21 on the myocardium is connected with the inhibition of cardiac hypertrophy, collagen production, and remodeling. Moreover, FGF21 decreases inflammation and oxidative stress, and prevents senescence, apoptosis, and pyroptosis of cardiomyocytes.11
FGF21 has emerged as a reliable prognostic marker for CVD,12,13 major adverse cardiovascular events, and all‑cause mortality among patients with coronary artery disease,14 as well as in individuals without clinically evident CVD.15 In patients with RA, elevated serum FGF21 levels have been observed,16 which are linked to physical functional decline and abnormal body composition.17,18 However, to date, no studies have directly evaluated the prognostic utility of FGF21 concentration in predicting cardiovascular outcomes specifically within the RA population.
Given the limitations of existing cardiovascular risk scores in RA, there is growing interest in identifying surrogate markers that may enhance predictive accuracy. This study aimed to investigate whether circulating levels of FGF21 are associated with an increased cardiovascular risk, as assessed by different risk scoring systems, in a cohort of 51 patients with RA.
Patients and methods
Population characteristics
A total of 51 patients with RA who fulfilled the 2010 American College of Rheumatology/EULAR classification criteria19 were enrolled in the study. Recruitment was conducted between April 2017 and August 2019 at the Department of Rehabilitation, Medical University of Bialystok, Poland. The research protocol was approved by the Bioethics Committee of the Medical University of Bialystok (R‑I‑002/234/2016), and was carried out in accordance with the principles outlined in the Declaration of Helsinki, with strict adherence to ethical standards throughout the research process. Written informed consent was obtained from all participants prior to their inclusion in the study.
Demographic and anthropometric data, including age, sex, weight, height (both measured at the research center), and body mass index (BMI) were collected for all participants. Detailed medical histories were obtained, focusing on RA duration, presence and duration of morning stiffness, comorbidities, present and past medication use, smoking status (categorized as current, former, never smoking), and a family history of CVD. Systolic and diastolic blood pressure (BP) measurements were obtained in accordance with current clinical recommendations. Radiographic evaluation of the hands and feet was conducted to assess structural joint damage. Disease activity was qualified using the Clinical Disease Activity Index (CDAI), while the patients’ functional disability level was measured using the modified Health Assessment Questionnaire (mHAQ) disability index.
Laboratory evaluations included complete blood count, rheumatoid factor, estimated glomerular filtration rate (eGFR), and lipid profile parameters (total cholesterol [TC], high‑density lipoprotein cholesterol [HDL‑C], low‑density lipoprotein cholesterol [LDL‑C], and triglycerides). The level of high‑sensitivity CRP (hs‑CRP; Roche Diagnostics, Rotkreuz, Switzerland) was also measured. eGFR was calculated using the Modification of Diet in Renal Disease equation.
FGF21 concentrations were measured from patient serum samples that were frozen and stored at –80 °C, using commercially available enzyme‑linked immunosorbent assay kits (R&D Systems, Minneapolis, Minnesota, United States) according to the manufacturer’s protocols.
Comorbidities were diagnosed as follows: arterial hypertension, based on in‑office BP measurements; hyperlipidemia, based on elevated TC, LDL‑C, or triglyceride levels; diabetes mellitus (DM), based on an increased fasting glucose level; goiter and thyroid nodules, based on ultrasonographic examination; Hashimoto disease, based on the presence of thyroid peroxidase and thyroglobulin antibodies; asthma, based on spirometry; gout, based on typical symptoms and high uric acid levels; antiphospholipid syndrome, based on previous episodes of venous thrombosis and the presence of antiphospholipid antibodies; chronic kidney disease, based on diminished eGFR; and depression was diagnosed by a psychiatrist.
Cardiovascular risk scores
Expanded Cardiovascular Risk Prediction Score for Rheumatoid Arthritis
The ERS‑RA estimates the 10‑year risk of cardiovascular morbidity in patients with RA.6 It incorporates conventional cardiovascular risk factors (sex, hyperlipidemia, hypertension, DM, and current smoking status) and 4 RA‑specific variables: disease duration longer than 10 years, disease activity measured by CDAI, functional disability assessed by mHAQ, and corticosteroid use. Risk scores were calculated using a publicly available Excel macro.20
Systematic Coronary Risk Evaluation 2
SCORE2 is recommended by the current ESC guidelines3 for estimating the 10‑year risk of fatal and nonfatal cardiovascular events, including myocardial infarction (MI), stroke, and aortic aneurysm, in individuals aged 40 to 69 years. This model incorporates traditional cardiovascular risk factors, such as age, sex, smoking status, systolic BP, and serum concentrations of TC, LDL‑C, and HDL‑C. According to the ESC guidelines, Poland is classified as a high‑risk country, so the dedicated online calculator for high‑risk populations was used.21
To improve cardiovascular risk estimation in patients with RA, a multiplication factor of 1.5 was applied to the calculated SCORE2 values, yielding a modified SCORE2 (mSCORE2), as recommended by the ESC guidelines. For patients with concomitant DM, the SCORE2‑DM calculator was used.22
LIFEtime‑perspective Cardiovascular Disease 2 model
The LIFE‑CVD2 model estimates both 10‑year and lifetime risks of CVD (MI, stroke), and CVD‑related mortality, as well as event‑free life expectancy for individuals aged 35 to 89 years.23
The model incorporates age, sex, smoking status, systolic BP, TC, LDL‑C, and HDL‑C concentrations, and the presence of type 2 DM. In addition, it accounts for lifestyle variables, such as daily step count and adherence to the Mediterranean diet, as well as medication use, including statins, ezetimibe, bempedoic acid, and antithrombotic drugs. According to this model, Poland is categorized as a country with a high cardiovascular risk. The risk was assessed using the online calculator.24
Cardiovascular Disease Risk Prediction Algorithm
QRISK3 estimates the 10‑year risk of cardiovascular morbidity (ischemic stroke, transient ischemic attack, MI, and coronary artery disease) in individuals aged 25 to 84 years.5
QRISK3 incorporates age, sex, ethnicity, smoking status (categorized as current, former, or never smoking), and a positive family history of angina or MI in a first‑degree relative under 60 years of age. Additional variables include systolic BP, BMI, TC‑to‑HDL‑C ratio, presence of type 1 or 2 DM, and treated hypertension. QRISK3 also incorporates new risk factors that enhance its predictive accuracy. These include RA, systemic lupus erythematosus, atrial fibrillation, chronic kidney disease (stage 3, 4, or 5), migraine, severe mental illness, use of corticosteroids or atypical antipsychotics, and erectile dysfunction. Risk scores were calculated using the online calculator.25
Statistical analysis
All statistical analyses were performed using R (version 4.4.2; the R Foundation for Statistical Computing, Vienna, Austria) and Statistica (version 13–3; StatSoft Polska, Kraków, Poland), with a significance level set at a P value below 0.05. Continuous variables were expressed as mean with SD or median with interquartile range (IQR), depending on their distribution. Normality of the distribution was assessed using multiple methods; primarily, we used the Shapiro–Wilk test, and further, the data were analyzed with descriptive statistics, including skewness and kurtosis metrics. Visual inspection was performed in justified cases. Homogeneity of variance was evaluated using the Levene test.
To examine the impact of predictors on 5 risk scores, we worked under the generalized linear model framework using linear regression. A 2‑step linear regression approach was employed. Predictors with P values below 0.05 in univariable analyses were initially included in multivariable models. A backward stepwise selection method was applied to refine the model. Multicollinearity was assessed using variance inflation factors (VIFs), with all included predictors satisfying the condition of VIF below 2. Model performance was evaluated using the coefficient of determination (R2) and adjusted R2.
Results
Demographic data
A total of 51 patients (46 women, 5 men) at a mean (SD) age of 48.8 (8.2) years and a median (IQR) disease duration of 12 (4.95–20.25) years were enrolled in the study. The mean CDAI score was 25 (12.12), indicating moderate disease activity.
Laboratory findings
The median hs‑CRP level was 2.88 (1.06–6.19) mg/l (reference range [RR], 0–3 mg/l), suggesting low laboratory disease activity. The median serum FGF21 level was 98.13 (42.96–187.72) pg/ml. The mean eGFR value was 92.08 (14.85) ml/min/1.73 m2, which falls within the normal range. Detailed baseline characteristics of the study population are presented in Supplementary material, Table S1.
Association with clinical parameters
Outcomes of univariable and multivariable linear regression models for all cardiovascular risk scores are summarized in Supplementary material, Tables S2−S5.
Since FGF21 was the only significant parameter in the LIFE‑CVD2 model–based lifetime risk, it was not possible to fit a stable multivariable regression model.
Methotrexate use was independently associated with a 5.1‑percentage point (pp) reduction in cardiovascular risk as assessed by the mSCORE2 in multivariable regression analysis (P = 0.02).
In multivariable regression models, each 1‑mg/dl increase in serum LDL‑C level corresponded to a rise by 0.04 pp in ERS‑RA (P = 0.02).
Serum hs‑CRP level was not associated with cardiovascular risk in any of the evaluated scoring systems (P = 0.27 for ERS‑RA; P = 0.37 for mSCORE2; P = 0.96 for LIFE‑CVD2 model 10‑year risk; P = 0.41 for LIFE‑CVD2 model lifetime risk; and P = 0.28 for QRISK3).
Associations between fibroblast growth factor 21 levels and cardiovascular risk prediction scores
Serum FGF21 levels were positively associated with an increased cardiovascular risk across all scoring systems in both univariable and multivariable analyses. Notably, in the LIFE‑CVD2 model, FGF21 was the only significant predictor of lifetime cardiovascular risk in the univariable regression model.
In univariable linear regression models, each 1‑pg/ml increase in the FGF21 concentration was associated with a 0.02‑pp increase in QRISK3 (P <0.001) and approximately 0.01‑pp increases in the other scales (P = 0.003 for LIFE‑CVD2 model lifetime risk, and P <0.001 for the remaining scores). Multivariable linear regression models confirmed these associations, with a 1‑pg/ml increase in FGF21 levels independently contributing to an approximate 0.01‑pp rise in cardiovascular risk across all scoring systems. Standardized β coefficients from multivariable analyses further highlighted the strength of these associations. A 1 SD increase in FGF21 was associated with increases of 0.44 SD in ERS‑RA (P <0.001), 0.34 SD in mSCORE2 (P = 0.002), 0.42 SD in LIFE‑CVD2 10‑year risk (P <0.001), and 0.47 SD in QRISK3 (P <0.001).
The relationships between FGF21 concentrations and cardiovascular risk prediction scores are summarized in Figure 1.
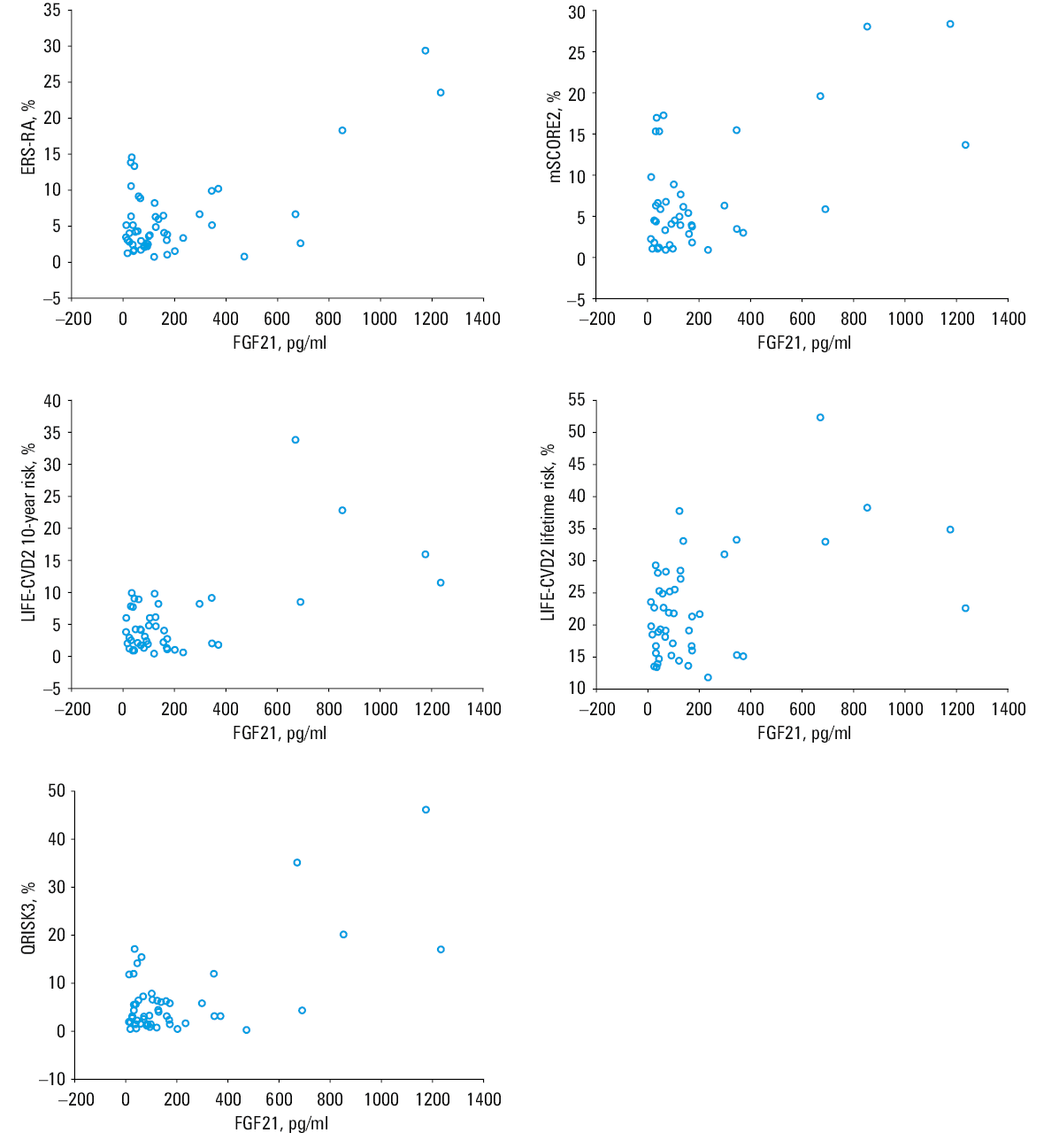
Abbreviations: ERS‑RA, Risk Prediction Score for Rheumatoid Arthritis; FGF21, fibroblast growth factor 21; LIFE‑CVD2, LIFEtime‑perspective Cardiovascular Disease 2; Mscore2, modified Systematic Coronary Risk Evaluation 2; QRISK3, Cardiovascular Disease Risk Prediction Algorithm
Impact of demographics
Sex and age were treated as confounders and were initially included in the regression analyses as potential predictors. Because both variables are components of the cardiovascular risk scores under investigation, sensitivity analyses were conducted with these variables excluded from multivariate regression models to assess the stability of the remaining associations. The results did not differ from those obtained in the original models.
Discussion
In this study, FGF21 levels were significantly and positively associated with cardiovascular risk across all investigated scoring systems. Although numerous studies have demonstrated a link between elevated serum levels of FGF21 and the development of CVD, poor clinical outcomes, and increased cardiovascular and all‑cause mortality,12,14,15 no research to date has specifically examined the prognostic value of FGF21 in cardiovascular risk assessment among patients with RA. To our best knowledge, this is the first study to evaluate the relationship between serum FGF21 levels and cardiovascular risk in an RA population. Furthermore, this study is the first to incorporate the novel LIFE‑CVD2 model, which estimates both the 10‑year and lifetime cardiovascular risk.
The mean FGF21 level in our study was 203.91 pg/ml, which was lower than the mean level of 260.57 pg/ml reported by Hulejova et al16 in RA patients with moderate clinical disease activity (mean Disease Activity Score‑28 for RA, 5.03) and high laboratory disease activity (mean CRP level, 22.76 mg/l). In a study by Liu et al,13 which investigated the predictive value of serum FGF21 level for vascular disease risk in adults with type 2 DM, mean serum FGF21 levels were lower in the healthy controls (123.9 pg/ml) and diabetic patients (197.2 pg/ml), but higher in the patients with carotid atherosclerosis or hypertension (305.9 pg/ml), and the highest in those with both conditions (505.5 pg/ml).
In a cross‑sectional study by Erre et al,4 involving 1251 patients from the CORDIS (Community Research and Development Information Service) database (mean age, 60.4 y; mean disease duration, 11.6 y), the mean plasma CRP level was 6.8 mg/l (RR, 0–4 mg/l), and the mean 10‑year cardiovascular risk estimated by the ERS‑RA model was 12.9%. A significant, positive, and independent association was observed between CRP levels and cardiovascular risk predicted by ERS‑RA. Specifically, each 20‑mg/l increase in CRP was associated with a 1% increase in predicted cardiovascular risk. Importantly, this relationship was independent of RA activity.
In our RA cohort, the mean ERS‑RA score was 6.05%, while the median hs‑CRP level was 2.88 mg/l, and was not significantly associated with cardiovascular risk in any of the evaluated scoring systems. As compared with the CORDIS population, our study group was younger, had a longer disease duration, and a higher number of patients were receiving conventional synthetic disease‑modifying antirheumatic drugs and anti‑inflammatory therapy, which may partially account for the absence of a relationship between hs‑CRP levels and cardiovascular risk.
In a study by Nowakowski et al,26 which assessed endothelial dysfunction via flow‑mediated dilation (FMD) of the brachial artery in RA patients (median age, 39.5 y; median disease duration, 5 y; median CRP level, 1 mg/l) without established cardiovascular risk factors, the subgroup with normal FMD (>7%) exhibited higher median CRP levels than the patients with impaired FMD (<7%). Our study population was older and characterized by longer disease duration and higher median hs‑CRP levels; however, we found no association between this inflammatory marker and cardiovascular risk.
Limitations
First, the relatively small sample size (n = 51) may limit the statistical power and generalizability of the findings. Second, as the study was conducted exclusively in Polish patients with RA, cardiovascular risk was assessed using mSCORE2 and LIFE‑CVD2 algorithms calibrated for high‑risk populations, which may restrict the applicability of the results to populations with different baseline cardiovascular risk profiles. Another important limitation is the cross‑sectional design and lack of longitudinal follow‑up, which precludes direct comparison between predicted cardiovascular risk and actual 10‑year cardiovascular morbidity and mortality. Long‑term prospective studies are warranted to validate the prognostic accuracy of the evaluated risk scores and further explore the utility of FGF21 as a surrogate biomarker in RA‑related cardiovascular risk stratification.
Conclusions
In conclusion, FGF21 may serve as a promising surrogate biomarker for enhancing cardiovascular risk assessment in patients with RA, aiding in identifying those who may benefit from intensified monitoring and targeted preventive interventions.
- Hansildaar R, Vedder D, Baniaaman M, et al. Cardiovascular risk in inflammatory arthritis: rheumatoid arthritis and gout. Lancet Rheumatol. 2021; 3: e58‑e70. | Crossref
- van der Woude D, van der Helm‑van Mil AHM. Update on the epidemiology, risk factors, and disease outcomes of rheumatoid arthritis. Best Pract Res Clin Rheumatol. 2018; 32: 174‑187. | Crossref
- Visseren FLJ, Mach F, Smulders YM, et al. ESC National Cardiac Societies; ESC Scientific Document Group. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2021; 42: 3227‑3337. | Crossref
- Erre GL, Cacciapaglia F, Sakellariou G, et al. C‑reactive protein and 10‑year cardiovascular risk in rheumatoid arthritis. Eur J Intern Med. 2022; 104: 49‑54. | Crossref
- Hippisley‑Cox J, Coupland C, Brindle P. Development and validation of QRISK3 risk prediction algorithms to estimate future risk of cardiovascular disease: prospective cohort study. BMJ. 2017; 357: j2099. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION