Impact of cardiovascular-kidney-metabolic conditions on clinical outcomes in patients with atrial fibrillation: results from a prospective cohort
1 Key words: adverse events, atrial fibrillation, cardiovascular-kidney-metabolic, integrated care, left atrial remodeling
Key words: adverse events, atrial fibrillation, cardiovascular-kidney-metabolic, integrated care, left atrial remodeling

 CC BY 4.0
CC BY 4.0
Impact of cardiovascular-kidney-metabolic conditions on clinical outcomes in patients with atrial fibrillation: results from a prospective cohort
Introduction: Cardiovascular‑kidney‑metabolic (CKM) conditions are frequently encountered in clinical practice.
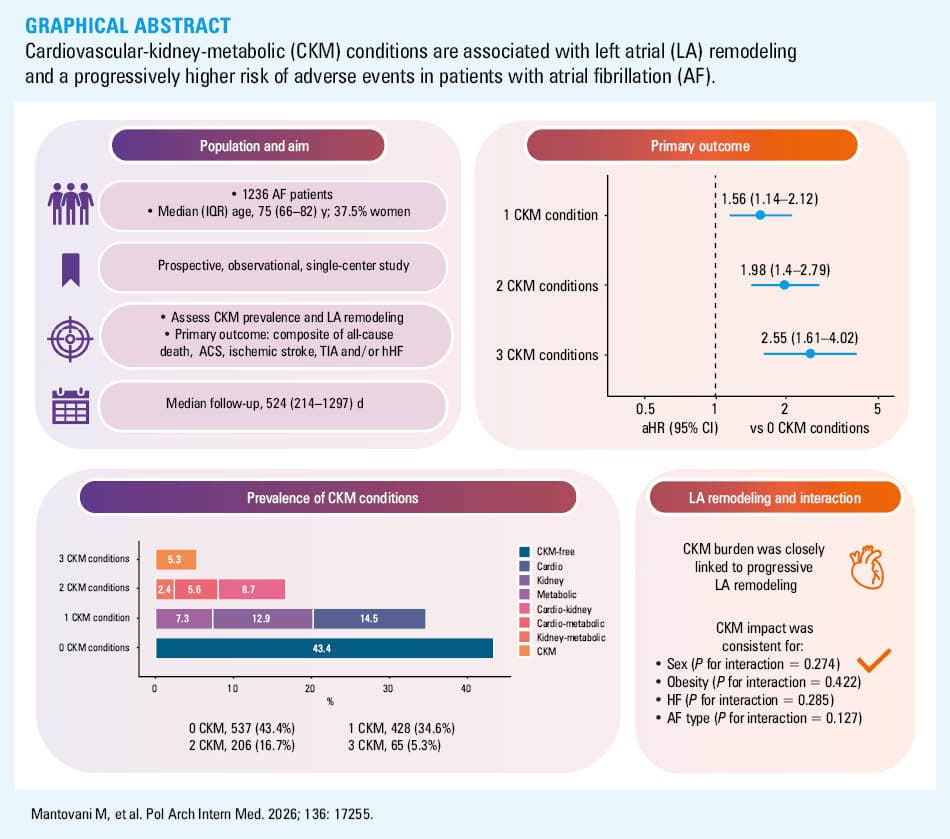
Objectives: Our aim was to evaluate the epidemiology and impact of CKM conditions in patients with atrial fibrillation (AF), with a focus on their association with left atrial (LA) remodeling and clinical outcomes.
Patients and methods: Patients with AF enrolled in this single‑center prospective study were stratified based on the presence of CKM comorbidities. We assessed the relationship between CKM status, LA remodeling, and adverse clinical outcomes. The primary outcome was a composite of all‑cause death, acute coronary syndrome, ischemic stroke and transient ischemic attack, and hospitalization for heart failure.
Results: A total of 1236 patients at a median (interquartile range) age of 75 (66–82) years (37.5% women) were included. Among them, 43.4% had no CKM conditions, 34.6% had 1 CKM condition, 16.7% had 2 CKM conditions, and 5.3% had 3 CKM conditions. LA remodeling was progressively more pronounced with increasing CKM burden. After median follow‑up of 524 (217–1297) days, 283 events of the primary outcome (27.5%) were reported. As compared with the patients with 0 CKM conditions, there was a progressively higher risk of adverse events in the patients with 1 CKM condition (adjusted hazard ratio [aHR], 1.56; 95% CI, 1.14–2.12), 2 CKM conditions (aHR, 1.98; 95% CI, 1.4–2.79), and 3 CKM conditions (aHR, 2.55; 95% CI, 1.61–4.02). The impact of the CKM status was consistent irrespective of sex, obesity, and AF type.
Conclusions: CKM multimorbidity is highly prevalent in AF patients, where it is associated with progressive LA remodeling and a stepwise increase in the risk of adverse events.
What's new?
Atrial fibrillation (AF) often occurs together with other long‑term conditions, affecting the cardiovascular system, kidneys, and metabolism. However, the impact of these combinations on patient health and prognosis is not fully known. In our study of over 1200 AF patients, more than half had at least 1 cardiovascular, kidney, or metabolic (CKM) condition. Notably, there was a clear association between the burden of CKM conditions and progressive left atrial remodeling. Furthermore, increasing CKM burden was associated with a stepwise higher risk of major adverse events, including death, heart failure hospitalization, and stroke. This association remained consistent regardless of age, sex, obesity, or AF type, highlighting the importance of integrated and holistic care across cardiovascular, renal, and metabolic dimensions.
Introduction
Atrial fibrillation (AF) is the most common cardiac arrhythmia globally, with its prevalence and incidence projected to substantially rise in the coming decades.1-3
AF is associated with an increased risk of mortality and adverse cardiovascular outcomes, representing a major public health and clinical challenge.4-7 Notably, AF rarely occurs in isolation, and is often accompanied by a wide spectrum of cardiac and noncardiac comorbidities, which tend to cluster in specific patterns.8-11 Among these, increasing attention has been directed toward the cardiovascular‑kidney‑metabolic (CKM) axis, as these conditions commonly co‑occur and interact.12 A recent American Heart Association (AHA) consensus document defined CKM syndrome as a complex interplay of interrelated diseases that progress through distinct stages and may ultimately culminate in overt multiorgan dysfunction.13 While the individual effects of each comorbidity on outcomes in AF patients have been previously reported, their combined impact—particularly in the form of CKM multimorbidity—remains poorly understood.
Emerging evidence also suggests that AF may serve not only as a risk factor but also as a clinical marker of advanced systemic disease and CKM multimorbidity.13 In this context, elucidating the relationship between CKM conditions and AF may offer novel insights into the pathophysiological mechanisms of disease progression and patient stratification.
Additionally, while AF is well known to be associated with atrial remodeling, and CKM conditions are also thought to impair left atrial (LA) structure and function, the effect of CKM multimorbidity on atrial remodeling in AF patients is yet to be fully explored.14-17
Therefore, the aim of this study was to investigate the prevalence and impact of CKM conditions on LA remodeling and on the risk of adverse cardiovascular events in patients with AF.
Patients and methods
Study design and definitions
We included AF patients prospectively enrolled in a single‑center observational study held at the Cardiology Division of the tertiary care University Hospital in Modena. Both inpatients and outpatients aged at least 18 years, who had electrocardiographic documentation of AF within the previous year, and provided a written informed consent were enrolled between January 2016 and August 2024. At enrollment, investigators collected data on medical history, laboratory findings, and ongoing pharmacologic treatment. The study protocol was approved by the local Ethics Committee (Comitato Etivo Area Vasta Emilia Nord ‑ AVEN) (237/16), and the study was performed in accordance with the European Union Note for Guidance on Good Clinical Practice (CPMP/ECH/135/95) and the 2013 Declaration of Helsinki.
For the purpose of this analysis, the cohort was stratified according to CKM status based on the number and type of comorbid CKM conditions at baseline, as previously described.18 The following conditions were identified: 1) cardiovascular: defined as a history of at least 1 event of myocardial infarction, percutaneous coronary intervention, coronary artery bypass grafting, ischemic stroke, peripheral artery disease, and / or peripheral arterial revascularization; 2) kidney: chronic kidney disease (CKD) was defined as an estimated glomerular filtration rate (eGFR) below 60 ml/min/1.73 m2, calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD‑EPI) equation and the Cockcroft–Gault formulas; 3) metabolic: documented specialist diagnosis of type 2 diabetes or glycated hemoglobin level of 6.5% (48 mmol/mol) or higher, irrespective of glucose‑lowering therapy. Pharmacologic treatment alone was not used as a diagnostic criterion, as alternative indications for the prescription of some of these drugs might be present.
The patients were stratified both by number and phenotypic combinations of CKM conditions. Specifically, 0 CKM conditions meant that none of the above comorbidities were present; 1 CKM condition meant the presence of only 1 of the cardiovascular, kidney, or metabolic conditions; 2 CKM conditions indicated the presence of 2 conditions (cardiovascular‑kidney, cardiovascular‑metabolic, or kidney‑metabolic); and 3 CKM conditions meant that all 3 types of comorbidities were present.
The stratification by phenotype was defined as follows as the presence of a single condition or various possible combinations of the conditions: CKM‑free phenotype, cardiovascular only, kidney only, metabolic only, cardiovascular‑kidney, cardiovascular‑metabolic, kidney‑metabolic, or cardiovascular‑kidney‑metabolic phenotypes.
Furthermore, we performed several sensitivity analyses: 1) including chronic heart failure (HF) in the definition of cardiovascular condition; 2) excluding ischemic stroke from the definition of cardiovascular condition; 3) including obesity in the definition of metabolic condition.
The diagnosis and pattern of AF, as well as CHA2DS2-VASc, CHA2DS2-VA, and HAS‑BLED scores were assessed according to the 2020 and 2024 European Society of Cardiology guidelines.19-21
For the purpose of this analysis, all patients with available baseline data concerning CKM status were included.
Pharmacologic treatments
Baseline pharmacologic treatment was recorded, including prescription for oral anticoagulants (OACs), antiplatelet therapy, and other cardiovascular medications. Detailed data were available for β-blockers, calcium channel blockers, digoxin, class IC and III antiarrhythmic drugs (AADs), angiotensin‑converting enzyme inhibitors, angiotensin receptor blockers, angiotensin receptor‑neprilysin inhibitors, mineralocorticoid receptor antagonists (MRAs), and sodium‑glucose cotransporter 2 inhibitors (SGLT2is). Data were also collected on the use of metformin, insulin, and statins.
Assessment of left atrial echocardiographic parameters
In a subset of 569 patients, transthoracic echocardiography with LA assessment was performed at our echocardiography laboratory using commercially available ultrasound systems. All measurements were obtained from 3 different cardiac cycles for patients in sinus rhythm and from 5 consecutive beats for patients in AF. Final values were averaged and then indexed to body surface area (BSA), when appropriate.
Indexed LA volume (LAVi) was measured using the biplane Simpson method from apical 4- and 2‑chamber views, and categorized as normal (≤34 ml/m2), mildly dilated (35–41 ml/m2), moderately dilated (42–48 ml/m2), and severely dilated (≥48 ml/m2).22 Indexed LA anteroposterior diameter was measured in B‑mode, in parasternal long‑axis view, at end‑systole (end of the QRS in the electrocardiographic trace), when its dimension is maximal, using the inner‑to‑inner edge technique, and then indexed to BSA. LA ejection fraction was calculated using the formula: ([maximum volume – minimum volume] / maximum volume) × 100.23
Left ventricular end‑diastolic diameter was measured in the parasternal long‑axis view as per current guideline,22 and left ventricular ejection fraction (LVEF) was calculated using the Simpson rule.
Overall, good reproducibility for echocardiographic measures has been previously reported for our echocardiography laboratory.24
Follow‑up and adverse events
Clinical follow‑up was conducted by site investigators through in‑person visits or phone contact with the patients or caregivers. Follow‑up was scheduled at 6 months, 1 year, and annually thereafter.
The primary end point was a composite of all‑cause death, acute coronary syndromes (ACS), ischemic stroke and / or transient ischemic attack (TIA), and hospitalization for HF (hHF). The secondary exploratory end points included individual components of the primary outcome.
Statistical analysis
Continuous variables are reported as median and interquartile range (IQR) and were compared using the Kruskal–Wallis test. Categorical variables are expressed as numbers and percentages and were compared using the χ2 test.
The incidence rates (IRs) for the primary and secondary end points were calculated as the number of events per 100 person‑year with corresponding 95% CIs. The Kaplan–Meier survival curves were built to show the differences in the survival rates across CKM subgroups, and were statistically tested using the log‑rank test. The Cox proportional hazards models were used to evaluate the association between the CKM status and the risk of the primary and secondary exploratory end points. The adjusted model included age, sex, hypertension, HF, type of AF, and use of OAC as covariates. Moreover, we built several differently adjusted Cox regression models, including among covariates LAVi, AF duration, medical treatment (OACs, antiplatelet therapy, MRAs, AADs, statins, and SGLT2is), and CKD stages. We tested the proportional hazard assumption using the Schoenfeld residuals, and no critical violation was found. For the secondary exploratory outcomes of ACS/stroke/TIA, and hHF, we also performed a Fine–Gray competing risk analysis to account for the possibility of death as a competing event.
Subgroup analyses as interaction analyses were performed to explore potential effect modification by key clinical characteristics (eg, HF, obesity), with the CKM status dichotomized as 0–1 vs 2–3 conditions.
Additionally, interaction analyses were conducted using restricted cubic spline curves with 3 knots to assess the continuous, nonlinear associations of age, body mass index (BMI), and LAVi with the primary end point, stratified by the CKM status (dichotomized as 0–1 vs 2–3 conditions). Reference values used for interpretation were 75 years for age, 30 kg/m2 for BMI, and 34 ml/m2 for LAVi. All results are reported as hazard ratio (HR) and 95% CI. For the competing risk analysis, the results are shown as subdistribution HR (sHR) and 95% CI. A 2‑sided P value below 0.05 was considered significant. All analyses were performed using the R software, version 4.3.2 for Mac operating system (R Foundation for Statistical Computing, Vienna, Austria).
Results
Study population
The study included 1236 patients with AF, at a median (IQR) age of 75 (66–82) years, 37.5% of whom were women. The study flowchart is shown in Supplementary material, Figure S1. Overall, 43.4% of the cohort had no CKM conditions, 34.6% had 1 CKM condition associated with AF, 16.7% had 2, and 5.3% had all 3 CKM conditions. Baseline characteristics of the overall cohort and groups stratified according to the CKM status are detailed in Table 1, while the characteristics of the patients stratified according to specific CKM phenotypes are summarized in Supplementary material, Table S1. Among the various phenotypes, the cardiovascular component was the most prevalent (34.1% of the total cohort), with 14.5% of the patients presenting with the cardiovascular‑only phenotype (Figure 1).
Parameter | Overall | 0 CKM conditions | 1 CKM condition | 2 CKM conditions | 3 CKM conditions | P value | |
Data are presented as number (percentage) or median (interquartile range).
Abbreviations: AF, atrial fibrillation; BMI, body mass index; CAD, coronary artery disease; CG, Cockcroft–Gault formula; CKD, chronic kidney disease; CKD‑EPI, Chronic Kidney Disease Epidemiology Collaboration equation; CKM, cardiovascular‑kidney‑metabolic; COPD, chronic obstructive pulmonary disease; eGFR, estimated glomerular filtration rate; HF, heart failure; PAD, peripheral artery disease | |||||||
All patients | 1236 (100) | 537 (43.4) | 428 (34.6) | 206 (16.7) | 65 (5.3) | – | |
Women | 463 (37.5) | 198 (36.9) | 169 (39.5) | 76 (36.9) | 20 (30.8) | 0.55 | |
Age, y | 75 (66–82) | 69 (59–76) | 77 (71–83) | 80 (74–84) | 78 (72–83) | <0.001 | |
Hypertension | 913 (73.9) | 325 (60.5) | 352 (82.2) | 178 (86.4) | 58 (89.2) | <0.001 | |
Dyslipidemia | 650 (52.6) | 216 (40.3) | 250 (58.4) | 141 (68.4) | 43 (66.2) | <0.001 | |
Type 2 diabetes | 254 (20.6) | 0 | 90 (21) | 99 (48.1) | 65 (100) | <0.001 | |
Obesity | 281 (23.2) | 120 (22.7) | 100 (23.7) | 39 (19.6) | 22 (34.9) | 0.09 | |
BMI, kg/m2 | 26.2 (23.11–29.67) | 26 (22.79–29.63) | 26.56 (23.13–29.69) | 25.8 (22.9–29.36) | 27.1 (24.16–31.21) | 0.17 | |
Active smoking | 124 (10) | 70 (13.1) | 35 (8.2) | 13 (6.3) | 6 (9.2) | 0.02 | |
CAD | 318 (25.7) | 0 | 125 (29.2) | 139 (67.5) | 54 (83.1) | <0.001 | |
HF | 371 (30) | 107 (19.9) | 131 (30.6) | 95 (46.1) | 38 (58.5) | <0.001 | |
PAD | 136 (11) | 0 | 60 (14) | 52 (25.2) | 24 (36.9) | <0.001 | |
CKD | 361 (29.2) | 0 | 159 (37.1) | 137 (66.5) | 65 (100) | <0.001 | |
eGFR (CG), ml/min/1.73 m2 | 68.01 (49.39–91.71) | 83.97 (65.19–106.51) | 61.43 (46.64–83.4) | 48.75 (37.97–62.76) | 40.6 (36.71–55.9) | <0.001 | |
eGFR (CKD‑EPI), ml/min/1.73 m2 | 70 (59–85) | 82 (69–92) | 62 (58–81) | 57 (42–61) | 43 (32–50) | <0.001 | |
Ischemic stroke | 65 (5.3) | 0 | 31 (7.3) | 24 (11.7) | 10 (15.4) | <0.001 | |
Previous bleeding | 119 (9.6) | 34 (6.3) | 47 (11) | 26 (12.6) | 12 (18.5) | 0.001 | |
Anemia | 308 (25.5) | 81 (15.6) | 107 (25.4) | 86 (42.8) | 34 (53.1) | <0.001 | |
Liver disease | 40 (3.2) | 14 (2.6) | 17 (4) | 7 (3.4) | 2 (3.1) | 0.7 | |
COPD | 102 (8.3) | 29 (5.4) | 39 (9.1) | 23 (11.2) | 11 (16.9) | 0.002 | |
CHA2DS2-VA score, points | 3 (2–4) | 2 (1–3) | 4 (3–4) | 5 (4–5) | 6 (5–6) | <0.001 | |
CHA2DS2-VASc score, points | 4 (2–5) | 2 (1–3) | 4 (3–5) | 5 (4–6) | 6 (5–7) | <0.001 | |
HAS‑BLED score, points | 1 (1–2) | 1 (0–1) | 1 (1–2) | 2 (1–3) | 3 (2–3) | <0.001 | |
AF type | Paroxysmal | 273 (22.1) | 141 (26.3) | 86 (20.1) | 32 (15.5) | 14 (21.5) | <0.001 |
Persistent | 273 (22.1) | 143 (26.6) | 93 (21.7) | 34 (16.5) | 3 (4.6) | ||
Permanent | 514 (41.6) | 165 (30.7) | 204 (47.7) | 109 (52.9) | 36 (55.4) | ||
First diagnosed | 176 (14.2) | 88 (16.4) | 45 (10.5) | 31 (15) | 12 (18.5) | ||
AF ablation | 54 (4.4) | 39 (7.3) | 12 (2.8) | 3 (1.5) | 0 | <0.001 | |

The patients with 0 CKM conditions were younger, with a lower prevalence of dyslipidemia, hypertension, HF, as well as previous bleeding and chronic obstructive pulmonary disease (COPD). These comorbidities progressively increased with higher CKM burden along with CHA2DS2-VA, CHA2DS2-VASc, and HAS‑BLED scores (Table 1).
Pharmacologic treatment
As shown in Supplementary material, Table S2, the prescription for OAC was overall high (92.1%), despite lower rates in the patients with 0 and 3 CKM conditions (87.7% and 86.2%, respectively). Conversely, antiplatelet therapy use was markedly higher among the individuals with 3 CKM conditions (50.8% vs 3.7% in the patients with no CKM conditions). The use of AADs was more common in the patients without CKM conditions (16.6%), and progressively decreased with increasing CKM burden. Treatments stratified based on CKM phenotypes are detailed in Supplementary material, Table S3.
Left atrial echocardiographic parameters
Echocardiographic data were analyzed in a subset of 569 patients (median age, 74 [66–81] y; 38.3% women) with available parameters. There were no significant differences in sex, median age, or median CHA2DS2-VASc score between the patients included and those excluded from this analysis (all P >0.05). Overall, 35.3% of the patients did not exhibit LA dilation. As reported in Table 2, significant differences in LA morphology were observed across CKM groups. The proportion of patients with LA dilation progressively increased in parallel with higher CKM burden. Specifically, the prevalence of severe LA dilation increased from 24.2% in the individuals with no CKM conditions up to 40% and 40.5% in the patients with 2 or 3 CKM conditions, respectively.
Parameter | Overall | 0 CKM conditions | 1 CKM condition | 2 CKM conditions | 3 CKM conditions | P value | |
Data are presented as number (percentage) or median (interquartile range).
Abbreviations: iLAAPD, indexed left atrial antero‑posterior diameter; LA, left atrium; LAEF, left atrial ejection fraction; LAVi, left atrial volume index; LVEDD, left ventricular end‑diastolic diameter; LVEF, left ventricular ejection fraction; others, see Table 1 | |||||||
Patients | 569 (100) | 248 (43.6) | 184 (32.3) | 100 (17.6) | 37 (6.5) | – | |
LVEF, % | 55 (45–60) | 59 (54–60) | 55 (45–60) | 50 (38–60) | 43 (38–56) | <0.001 | |
LVEDD, mm | 52 (47–58) | 51 (46–55) | 51 (47–58) | 54 (46–62) | 55 (47–58) | 0.18 | |
LA dilation | No | 201 (35.3) | 112 (45.2) | 58 (31.5) | 23 (23) | 8 (21.6) | 0.003 |
Mild | 101 (17.8) | 41 (16.5) | 30 (16.3) | 21 (21) | 9 (24.3) | ||
Moderate | 86 (15.1) | 35 (14.1) | 30 (16.3) | 16 (16) | 5 (13.5) | ||
Severe | 181 (31.8) | 60 (24.2) | 66 (35.9) | 40 (40) | 15 (40.5) | ||
LAVi, ml/m2 | 40 (29–51) | 36 (26–48) | 42 (30–53) | 43 (35–54) | 44 (36–54) | <0.001 | |
iLAAPD, mm | 21 (18–24) | 20 (17–23) | 21 (18–24) | 22 (19–25) | 23 (20–24) | 0.002 | |
LAEF, % | 35 (24–48) | 37 (27–51) | 34 (23–44) | 31 (22–44) | 36 (22–50) | 0.02 | |
Echocardiographic parameters stratified by CKM phenotypes are reported in Supplementary material, Table S4.
Risk of adverse events
A total of 1030 patients (83.3% of the original cohort; median age, 75 [66–81] y; 37.8% women) with available follow‑up information were included in the survival analysis. No significant differences were observed between the patients with and without follow‑up, concerning age, sex, and CHA2DS2-VA score. During median follow‑up of 524 (214–1297) days, 283 events of the primary composite outcome (27.5%) were reported. Detailed event rates, IRs, and Cox regression results are reported in Table 3, while Figure 2 shows the Kaplan–Meier curves for the primary composite outcomes according to the CKM status.
Parameter | Events, n (%) | IR (95% CI) per 100 person‑years | HR (95% CI) | aHRa (95% CI) |
a Adjusted for age, sex, hypertension, HF, type of AF, and use of OAC
b Composite outcome of all‑cause death, ACS/ischemic stroke/TIA, and hospitalization for HF
c Fine–Gray competing risk analysis for the relationship between the CKM status and ACS/stroke/TIA and hospitalization for HF; subdistribution unadjusted and adjusted HRs are reported for these outcomes
Abbreviations: ACS, acute coronary syndrome; aHR, adjusted hazard ratio; HF, heart failure; IR, incidence rate; OAC, oral anticoagulation; TIA, transient ischemic attack; others, see Table 1 | ||||
Composite outcomeb | 283 (27.5) | – | – | – |
0 CKM conditions | 79 (17.3) | 6.35 (4.95–7.75) | Ref | Ref |
1 CKM condition | 103 (29.3) | 13 (10.5–15.5) | 2.04 (1.52–2.73) | 1.56 (1.14–2.12) |
2 CKM conditions | 73 (44.2) | 21.1 (16.3–25.9) | 3.3 (2.4–4.55) | 1.98 (1.4–2.79) |
3 CKM conditions | 28 (49.1) | 27.8 (17.5–38.1) | 4.32 (2.8–6.66) | 2.55 (1.61–4.02) |
All‑cause death | 171 (16.6) | – | – | – |
0 CKM conditions | 41 (9) | 3 (2.08–3.91) | Ref | Ref |
1 CKM condition | 62 (17.6) | 6.39 (4.8–7.98) | 2.14 (1.44–3.17) | 1.44 (0.95–2.18) |
2 CKM conditions | 53 (32.1) | 12.8 (9.39–16.3) | 4.33 (2.88–6.51) | 2.17 (1.41–3.34) |
3 CKM conditions | 15 (26.3) | 9.93 (4.91–15) | 3.33 (1.84–6.02) | 1.77 (0.95–3.28) |
ACS/ischemic stroke/TIAc | 90 (8.8) | – | – | – |
0 CKM conditions | 25 (5.5) | 1.95 (1.18–2.71) | Ref | Ref |
1 CKM condition | 39 (11.1) | 3.04 (2.16–4.15) | 2.2 (1.34–3.6) | 2.4 (1.37–4.23) |
2 CKM conditions | 15 (9.1) | 3.98 (1.96–5.99) | 1.62 (0.86–3.06) | 1.81 (0.87–3.78) |
3 CKM conditions | 11 (19.3) | 9.27 (3.79–14.7) | 3.98 (1.86–8.54) | 4.12 (1.84–9.23) |
Hospitalization for HFc | 110 (10.7) | – | – | – |
0 CKM conditions | 26 (5.7) | 1.99 (1.23–2.76) | Ref | Ref |
1 CKM condition | 40 (11.4) | 4.60 (3.18–6.03) | 2.17 (1.33–3.55) | 1.55 (0.91–2.64) |
2 CKM conditions | 29 (17.8) | 8.10 (5.23–11.63) | 3.37 (1.98–5.75) | 1.6 (0.86–2.96) |
3 CKM conditions | 15 (26.3) | 11.8 (5.82–17.7) | 5.31 (2.88–9.76) | 2.54 (1.28–5.06) |

A progressively increasing risk of adverse outcomes was observed with higher CKM burden, even after multivariable adjustment (Table 3). Specifically, as compared with the patients without CKM conditions, those with 1 CKM condition had by 56% higher risk (aHR, 1.56; 95% CI, 1.14–2.12), those with 2 CKM conditions had nearly a 2‑fold higher risk (aHR, 1.98; 95% CI, 1.4–2.79), and those with 3 CKM conditions had more than double risk (aHR, 2.55; 95% CI, 1.61–4.02) of experiencing the primary composite end point.
Regarding secondary exploratory outcomes, unadjusted analyses showed a higher risk of death across all CKM groups, while this association remained significant only for the patients with 2 CKM conditions after multivariable adjustment (aHR, 2.17; 95% CI, 1.41–3.34).
Using the Fine–Gray competing risk analysis to account for the competing risk of death, a significant association was found between the highest CKM burden and the risk of hHF (sHR, 2.54; 95% CI, 1.28–5.06; Table 3). Similarly, the patients with 1 and 3 CKM conditions had a higher risk of ACS/stroke/TIA, even after adjusting for covariates (sHR, 2.4, 95% CI, 1.37–4.23; and sHR, 4.12; 95% CI, 1.84–9.23, respectively; Table 3).
Across the different multivariable adjustment models (Supplementary material, Table S5), the association between CKM burden and the composite outcome remained consistent with the main analysis. For all‑cause death, the patients with 2 CKM conditions showed an increased risk across all models, except for the model adjusted for CKD stages, whereas an increased risk for patients with 3 CKM conditions emerged only in the model adjusted for pharmacologic therapy (HR, 2.06; 95% CI, 1.01–4.22).
Regarding thromboembolic and ischemic events, adjustment for pharmacologic therapy attenuated the differences in risk across the CKM categories. In contrast, when adjusting for CKD stages, all CKM categories were associated with an increased risk, with the highest risk observed in the patients with 3 CKM conditions (HR, 10.49; 95% CI, 4.19–26.29). The results comparable to the main analysis were observed with the other adjustment models.
Concerning hHF, the presence of 3 CKM conditions was consistently associated with a higher risk across all models (with the only exception of adjustment for CKD stages), while only minor variations for the patients with 1 or 2 CKM conditions were observed, depending on the adjustment applied.
When analyzing the CKM phenotypes (Supplementary material, Table S6), the cardiovascular component was associated with the highest risk, both as a single condition (HR, 1.86; 95% CI, 1.3–2.67) and when combined with kidney (cardiovascular‑kidney phenotype) or metabolic (cardiovascular‑metabolic phenotype) components (HR, 2.06; 95% CI, 1.4–3.03; and HR, 1.82; 95% CI, 1.05–3.17, respectively), as compared with the CKM‑free individuals. Conversely, among the patients with only 1 CKM condition, the metabolic phenotype was associated with a significantly lower risk of adverse events, as compared with the cardiovascular or renal ones (HR, 0.5; 95% CI, 0.26–0.97). No significant differences in the risk were observed across different phenotype combinations among the patients with 2 CKM conditions (Supplementary material, Table S6).
Subgroup analyses
Subgroup analyses for the primary end point are reported in Figure 3.

As depicted in Figure 3A, no significant interaction was observed with sex, obesity, hypertension, HF, COPD, and AF type. In Figure 3B, age was modeled as a continuous variable, and showed a progressive, linear association with adverse events (P <0.001; P for nonlinearity = 0.14), but no significant interaction was found with CKM status (P for interaction = 0.27). As shown in Figure 3C, BMI was not independently associated with the risk of adverse events (P = 0.13), and no interaction was found with CKM status (P for interaction = 0.58), although the patients with 2–3 CKM conditions consistently had a higher risk across all BMI values. Finally, LAVi (Figure 3D) was strongly associated with the risk of the primary end point (P <0.001), with a nonlinear relationship (P for nonlinearity = 0.003), but again no marked interaction was observed with the CKM status (P for interaction = 0.5).
Sensitivity analyses with different definitions of cardiovascular‑kidney‑metabolic conditions
Baseline characteristics of the patients included in the sensitivity analyses using different criteria for the definition of CKM conditions are reported in Supplementary material, Tables S7–S9. The percentage of patients with at least 1 CKM condition increased when including also obesity or HF in the metabolic and cardiovascular components, respectively. On the contrary, it decreased when excluding stroke from the cardiovascular condition, as detailed in Supplementary material, Table S8. Similarly to the main analysis, a progressively higher prevalence of concomitant diseases, and higher CHA2DS2-VA and HAS‑BLED scores were also noted across CKM strata (all P <0.001).
Treatment patterns (Supplementary material, Tables S10–S12) showed consistent trends with increasing CKM burden, with more frequent use of cardiometabolic therapies, such as MRAs, statins, and SGLT2is among the patients with multiple CKM conditions.
Regarding survival analyses (Supplementary material, Table S13), the association between the number of CKM conditions and the risk of the primary composite outcome remained broadly consistent when alternative definitions of cardiovascular or metabolic conditions were applied. However, the effect estimates were attenuated for the patients with 1 CKM condition—particularly for all‑cause death—after multivariable adjustment, irrespective of the definition used.
Discussion
In this prospective, real‑world cohort of AF patients, we observed that CKM comorbidities were highly prevalent, with more than half of the population presenting at least 1 condition, and their burden was closely associated with both progressive LA remodeling and an increased risk of adverse clinical outcomes. Our findings reinforce the concept that AF should be regarded not only as an isolated rhythm disorder but rather as a systemic manifestation of CKM multimorbidity, with shared pathophysiological mechanisms linking structural remodeling, metabolic dysregulation, and cardiorenal impairment.
Recent data from the AHA have reframed the CKM construct as a multidimensional continuum encompassing interrelated cardiovascular, renal, and metabolic disturbances that evolve over time toward multiorgan dysfunction.13,25 In our cohort, CKM conditions frequently clustered and were more common than previously reported in the general population, suggesting that AF patients represent an enriched population for CKM multimorbidity.12,26 Of note, the patients with higher CKM burden were older, more frequently hypertensive, and had higher CHA2DS2-VASc and HAS‑BLED scores, reflecting advanced systemic disease.27,28 The progressive increase in permanent AF among the patients with 2 or more CKM conditions further supports the notion that the CKM status is a marker of disease chronicity and a potential driver of arrhythmia persistence.29
Concerning treatments, the use of OACs was overall high in our cohort, with some variations according to the CKM burden. Specifically, the patients without CKM conditions showed a slightly lower OAC use (87.7%), likely reflecting their lower thromboembolic risk and comorbidity burden. OAC use increased progressively among the patients with 1 or 2 CKM conditions, but decreased to 86.2% in those with 3 CKM conditions, possibly due to concerns regarding bleeding risk in this more complex population.30,31 Similarly, differences emerged in the selection of rhythm control strategies: the patients with 2 or 3 CKM conditions were less likely to receive rhythm control interventions. This trend may be explained by the higher prevalence of permanent AF, advanced age, and greater overall comorbidity burden in this subgroup.32,33
Importantly, our study provides the first detailed echocardiographic evidence linking the cumulative burden of CKM conditions to progressive LA remodeling in AF. We observed a clear, graded relationship: the greater the number of CKM conditions, the more pronounced the LA dilation and dysfunction.
These findings suggest that the CKM axis contributes to atrial structural and functional remodeling through several converging mechanisms. Chronic pressure overload from hypertension and vascular stiffness, metabolic inflammation and lipotoxicity from insulin resistance, and uremic toxicity from renal dysfunction all contribute to the atrial substrate. This remodeling may both predispose to AF onset and perpetuate its persistence, potentially reducing the efficacy of rhythm control strategies.
Moving toward adverse events, the relationship between CKM burden and clinical outcomes was consistent across multiple analyses. As compared with the patients without CKM conditions, those with 1, 2, and 3 conditions experienced a stepwise increase in the risk of death, ischemic events, and hHF, with a more than 2‑fold higher adjusted risk in the group with the greatest CKM burden. These data align with prior studies, stressing the synergistic effect of comorbidity clusters on adverse outcomes in AF, and extend them by quantifying the incremental prognostic weight of CKM domains.27,28 Moreover, some differences were observed across the various combinations of CKM conditions. Of note, the cardiovascular and cardio‑kidney phenotypes carried the highest risk, highlighting the dominant contribution of atherosclerosis and renal dysfunction to clinical deterioration in AF. In contrast, the metabolic condition was associated with a lower contribution, likely because these patients are often in better general condition, with a more favorable risk profile, potentially reflecting younger age, lower overall comorbidity burden, a more frequent use of disease‑modifying cardiometabolic therapies, and when appropriately managed, a lower likelihood of adverse events.34
Concerning the individual components of the primary outcome, the weaker associations with ischemic events observed for the patients with 2 CKM conditions likely reflect limited statistical power, a relatively small sample size, and heterogeneity in the contribution of individual CKM conditions, rather than true biological differences.
From a pathophysiological standpoint, these findings emphasize the interconnected nature of the CKM dysfunction. Atherosclerosis, endothelial injury, chronic low‑grade inflammation, and neurohormonal activation form a vicious circle that amplifies cardiac and renal remodeling, impairs hemodynamic reserve, and worsens diastolic function.35,36 Within this framework, AF may represent both a marker and a mediator of CKM progression, as irregular atrial contraction exacerbates atrial stretch, impairs renal perfusion, and worsens metabolic control. This bidirectional relationship underscores the need for an integrated approach to risk stratification and management.37
Clinically, our results advocate for a paradigm shift toward multidisciplinary care in AF.9,38 Comprehensive and holistic strategies targeting upstream CKM pathways are warranted.39,40 Beyond pharmacologic therapy, implementation of CKM‑integrated models of care may synergistically improve outcomes by addressing the shared substrate of AF and CKM syndrome.41,42 Beyond its prognostic implications, CKM assessment could be systematically integrated into the Atrial fibrillation Better Care pathway to identify patients at a higher risk of adverse outcomes who may benefit from intensified cardiometabolic therapy or closer monitoring. The patients with multiple CKM conditions may represent a subgroup in which early initiation of disease‑modifying agents, such as SGLT2is, glucagon‑like peptide‑1 receptor agonists, or MRAs, or a more aggressive rhythm control strategy is particularly warranted. Moreover, CKM burden could guide a more personalized AF management. Routine incorporation of CKM evaluation into clinical practice may therefore refine risk stratification, enhance individualized care, and ultimately improve long‑term outcomes in this high‑risk population.
In addition, future studies should explore whether CKM burden could serve as a biomarker to guide treatment intensity, and whether emerging cardiometabolic agents can modify atrial remodeling. In parallel, expanding the representation of CKM multimorbidity in clinical trials will be critical to capture the true spectrum of risk and to assess therapeutic effects across overlapping disease domains.
Taken together, our findings provide new insights into the intertwined nature of CKM burden among AF patients. CKM multimorbidity is common, clinically relevant, and independently associated with LA remodeling and adverse outcomes. Recognizing AF into the broader CKM syndrome highlights an opportunity for early identification and comprehensive management of this high‑risk population, ultimately aiming at interrupting the vicious circle of systemic dysfunction and disease progression.
Limitations
This study should be interpreted in light of several limitations. First, although the prospective design strengthens our findings, the single‑center observational nature limits the ability to infer causality. This study was conducted in a single tertiary‑care center, which may introduce referral bias and reflect regional diagnostic and management practices. Therefore, the prevalence of CKM phenotypes and the strength of their associations with clinical outcomes may not be fully generalizable to other populations or health care systems, such as Asian.43
Second, the definition of CKM conditions relied on the available clinical data and albuminuria was not assessed, potentially resulting in an underestimation of CKD prevalence. Such nondifferential misclassification could have attenuated the observed associations with adverse outcomes, suggesting that the true impact of CKD may be greater than reported. Likewise, the metabolic domain was defined by the presence of type 2 diabetes, consistent with previous studies,18,44 but did not include measures of insulin resistance or lipid metabolism. Although obesity was excluded from the primary definition, we performed both interaction and sensitivity analyses including obesity.
Third, residual confounding cannot be completely ruled out despite multivariable adjustments, particularly given the potential influence of unmeasured or incompletely captured clinical variables (eg, socioeconomic status, diet, physical activity, and inflammatory biomarkers, phenotypic classification of HF, achievement of therapeutic targets for comorbidity management as well as international normalized rate values and potentially inappropriate direct OAC dosing). Similarly, AF burden could not be directly assessed; we used time since the first diagnosis as a surrogate, which may not fully capture arrhythmia‑related risk or its impact on atrial remodeling and clinical outcomes.
Moreover, the relatively small sample size and limited number of events in certain CKM subgroups may have reduced statistical power and contributed to nonlinear associations for specific outcomes, such as ischemic events.
Furthermore, echocardiographic data were available only in a subset of patients, which may have introduced selection bias, although baseline characteristics were comparable with the overall cohort.
Conclusions
In a contemporary, prospectively enrolled cohort of AF patients, CKM multimorbidity was highly prevalent and closely linked to progressive LA remodeling and adverse clinical outcomes. The increasing CKM burden was associated with a stepwise rise in the risk of adverse events, independent of conventional risk factors, underscoring the pivotal r ole of CKM dysfunction as a systemic substrate underlying AF progression and highlighting the need for integrated, multidisciplinary care.
- Tan S, Zhou J, Veang T, et al. Global, regional, and national burden of atrial fibrillation and atrial flutter from 1990 to 2021: sex differences and global burden projections to 2046 ‑ a systematic analysis of the Global Burden of Disease Study 2021. Europace. 2025; 27: euaf027. | Crossref
- Kornej J, Börschel CS, Benjamin EJ, Schnabel RB. Epidemiology of atrial fibrillation in the 21st century: novel methods and new insights. Circ Res. 2020; 127: 4‑20. | Crossref
- Chugh SS, Havmoeller R, Narayanan K, et al. Worldwide epidemiology of atrial fibrillation: a Global Burden of Disease 2010 Study. Circulation. 2014; 129: 837‑847. | Crossref
- Cheng S, He J, Han Y, et al. Global burden of atrial fibrillation / atrial flutter and its attributable risk factors from 1990 to 2021. Europace. 2024; 26: euae195. | Crossref
- Lip GYH, Proietti M, Potpara T, et al. Atrial fibrillation and stroke prevention: 25 years of research at EP Europace Journal. Europace. 2023; 25: euad226. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION