High prevalence of silent aneurysms and fibromuscular dysplasia in spontaneous coronary artery dissection survivors: analysis of the SCAD-POL Registry
Key words: aneurysm, extracoronary vascular abnormalities, fibromuscular dysplasia, spontaneous coronary artery dissection

 CC BY 4.0
CC BY 4.0
High prevalence of silent aneurysms and fibromuscular dysplasia in spontaneous coronary artery dissection survivors: analysis of the SCAD-POL Registry
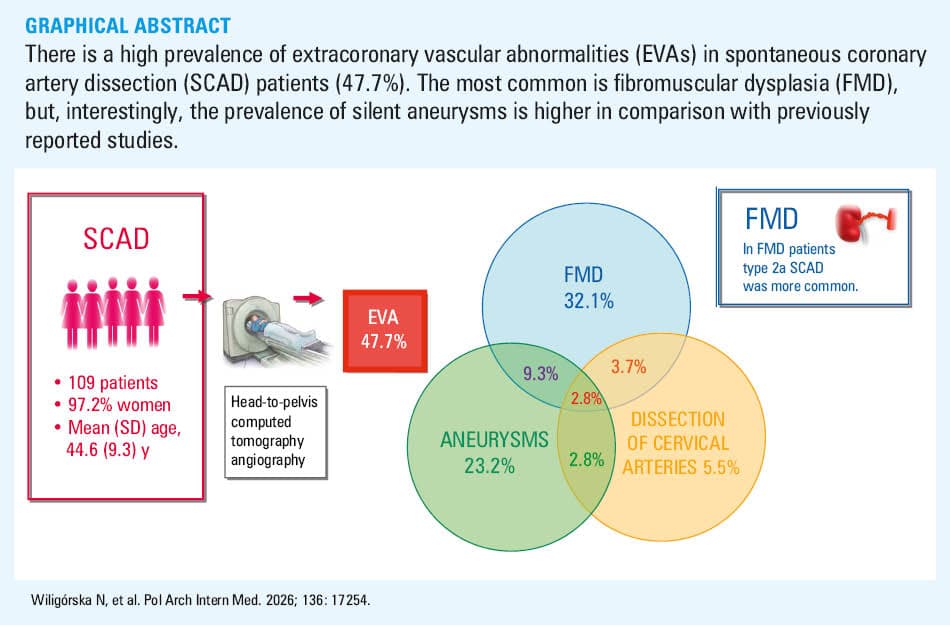
Introduction: Extracoronary vascular abnormalities (EVAs) have been found in patients with spontaneous coronary artery dissection (SCAD), suggesting that SCAD may reflect systemic vascular disease.
Objectives: The aim of this study was to assess the prevalence and characteristics of EVAs in SCAD survivors.
Patients and methods: A total of 109 consecutive patients with a history of SCAD underwent head‑to‑pelvis computed tomography angiography for EVA screening. EVAs were defined as the presence of fibromuscular dysplasia (FMD), aneurysm, or cervical dissections.
Results: EVAs were identified in 47.7% of the cohort. The prevalence of FMD was 32.1%, aneurysms were observed in 23.2% of the patients, and dissections of cervical arteries in 5.5%, while 9.3% of the patients presented with both FMD and aneurysms. FMD predominantly affected the renal (20.3%) and cervical (15.6%) arteries, while aneurysms were most commonly detected in the renal and splenic arteries (7.3% each). Multisite FMD was present in 8.3% of the patients. Aneurysms in more than 1 vascular bed were found in 4.6% of the cases. Cervical FMD was associated with migraine headaches in 58.8% of the patients and was clinically silent in 41.2%. All aneurysms were silent, however, 3 patients (12%) with intracerebral aneurysms required intravascular treatment due to a risk of rupture. In FMD patients, higher prevalence of type 2a SCAD (65.7% vs 43.1%; P = 0.03) and pregnancy‑associated SCAD (17.6% vs 4.2%; P = 0.03) was observed. The patients with type 2a SCAD had a 2.5‑fold higher likelihood of having FMD (odds ratio, 2.53; 95% CI, 1.09–5.87; P = 0.03).
Conclusions: This study showed a significant prevalence of EVAs in SCAD survivors, with silent aneurysms being more common than previously reported.
What's new?
This study evaluated extracoronary vascular abnormalities (EVAs) in spontaneous coronary artery dissection (SCAD), a distinct form of acute coronary syndrome. This is the first study that describes EVAs in a Polish SCAD population, as it presents the results of a multicenter Polish registry coordinated by the National Institute of Cardiology. Our findings showed a high prevalence of EVAs, identified in almost half of the study population (47.7%). It may be clinically relevant that silent aneurysms were observed in 23.2% of the patients, a higher proportion than in previously reported studies. This emphasizes the relevance of comprehensive vascular imaging in SCAD patients, as silent aneurysms may otherwise remain undiagnosed until rupture, which may potentially be associated with a high risk of morbidity and mortality. Importantly, 60% of the aneurysms were isolated and not associated with fibromuscular dysplasia (FMD). Another novel finding was that type 2a SCAD was associated with a 2.5‑fold higher likelihood of FMD. This highlights the importance of systematic vascular screening in SCAD patients, particularly in those with angiographic type 2a SCAD.
Introduction
Spontaneous coronary artery dissection (SCAD) has recently been recognized as an important and underdiagnosed cause of acute coronary syndrome (ACS), particularly in young and middle‑aged women. Due to their younger age, female sex, and the absence of typical atherosclerotic risk factors, patients with SCAD are at a higher risk of being misdiagnosed.1 SCAD patients account for up to 4% of ACS cases overall, but in women under 50 years of age the prevalence of SCAD is substantially higher.1,2
SCAD involves the development of a false lumen within the coronary artery wall, typically caused by an intramural hematoma or an intimal tear. This false lumen compresses the true lumen, reducing blood flow and causing myocardial ischemia or infarction.2 The diagnosis is usually established on coronary angiography. Intravascular imaging, such as intravascular ultrasound or optical coherence tomography can help make the SCAD diagnosis, but these techniques are associated with a risk of the dissection propagation and iatrogenic catheter‑induced dissection.3 In contrast with traditional coronary events, SCAD is not driven by thrombosis and plaque rupture and requires specific management strategies.
There is increasing evidence that SCAD may not be an isolated vascular event but rather a manifestation of systemic arteriopathy. This is supported by the frequent coexistence of extracoronary vascular abnormalities (EVAs), including fibromuscular dysplasia (FMD), aneurysms, and arterial dissections. EVAs may be clinically silent but can have important long‑term implications, particularly when intracerebral or visceral aneurysms are identified. The frequency of EVAs in SCAD varies widely among studies, depending on both the population and the imaging modality.1
SCAD has been associated with various extracoronary arteriopathies. The most frequent of these is FMD—a nonatherosclerotic, noninflammatory disease of arterial walls, typically occurring in the small and medium‑sized arteries, and also commonly affecting middle‑aged women.4 Angiographically, FMD is classified as either multifocal (string‑of‑beads pattern) or focal (tubular stenosis). Multifocal FMD is the most common type.2
The documented expert consensus is to recommend comprehensive brain‑to‑pelvis vascular imaging in SCAD patients.2,5,6 However, the impact of this approach on clinical implications for individual patients remains largely unknown. It is still under discussion whether identifying a particular type of EVA may help clinicians in tailoring treatment, follow‑up, and preventive strategies for secondary vascular events. Moreover, the impact of the EVA presence on patient prognosis is still debated.
Therefore, the primary aim of this study was to estimate the prevalence and characteristics of EVAs in patients with angiographically confirmed SCAD. We also sought to evaluate whether systematic evaluation of patients with SCAD, including whole‑body imaging, reveals clinically relevant abnormalities, and to characterize differences between the SCAD patients with and without different types of EVAs.
Patients and methods
The SCAD‑POL Registry is a retrospective, multicenter, observational study coordinated by the National Institute of Cardiology, Warsaw, Poland. Between 2018 and 2024, a total of 109 consecutive patients with angiographically confirmed SCAD were enrolled.
Demographic data and clinical comorbidity details (including traditional cardiovascular risk factors, such as hypertension, diabetes, smoking, or dyslipidemia) were collected. All coronary angiogram videos were obtained from local or referral hospitals for review at our center. They were reviewed by 2 invasive cardiologists (JK, AW) to confirm the diagnosis of SCAD and to classify SCAD types according to current consensus definitions.6
As part of the registry protocol, all patients underwent echocardiography and head‑to‑pelvis computed tomography angiography (CTA) to evaluate for EVAs. Imaging was performed routinely in all SCAD survivors, as it is recommended in international expert consensuses5 with the aim of screening for EVA. CTA was performed using a SOMATOM Force dual‑source CT scanner (Siemens, Erlangen, Germany), with collimation, 192 mm × 0.6 mm; resolution, 0.24 mm; rotation, 0.25 second; and slice thickness, 0.6–1 mm. The imaging protocol covered intracerebral, cervical, thoracic, abdominal, and pelvic arteries. Contrast‑enhanced arterial phase images were used to identify vascular abnormalities.
The diagnosis of FMD was based on the presence of sequential focal narrowing separated by focal dilations (string‑of‑beads appearance, ie, multifocal FMD) or segments of tubular stenosis (focal FMD) in at least 1 arterial bed, in accordance with the international consensus on FMD.7 Multisite FMD was defined as the presence of FMD stenoses in 2 or more of the vascular beds. Aneurysm was defined as an above 50% enlargement in the diameter of an artery in comparison with an adjacent normal arterial segment. Figure 1 shows typical multifocal FMD found in the renal arteries, and Figure 2 presents an example of intracerebral aneurysm. The diagnosis of dissection was made based on the presence of a dual‑lumen vessel. EVAs were defined as the presence of FMD, aneurysm, or dissection in any vascular bed. The study protocol was approved by the local ethics committee of the National Institute of Cardiology (IK.NPIA.2.24/III/2018). All participants provided fully informed written consent.


Statistical analysis
Categorical variables were expressed as counts and percentages. Continuous variables were expressed as mean (SD) or median with interquartile range, depending on data distribution. Normality was assessed using the Shapiro–Wilk test. Comparisons of normally distributed variables were made using the t test, while non‑normally distributed variables were analyzed with the Wilcoxon rank‑sum test. Categorical variables were compared using the χ2 test or Fisher exact test, as appropriate. When significant associations were detected between FMD and other variables, odds ratios (ORs) with 95% CIs were calculated. A 2‑tailed P value below 0.05 was considered significant. The statistical analyses were performed with SAS package, version 9.4 (SAS Institute Inc., Cary, North Carolina, United States).
Results
The study population included 109 patients. Mean (SD) age of the entire cohort was 44.6 (9.3) years, with a majority being women (97.2%). Baseline characteristics of the population are summarized in Table 1.
Parameter | Value | |
Data are presented as number (percentage) or median (interquartile range) unless indicated otherwise.
Abbreviations: EVA, extracoronary vascular abnormality; FMD, fibromuscular dysplasia; LDL, low‑density lipoprotein; SCAD spontaneous coronary artery dissection | ||
Age, y, mean (SD) | 44.6 (9.3) | |
Women | 106 (97.2) | |
Comorbidities and cardiac risk factors | ||
Hypertension | 38 (34.9) | |
Diabetes mellitus | 7 (6.4) | |
Dyslipidemia | 20 (18.3) | |
Hyperthyroidism | 5 (4.6) | |
Hypothyroidism | 17 (15.6) | |
Smoking | 41 (37.6) | |
Migraines | 42 (38.5) | |
Pregnancy‑associated SCAD (n = 106) | 9 (8.26) | |
Family history | ||
SCAD | 1 (0.9) | |
Noncoronary artery dissection | 0 | |
Aneurysms | 5 (4.9) | |
FMD | 0 | |
Acute coronary syndrome <65 y | 23 (22.5) | |
Connective tissue disease | 2 (2) | |
EVAs | ||
Overall | 52 (47.7) | |
FMD | Total | 35 (32.1) |
Multifocal | 30 (85.7) | |
Focal | 5 (14.3) | |
Localization of FMD | Renal arteries | 22 (20.3) |
Cervical FMD | 17 (15.6) | |
Multisite FMD | 9 (8.3) | |
Aneurysms | Total | 25 (23.2) |
Renal | 8 (7.3) | |
Intracerebral | 7 (6.4) | |
Splenic | 8 (7.3) | |
Cervical | 6 (5.5) | |
Aneurysm in more than 1 vascular bed | 5 (4.6) | |
FMD‑related | 10 (40) | |
Isolated | 15 (60) | |
Dissection of cervical arteries | 6 (5.5) | |
Coexisting FMD and aneurysms | 10 (9.3) | |
Coexisting FMD and dissection of cervical arteries | 4 (3.7) | |
Coexisting aneurysms and dissection of cervical arteries | 3 (2.8) | |
Coexisting FMD, aneurysms, and dissection of cervical arteries | 3 (2.8) | |
SCAD type | ||
1 | 11 (10.1) | |
2a | 54 (49.6) | |
2b | 17 (15.6) | |
3 | 10 (9.2) | |
4 | 22 (20.2) | |
SCAD localization | ||
Right coronary artery | 22 (20.4) | |
Left anterior descending artery | 61 (56.5) | |
Circumflex artery | 39 (36.4) | |
Left main artery | 11 (10.2) | |
Laboratory findings | ||
Troponin T, ng/l | 350 (55–1056) | |
Creatine kinase‑MB, ng/ml | 15 (4–47) | |
C‑reactive protein, mg/l | 1.61 (0.6–4.7) | |
LDL cholesterol, mmol/l | 2.91 (2.31–3.47) | |
EVAs were present in 47.7% of the cohort. FMD was identified in 32.1% of the patients. The renal (20.3%) and cervical (15.6%) arteries were the most frequently affected vascular beds. Multifocal FMD was observed more frequently than focal FMD (27.5% vs 4.6%). FMD in more than 1 vascular bed (multisite FMD) was present in 8.3% of the patients.
Aneurysms were identified in 23.2% of the cohort, predominantly involving renal and splenic arteries (7.3% each) and intracerebral arteries (6.4%), with cervical arteries slightly less affected (5.5%). Among 25 aneurysms, 10 (40%) were FMD‑related and 15 (60%) were isolated. Aneurysms in more than 1 vascular territory were observed in 4.6% of the patients.
Cervical dissections were detected in 5.5% of the cohort.
A minority of patients (9.3%) had both FMD and aneurysms, while 2.8% had FMD, aneurysm, and cervical dissection simultaneously.
Migraines were reported by 58.8% of the patients with cervical FMD. All patients with aneurysms were asymptomatic. However, 3 individuals with intracerebral aneurysms (12%) required intravascular treatment due to a high risk of rupture. Cervical dissections were rare and equally likely to be symptomatic (headache) or silent. No patient experienced stroke or transient ischemic attack attributable to EVAs. Table 2 shows symptoms in the patients with particular types of EVAs.
Parameter | Value |
Data are presented as number of patients (percentage).
Abbreviations: see Table 1 | |
Cervical FMD (n = 17) | |
Stroke | 0 |
Migraine headaches | 10 (58.8) |
Clinically silent | 7 (41.2) |
Dissection of cervical arteries (n = 6) | |
Stroke | 0 |
Migraine headaches | 3 (50) |
Clinically silent | 3 (50) |
Aneurysms (n = 25) | |
Rupture | 0 |
Clinically silent | 25 (100) |
Requiring endovascular treatment | 3 (12) |
Treatment strategies (conservative management, percutaneous coronary intervention, and coronary artery bypass grafting) did not differ between the groups. Left ventricular ejection fraction (LVEF) at discharge was similar (52% in the EVA vs 56% in the non‑EVA group).
In the patients with FMD, type 2a SCAD was observed more often than in those without FMD (65.7% vs 43.1%; P = 0.03), whereas type 3 SCAD was less common (0% vs 13.9%; P = 0.03). The patients with type 2a SCAD had a 2.5‑fold higher likelihood of FMD (OR, 2.5; 95% CI, 1.09–5.87).
Pregnancy‑associated SCAD (P‑SCAD) occurred more often in the patients with FMD (17.6% vs 4.2%; OR, 4.9; 95% CI, 1.2–21.1; P = 0.03), and hyperthyroidism was also more frequent in the FMD group (11.4% vs 1.3%; OR, 9.4; 95% CI, 1–87.7; P = 0.04).
The analysis of coronary angiograms in the acute phase of SCAD did not show changes typical of FMD.
The only significant difference in laboratory test results, including the levels of troponin T, creatine kinase‑MB, C‑reactive protein, and low‑density lipoprotein cholesterol, was higher troponin T level in the non‑FMD than the FMD group.
When comparing the groups with and without FMD, we also evaluated the prevalence of aneurysms and cervical dissections. Notably, in the patients with FMD both these complications occurred more frequently than in the group without FMD (aneurysms, 28.6% vs 20.5%; dissections, 11.4% vs 2.7%). However, the results did not reach significance.
Additionally, while comparing the subgroups of the patients with FMD and concomitant aneurysm or dissection and the patients with FMD alone, we observed higher LVEF in the individuals with FMD and other abnormalities than those with FMD alone (60% vs 51%; P = 0.04).
There were no significant differences between the groups of patients with and without aneurysms.
The comparison of EVA and non‑EVA patients is shown in Table 3, while particular subgroups are analyzed in Tables 4 and 5.
Patient characteristic | EVA group
(n = 52; 47.7%) | Non‑EVA group
(n = 57; 52.3%) | P value |
Data are presented as number (percentage) or median (interquartile range).
Abbreviations: ACEI, angiotensin‑converting enzyme inhibitor; ARB, angiotensin II receptor blocker; CABG, coronary artery bypass grafting; LVEF, left ventricular ejection fraction; NSTEMI, non–ST‑segment elevation myocardial infarction; PCI, percutaneous coronary intervention; POBA, plain old balloon angioplasty; P‑SCAD, pregnancy‑associated spontaneous coronary artery dissection; STEMI, ST‑segment elevation myocardial infarction; others, see Table 1 | |||
Comorbidities and cardiac risk factors | |||
Hypertension | 17 (32.7) | 21 (36.8) | 0.65 |
Diabetes mellitus | 1 (1.9) | 6 (10.5) | 0.12 |
Dyslipidemia | 11 (21.1) | 9 (15.8) | 0.47 |
Hyperthyroidism | 4 (7.7) | 1 (1.7) | 0.19 |
Hypothyroidism | 5 (9.6) | 12 (21) | 0.1 |
Smoking | 20 (38.5) | 21 (36.8) | 0.86 |
P‑SCAD | 7/51 (13.7) | 2/55 (3.6) | 0.08 |
STEMI | 26 (52) | 19 (35.8) | 0.1 |
NSTEMI | 25 (50) | 35 (66) | 0.1 |
SCAD type | |||
1 | 5 (9.8) | 6 (10.7) | 0.88 |
2a | 28 (54.9) | 26 (46.4) | 0.38 |
2b | 9 (17.6) | 8 (14.3) | 0.63 |
3 | 3 (5.9) | 7 (12.5) | 0.32 |
4 | 9 (17.6) | 13 (23.2) | 0.48 |
Laboratory findings | |||
Troponin T, ng/l | 228.5 (36–1008) | 533.5 (113–1191) | 0.14 |
Troponin T max, ng/l | 1377 (614–7666) | 1234 (533–3760) | 0.52 |
Creatine kinase‑MB, ng/ml | 16.7 (4–56.1) | 13.7 (3.1–35.9) | 0.29 |
C‑reactive protein, mg/l | 1.3 (0.6–4.35) | 1.75 (0.5–5) | 0.86 |
LDL cholesterol, mmol/l | 2.9 (2.12–3.47) | 2.93 (2.43–3.47) | 0.46 |
Treatment methods | |||
Conservative management | 27 (51.9) | 37 (64.9) | 0.17 |
PCI | 21 (40.4) | 18 (31.6) | 0.34 |
POBA | 1 (1.9) | 1 (1.75) | >0.99 |
CABG | 3 (5.8) | 1 (1.75) | 0.35 |
LVEF at discharge, % | 52 (45–60) | 56 (50–60) | 0.19 |
Pharmacologic treatment | |||
β-Blocker | 42 (80.8) | 45 (78.9) | 0.81 |
ACEI/ARB | 27 (51.9) | 36 (63.2) | 0.23 |
Flozin | 1 (1.9) | 2 (3.5) | >0.99 |
Statin | 39 (75) | 45 (78.9) | >0.99 |
Aspirin | 52 (100) | 57 (100) | >0.99 |
Clopidogrel | 28 (53.8) | 34 (59.6) | 0.54 |
Ticagrelor | 23 (44.2) | 16 (28.1) | 0.08 |
Patient characteristic | FMD group
(n = 35; 32.1%) | Non‑FMD group
(n = 74; 67.9%) | P value |
Data are presented as number (percentage) or median (interquartile range).
| |||
Comorbidities and cardiac risk factors | |||
Hypertension | 14 (40) | 24 (32.4) | 0.4 |
Diabetes mellitus | 1 (2.9) | 6 (8.1) | 0.43 |
Dyslipidemia | 8 (22.9) | 12 (16.2) | 0.4 |
Hyperthyroidism | 4 (11.4) | 1 (1.3) | 0.04 |
Hypothyroidism | 3 (8.6) | 14 (18.9) | 0.16 |
Smoking | 13 (37.1) | 28 (37.8) | 0.94 |
P‑SCAD | 6/34 (17.6) | 3/72 (4.2) | 0.03 |
SCAD type | |||
1 | 4 (11.4) | 7 (9.7) | 0.75 |
2a | 23 (65.7) | 31 (43.1) | 0.03 |
2b | 6 (17.1) | 11 (15.3) | 0.8 |
3 | 0 | 10 (13.9) | 0.03 |
4 | 5 (14.3) | 17 (23.6) | 0.26 |
Laboratory findings | |||
Troponin T, ng/l | 154 (19–519) | 555 (124–1191) | 0.01 |
Troponin T max, ng/l | 1143 (488–2272) | 1314 (619–6661) | 0.43 |
Creatine kinase‑MB, ng/ml | 24 (10.6–56.1) | 13.0 (3.1–36) | 0.09 |
C‑reactive protein, mg/l | 1.89 (0.65–4) | 1.51 (0.5–5) | 0.86 |
LDL cholesterol, mmol/l | 2.87 (1.94–3.34) | 2.93 (2.43–3.47) | 0.35 |
Treatment methods | |||
Conservative management | 16 (45.7) | 48 (64.9) | 0.06 |
PCI | 15 (42.8) | 24 (32.4) | 0.29 |
POBA | 1 (2.9) | 1 (1.35) | 0.54 |
CABG | 3 (8.6) | 1 (1.35) | 0.1 |
LVEF at discharge, % | 55 (45–60) | 55 (48–60) | 0.4 |
Pharmacologic treatment | |||
β-Blocker | 27 (77.1) | 60 (81.1) | 0.63 |
ACEI/ARB | 19 (54.3) | 44 (59.5) | 0.61 |
Flozin | 0 | 3 (4) | 0.55 |
Statin | 25 (71.4) | 59 (79.7) | 0.34 |
Aspirin | 35 (100) | 74 (100) | >0.99 |
Clopidogrel | 18 (51.4) | 44 (59.8) | 0.43 |
Ticagrelor | 14 (40) | 25 (33.8) | 0.53 |
FMD‑related complications | |||
Aneurysms | 10 (28.6) | 15 (20.5) | 0.36 |
Dissection of the cervical arteries | 4 (11.4) | 2 (2.7) | 0.08 |
Patient characteristic | Aneurysm (n = 25; 22.9%) | No aneurysm (n = 84; 77.1%) | P value |
Data are presented as number (percentage) or median (interquartile range).
| |||
Comorbidities and cardiac risk factors | |||
Hypertension | 7 (28) | 31 (36.9) | 0.41 |
Diabetes mellitus | 0 | 7 (8.3) | 0.35 |
Dyslipidemia | 5 (20) | 15 (17.9) | 0.78 |
Hyperthyroidism | 0 | 5 (6) | 0.59 |
Hypothyroidism | 3 (12) | 14 (16.7) | 0.76 |
Smoking | 11 (44) | 30 (35.7) | 0.45 |
P‑SCAD | 2/25 (8) | 7/81 (8.6) | >0.99 |
SCAD type | |||
1 | 2 (8.3) | 9 (11) | >0.99 |
2a | 11 (45.8) | 43 (52.4) | 0.57 |
2b | 3 (12.5) | 14 (17.1) | 0.76 |
3 | 4 (16) | 6 (7.3) | 0.42 |
4 | 5 (20.8) | 17 (20.7) | >0.99 |
Laboratory findings | |||
Troponin T, ng/l | 347 (126–1056) | 413 (54–1083) | 0.93 |
Troponin T max, ng/l | 1179 (594–7666) | 1243 (540–4679) | 0.92 |
Creatine kinase‑MB, ng/ml | 7.3 (2.6–52.4) | 17 (4.8–44.2) | 0.35 |
C‑reactive protein, mg/l | 0.9 (0.6–3.8) | 1.9 (0.55–5) | 0.28 |
LDL cholesterol, mmol/l | 2.9 (2.38–3.21) | 2.93 (2.28–3.5) | 0.53 |
Treatment methods | |||
Conservative management | 16 (64) | 48 (57.1) | 0.54 |
PCI | 9 (36) | 30 (35.7) | 0.98 |
POBA | 0 | 2 (2.4) | >0.99 |
CABG | 0 | 4 (4.8) | 0.57 |
LVEF at discharge, % | 57 (49–60) | 55.9 (47.5–60) | 0.76 |
Pharmacologic treatment | |||
β-Blocker | 20 (80) | 67 (79.8) | 0.98 |
ACEI/ARB | 12 (48) | 51 (60.7) | 0.26 |
Flozin | 1 (4) | 2 (2.4) | 0.55 |
Statin | 21 (84) | 63 (75) | 0.35 |
Aspirin | 25 (100) | 84 (100) | >0.99 |
Clopidogrel | 15 (60) | 47 (56) | 0.72 |
Ticagrelor | 10 (40) | 29 (34.5) | 0.62 |
Discussion
Previous studies confirm that SCAD patients often have coexisting EVAs, but the reported prevalence differs depending on the study population, the number of analyzed vascular territories, various imaging modalities and protocols, and different definitions used.8-10 In our multicenter registry, nearly half of the patients had an evidence of EVAs. The most common of these arterial abnormalities was FMD, occurring in 32.1% of the SCAD patients. This finding is consistent with previous studies, where the prevalence of FMD in SCAD individuals ranged from 11% to 86%.2,4,5,8,9,11-13 In our study, FMD was most frequently present in the renal (20.3%) and cervical (15.6%) arteries. These results are comparable to the prior series, in which renal FMD occurred in 15.6%–29% of the patients, and cerebrovascular FMD in 13.3%–22%.4,11 A corresponding prevalence of FMD was noted in the largest cohort of the Canadian registry, in which 750 patients were evaluated and FMD was diagnosed in 31.1% of the overall cohort (though this constituted a higher percentage of 56.7% among those who had complete FMD screening) in the renal, cerebrovascular, and iliac / femoral arteries (27.7%, 29.5%, and 21%, respectively).14 It is of note that we assessed the type of SCAD in the study cohort and observed some differences in the distribution of different SCAD types in particular subgroups. In our cohort, type 2a SCAD was significantly more common in the FMD group, whereas type 3 SCAD occurred less frequently. Moreover, the patients with type 2a SCAD had a 2.5‑fold higher likelihood of having FMD in any extracoronary arterial bed. These results highlight the need for routine extracoronary vascular screening in SCAD patients, particularly in those with type 2a SCAD.
Our study showed that P‑SCAD occurred more often in the patients with FMD. This may be partially explained by hormonal changes. Studies acknowledge elevated level of transforming growth factor β (TGF-β) in many SCAD and FMD patients, suggesting its involvement by regulating a variety of cellular functions in the arterial wall that lead to cellular proliferation, differentiation, modulation of extracellular matrix production, and ultimately, arterial remodeling.15 TGF-β promotes increased collagen production, reducing connective tissue elasticity. Sources suggest that TGF-β activity has a negative impact on arterial tortuosity and arterial weakening, both present in SCAD and FMD.15 Such patients may be more prone to hormonal changes during pregnancy. The excess progesterone in pregnancy may cause decreased collagen synthesis, medial collagen wall degradation, and loss of elastic fiber corrugation leading to weakening of the tunica media, which may predispose to arterial dissection. Moreover, an increase in estrogen may cause a release of metalloproteinases, thus weakening the vasa vasorum, predisposing to artery dissection. Hemodynamic changes in pregnancy, such as greater blood volume, heart rate, and cardiac output increase shear forces on the arterial wall.15
Although FMD was the most common EVA identified among the SCAD patients, both in our cohort and the previously studied ones,4,11 other arterial abnormalities, including dissections and aneurysms, were also detected, even in the absence of FMD.
Other investigations indicated that concomitant EVAs were significantly more commonly detected in patients with both SCAD and FMD than in SCAD patients without FMD.1 Nevertheless, in our study, only a minority of the patients (9.3%) presented with both FMD and aneurysm. The coexistence of FMD, aneurysm, and dissection of cervical arteries was found in an even smaller group of patients (2.8%). There was a relatively high prevalence of aneurysms, both isolated and FMD‑related.
Nevertheless, the prevalence of EVAs other than FMD is less thoroughly documented. Androulakis et al1 showed that aneurysms are most commonly detected in the renal (32.9% of patients with aneurysms) and carotid (21.1%) arteries, aorta (19.7%), as well as celiac (15.8%), and cerebrovascular (11.8%) arteries. Moreover, it has been reported that the prevalence of intracerebral aneurysms in SCAD patients is significantly higher than in the general population,1 reaching between 14% and 23%.8,11 It is noteworthy that, in our analysis, the prevalence of aneurysms reached 23.2%, which was higher than in previous studies. Renal and splenic aneurysms were the most common, occurring in 7.3% of the SCAD patients, whereas intracerebral aneurysms were identified in 6.4% of the studied cohort. Aneurysms of the cervical arteries were less frequently observed, as they were present in 5.5% of the patients. Notably, the prevalence of cerebral aneurysms in our research was relatively low when compared with the majority of other studies, where it ranged between 7.1% and 22.5%.11,14,16,17 Nevertheless, in a study by Macaya et al,18 where magnetic resonance imaging was used for screening, no intracerebral aneurysms were found. The clinical relevance of detecting silent aneurysms—especially intracerebral ones—remains high. In particular, large aneurysms may prompt appropriate specialty referrals for additional evaluation and possible interventions.3,18,19 Silent aneurysms may otherwise remain undiagnosed until rupture, which carries a high morbidity and mortality risk. It is worth noting that 3 patients in our study required endovascular treatment, illustrating the importance of screening for EVAs.
In our cohort, cervical dissections were the least frequent EVA (5.5%), which is consistent with prior data suggesting that extracoronary dissections are less common than FMD or aneurysms. They were found in 1.7%–19.7% of the cases in the studied cohorts, and most frequently affected the carotid, renal, and vertebral arteries (75%, 21.6%, and 17% of patients with dissections, respectively).1,4 Notably, dissections can be symptomatic, causing headaches or neurological symptoms. Although none of our patients experienced stroke, the identification of dissections highlights the importance of neurological surveillance in SCAD survivors.
It remains to be established whether EVAs other than FMD may be the result of very subtle FMD, an underlying genetic defect, or any kind of connective tissue disease.11 Nevertheless, the broad spectrum of EVAs in SCAD patients may raise the suspicion that a systemic arterial disorder may be the underlying cause of this condition, and may lead to the assumption that SCAD is a manifestation of generalized vascular disease.
Table 6 shows the prevalence of EVAs, FMD, and aneurysms among the SCAD patients in the most important studies, including large cohorts of patients, in the last 5 years.
Author, year | Patients, n | Screened for EVA, % (n/N) | FMD among those screened, % (n/N) | EVA other than FMD among those screened, % (n/N) | Aneurysm, % (n/N) |
Abbreviations: n, number of affected patients; N, total number of patients; NR, not reported; others, see Table 1 | |||||
Clare et al, 201920 | 208 | 43.2 (90/208) | 10 (9/90) | NR | NR |
Sharma et al, 201921 | 113 | 30.1 (34/113) | 52.9 (18/34) | 100% had EVA (including FMD) | NR |
Saw et al, 201914 | 750 | 54.8 (233/411) | 56.7 (233/411) | NR | Cerebral aneurysm in 7.1 (30/424) |
Garcia‑Guimaraes et al, 202116 | 318 | 29.2 (93/318) | 25.8 (24/93) | 14 (13/93) | 8.6 (8/93) |
Inohara et al, 202122 | 346 | 100 (346/346) | 72.3 (250/346) | NR | NR |
Androulakis et al, 202223 | 144 | 52.1 (75/144) | 6.7 (5/75) | 26.7 (20/75) | NR |
Persu et al, 20224 | 173 | 100 (173/173) | 31.8 (55/173) | 9.2 (16/173) | 7.5 (13/113) |
Feldbaum et al, 202324 | 157 | 53.5 (84/157) | 63 (53/84) | NR | NR |
Visina et al, 202325 | 193 | 100 (193/193) | 50.5 (97/193) | 32.6 (63/193) | 16.6 (32/193) |
To our knowledge, this is the first study assessing not only the prevalence of EVAs, but also analyzing SCAD type and EVA‑related symptoms.
These findings strongly support the importance of comprehensive vascular imaging for detecting noncoronary abnormalities in SCAD survivors, as the identification of EVAs can influence clinical management strategies. Although coming from a retrospective analysis, the information provided by our study contributes to a deeper insight into underlying vascular pathology in SCAD. Nevertheless, further prospective studies with systematic imaging, genetic profiling, and long‑term follow‑up are warranted to clarify the prognostic and therapeutic implications of EVAs in this population, to ascertain the pathophysiological implications of this intriguing association and, finally, to demonstrate the possible causality. Prospective registries should also evaluate optimal imaging surveillance intervals and thresholds for intervention.
Limitations
This study is limited by its retrospective, observational design. Therefore, we cannot conclude whether the associations that have been documented are causative. Furthermore, in view of the moderate sample size and multiple subgroup analysis performed, some of the associations reported may be due to chance, and therefore need confirmation.
Although this registry represents one of the largest SCAD cohorts analyzed in Poland, the sample size (n = 109) remains modest, limiting statistical power. Larger, prospective, multicenter studies are needed to confirm these findings and better define their clinical implications.
Conclusions
This study demonstrated a significant prevalence and distribution of EVAs in SCAD patients, with aneurysms being more common than previously reported. The study identified EVAs in almost half of the analyzed population (47.7%). The most common EVA was FMD, affecting 32.1% of the patients, and most frequently occurring in the renal and cervical arteries. Moreover, the study showed that the patients with type 2a SCAD had a 2.5‑fold higher likelihood of having FMD. There is a notable burden of aneurysms (23.2%) in SCAD patients, mostly located in the renal, splenic, and intracerebral arteries. However, most aneurysms (60%) were not associated with concomitant FMD. All aneurysms were clinically silent.
- Androulakis E, Kourek C, Vrettos A, et al. Assessment of extra‑coronary peripheral arteriopathy in spontaneous coronary dissection: state of the art in non‑invasive imaging techniques and future perspectives. Eur Heart J Imaging Methods Pract. 2023; 1: qyad044. | Crossref
- Adlam D, Alfonso F, Maas A, et al. European Society of Cardiology, acute cardiovascular care association, SCAD study group: a position paper on spontaneous coronary artery dissection. Eur Heart J. 2018; 39: 3353‑3368. | Crossref
- Bcharah H, Bcharah G, Nabi HA, et al. Extracoronary arterial pathologies in patients with spontaneous coronary artery dissection. Am J Cardiol. 2025; 258: 151‑157. | Crossref
- Persu A, Lopez‑Sublet M, Al‑Hussaini A, et al. Prevalence and disease spectrum of extracoronary arterial abnormalities in spontaneous coronary artery dissection. JAMA Cardiol. 2022; 7: 159‑166. | Crossref
- Hayes SN, Kim ESH, Saw J, et al. Spontaneous coronary artery dissection: current state of the science: a scientific statement from the American Heart Association. Circulation. 2018; 137: e523‑e557. | Crossref
ARTICLE INFORMATION