Endurance capacity and muscle strength as a composite indicator of physical reserve in men with systolic heart failure
Key words: 6-minute walk test, exercise tolerance, hand strength, heart failure, strength

 CC BY 4.0
CC BY 4.0
Endurance capacity and muscle strength as a composite indicator of physical reserve in men with systolic heart failure
Introduction: Reduced composite physical reserve (CPR) may coexist with systolic heart failure (HF).
Objectives: We aimed to evaluate clinical differences among patients stratified by CPR in the 6‑minute walk test (6MWT) and maximal handgrip (MHG) strength, and to identify clinical correlates of reduced physical function.
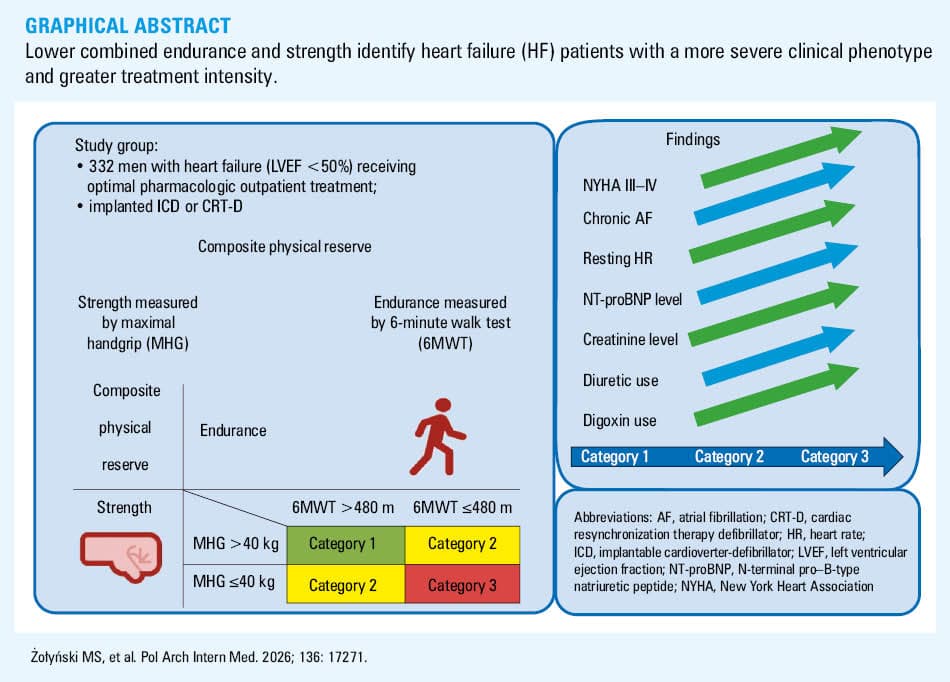
Patients and methods: This post hoc analysis included 332 men from a prospective cohort of outpatients with stable HF (left ventricular ejection fraction <50%) who completed both tests. The patients were stratified into 3 categories based on median splits of 6MWT (480 m) and MHG (40 kg) to define CPR: 1) both 6MWT and MHG values above the group medians; 2) either 6MWT or MHG at or below the median; or 3) both parameters at or below the median. Patient clinical characteristics were compared using analysis of covariance (estimated marginal means and SE) and logistic regression (odds ratios [ORs]), adjusted for age, diabetes, and smoking.
Results: The category 3 patients had higher mean (SD) resting heart rate (72.2 [0.96] vs 64.4 [1.1] bpm; P <0.001), serum creatinine level (1.27 [0.03] vs 1.16 [0.04] mg/dl; P <0.001), and N‑terminal pro–B‑type natriuretic peptide level (log10 3.09 [0.05] vs 2.76 [0.05] pg/ml; P <0.001) than the category 1 patients. Each 1‑category increase was associated with greater odds of New York Heart Association class III–IV (OR, 2.6; 95% CI, 1.78–3.8), resting heart rate above 75 bpm (OR, 2.44; 95% CI, 1.64–3.64), chronic atrial fibrillation (OR, 1.53; 95% CI, 1.06–2.2), and increased use of diuretics (OR, 1.53; 95% CI, 1.02–2.29) and digoxin (OR, 1.99; 95% CI, 1.17–3.39).
Conclusions: Lower combined endurance and strength identify HF patients with a more severe clinical phenotype and greater treatment intensity. This functional performance–based categorization may offer a simple, promising tool for clinical phenotype stratification in systolic HF.
What's new?
We propose composite physical reserve (CPR) as a novel functional construct integrating exercise tolerance (6‑minute walk test) and muscle strength (maximal handgrip strength). In men with systolic heart failure (HF; left ventricular ejection fraction <50%), reduced CPR was associated with a significantly more severe clinical phenotype, including elevated concentration of N‑terminal pro–B‑type natriuretic peptide, higher resting heart rate, increased diuretic and digoxin burden, and advanced New York Heart Association class. This dual‑marker approach enhances the assessment of HF clinical severity stratification using noninvasive tests of skeletal muscle function. Future studies should investigate whether enhancing CPR leads to improved clinical outcomes.
Introduction
Systolic heart failure (HF) profoundly impacts various organs and tissues.1 It triggers systemic inflammation, sympathetic activation, peripheral vasoconstriction, and nutrient deprivation.2-4 Consequently, muscle wasting, myocyte apoptosis, muscle fiber loss, and biochemical / metabolic alterations occur.2-4 Additionally, cardiac cachexia and sarcopenia further diminish muscle strength and exertional capacity.2-4
The 6‑minute walk test (6MWT) primarily reflects the function of type 1 and 2A fibers, while maximal handgrip (MHG) strength is more indicative of type 2X fiber performance.2-4 These tests are widely used in HF assessment and provide complementary insights into physical functioning.
Human skeletal muscles consist of 3 main fibers: type 1, type 2A, and type 2X.5 Slow‑twitch type 1 fibers rely on oxygen‑dependent aerobic metabolism and are characterized by higher level of myoglobin, oxidative enzymes, vascularization, and mitochondria.6-8 The type 1 fibers are predominantly found in the muscles responsible for posture and stabilization. Fast‑twitch type 2X (or 2B) fibers depend on anaerobic glycolysis, are rich in glycogen, and excel in power efforts or explosive movements of shorter duration.9 Type 2A fibers are aerobic, fast‑oxidizing, and share characteristics of both slow- and fast‑twitch fibers.5 They contract more powerfully than the type 1 fibers but do not fatigue as quickly as the type 2X ones. The 2A fibers are responsible for movement or prolonged endurance exercise.
The 6MWT assesses exercise tolerance10 and reflects the performance of type 1 and 2A fibers mainly in aerobic conditions. The MHG test measures muscle strength and predominantly reflects performance of type 2X fibers, which are adapted to anaerobic metabolism. These tests are widely used in the examination of HF patients.11
A shorter distance covered during the 6MWT is associated with more advanced systolic HF and an increased risk of adverse clinical outcomes, including mortality.12 A low MHG score is linked to frailty and predicts a poorer prognosis.13 While each test provides prognostic information independently, their combined interpretation may reveal unique patient phenotypes that are not apparent when analyzed in isolation. The clinical value of combining normal and abnormal 6MWT and MHG results for phenotyping and assessing disease severity in HF patients remains unclear. Exercise tolerance and muscle strength collectively comprise the composite physical reserve (CPR).
Given known sex‑based differences in muscle strength and exercise capacity, this study focused exclusively on men to reduce biological variability and enhance phenotype characterization. We aimed to compare clinical characteristics and HF severity among men divided into 3 functional categories based on the median 6MWT and MHG results. We hypothesize that stratification by 6MWT and MHG may help identify distinct clinical phenotypes among patients with systolic HF. Such a tool could be useful in clinical characterization and possibly treatment planning.
Patients and methods
Participant characteristics
This study is a post hoc analysis of data from prospectively enrolled outpatients with stable systolic HF and left ventricular ejection fraction (LVEF) below 50% and New York Heart Association (NYHA) class I–IV. The data were collected as part of the cross‑sectional component of the project “Predicting Adverse Clinical Outcomes in Patients with Implanted Defibrillating Devices” (grant number TEAM/2009–4/4), awarded by the Foundation for Polish Science for research conducted between October 2010 and February 2014.14,15 The study received approval from the Bioethics Committee of the Poznan University of Medical Sciences (363/10) and adhered to the principles outlined in the Declaration of Helsinki.16 Study participation was voluntary. All participants provided informed written consent.
Clinical evaluation
From an initial cohort of 457 patients, all women were excluded, leaving 389 men. From this group, 57 individuals were further excluded due to incomplete functional or echocardiographic data. The specific reasons for exclusion were: inability to safely perform the 6MWT (primarily due to prior stroke or gait impairment; n = 30), temporary technical failure of the hand dynamometer (n = 15), and poor echocardiographic image quality that precluded reliable LVEF assessment (n = 12). The final study population comprised 332 men who had complete datasets, including confirmed LVEF below 50% and results from both the 6MWT and MHG assessments.
During a standard cardiac examination, brachial systolic blood pressure (SBP), diastolic blood pressure (DBP), and mean blood pressure (MBP) were measured in a seated position using either an Omron M3 (Omron, Kyoto, Japan) or a Colin BPM 7000 (Colin, Sue, Japan) oscillometric sphygmomanometer. Heart rate (HR) was recorded simultaneously.
Biochemical measurements
Venous blood samples were taken for routine biochemical and hematological tests, including concentrations of creatinine, C‑reactive protein (CRP), N‑terminal pro–B‑type natriuretic peptide (NT‑proBNP), hemoglobin, estimated glomerular filtration rate (eGFR) by the Modification of Diet in Renal Disease formula, ionized calcium, and white blood cell count. The methods for analyzing the samples were the same as those used in previous papers related to the project.14,15
Transthoracic echocardiography
Standard echocardiography was performed using either an Acuson CV70 (Siemens, Erlangen, Germany) or a MyLab 30 CV (Esaote, Florence, Italy) device, in accordance with current guidelines.17 Left ventricular end‑diastolic dimension, left ventricular end‑systolic dimension, and left atrial (LA) dimension, LVEF value, aortic root diameter, and proximal right ventricular outflow were measured, together with the thickness of the interventricular septum and left ventricular posterior wall, mitral E and A velocities, mitral E wave deceleration time, and the ratios of E to e' and E to A. The measurement method was the same as previously reported.14,15
Maximal handgrip strength measurement
MHG was measured 3 times on each hand in a seated position using a Jamar hydraulic hand dynamometer (Sammons Preston Rolyan, Bolingbrook, Illinois, United States),18 with the highest value used for analysis.
Six‑minute walk test
For the 6MWT, the patients walked along a 32‑meter straight, level corridor,19 and the final distance was recorded with an accuracy of 1 meter. After completing the 6MWT, the patients reported fatigue using the rate of perceived exertion on the standard Borg visual scale. Arterial blood oxygen saturation was measured continuously during the test.
Patient categorization
The patients were stratified into 3 categories based on the whole‑group median scores of MHG (40 kg) and 6MWT (480 m; Table 1). Category 1 included the patients with higher endurance and muscle strength, that is, with the 6MWT and MHG results above their respective medians (>480 m and >40 kg); category 2 included the individuals with either median or below‑median endurance (indicated by the 6MWT) or median or below‑median strength (indicated by the MHG); and category 3 grouped those with the lowest endurance and muscle strength, with the 6MWT and MHG results at or below their respective medians (<480 m and <40 kg).
Parameter | Endurance, 6MWT | ||
>480 m | <480 m | ||
Abbreviations: 6MWT, 6‑minute walk test; MHG, maximal handgrip | |||
Strength, MHG | <40 kg | Category 1 | Category 2 |
>40 kg | Category 2 | Category 3 | |
Statistical analysis
Continuous data, assessed for normality using histograms, QQ plots, and the D’Agostino–Pearson test, were non‑normally distributed and are presented as medians and interquartile ranges (IQRs).20 Group comparisons were performed using the Kruskal–Wallis test (nonparametric analysis of variance) and Dunn–Bonferroni post hoc test for pairwise comparisons. Categorical data were summarized as frequencies and percentages and analyzed using the Pearson χ2 test, with the Fisher exact test applied where appropriate. The Cochran–Armitage test was utilized to assess for linear trends in categorical variables across the 3 ordinal patient categories. Given the exploratory and descriptive nature of the clinical phenotyping, P values for comparisons of baseline characteristics and comorbidities are reported as nominal, unadjusted values without correction for multiple testing.
For continuous variables that showed significant differences in the Kruskal–Wallis test, we conducted an analysis of covariance (ANCOVA). To maintain model parsimony and ensure a sufficient event‑per‑variable ratio across all subsequent regression models—particularly for outcomes with low event rates (eg, digoxin use; n = 36)—the number of adjustment covariates was constrained. We selected age, diabetes status, and active smoking for adjustment, as these covariates demonstrated potential confounding relationships with the CPR categories based on their unadjusted univariate associations (assessed via post hoc nonparametric analysis of variance for age and χ2 tests for diabetes and smoking). Results are presented as estimated marginal means and SE across the 3 patient categories, with post hoc pairwise comparisons. Additionally, since resting HR differed across categories, we compared the proportions of patients with HR above 75 bpm. Because nonparametric tests were utilized in the univariable analyses, a sensitivity analysis using a rank ANCOVA (Conover–Iman approach applied to rank‑transformed variables) was additionally performed to verify the robustness of the parametric multivariable models against distributional deviations. Due to the severe right‑skewness in the distribution of NT‑proBNP levels and the nonlinear nature of its relationships, a base‑10 logarithmic transformation (log10 NT‑proBNP) was applied prior to ANCOVA to meet parametric test assumptions.
We performed univariate logistic regression, consistently adjusted for the same 3 covariates (age, diabetes, and smoking) to ensure comparability with the ANCOVA models, to examine the association between HF functional categories (1, 2, and 3) treated as an ordinal independent variable, and various binary clinical outcomes, such as NYHA class III–IV, chronic atrial fibrillation (AF), and resting HR above 75 bpm. These clinical outcomes were selected based on binary variables with significant results in the Fisher exact test. Odds ratios (ORs) reflect the change in odds of each outcome per 1‑category increase in HF functional severity. A 2‑sided P value below 0.05 was considered significant. All analyses were performed using PQStat v.1.8.4.142 (PQStat Software, Poznań, Poland).
Results
Patient distribution across the 3 CPR categories was as follows: category 1 (higher endurance and strength), 94 patients (28.31%); category 2 (intermediate), 114 patients (34.34%); and category 3 (lowest endurance and strength), 124 patients (37.35%).
As shown in Table 2, the patients in category 3 presented with the most severe clinical phenotype. They were significantly older and had a higher prevalence of AF, diabetes, and advanced symptoms (NYHA class III or IV). In comparison with categories 1 and 2, the category 3 patients exhibited more pronounced cardiac impairment, including larger LA diameters, higher resting HR (more frequently >75 bpm), and elevated NT‑proBNP concentrations. They also demonstrated a poorer metabolic and inflammatory profile, with higher creatinine and CRP levels, and lower hemoglobin concentration. Pharmacologically, category 3 was associated with more frequent use of diuretics and spironolactone, but less frequent use of angiotensin‑converting enzyme inhibitors (ACEIs) or angiotensin II receptor blockers (ARBs). Table 3 provides additional clinical details, and Figure 1 illustrates the distribution of patients by NYHA class based on their 6MWT and MHG results.
Parameter | Category | P value for trenda | P value for 2‑proportion comparisonsb | |||||
Category 1 (n = 94) | Category 2 (n = 114) | Category 3 (n = 124) | Category 1 vs 2 | Category 1 vs 3 | Category 2 vs 3 | |||
Data are presented as number (percentage).
a P value for trend in the Cochran–Armitage test
b Pairwise comparison P values are exploratory, nominal values unadjusted for multiple testing.
Abbreviations: ACEI, angiotensin‑converting enzyme inhibitor; AF, atrial fibrillation; ARB, angiotensin II receptor blocker; CABG, coronary artery bypass grafting; HR, heart rate; MI, myocardial infarction; NYHA, New York Heart Association; TIA, transient ischemic attack | ||||||||
Comorbidities | Chronic AF | 19 (20.21) | 24 (21.05) | 44 (35.48) | 0.03 | 0.38 | 0.03 | 0.04 |
Hypertension | 93 (81.58) | 81 (86.17) | 98 (79.03) | 0.4 | 0.45 | 0.21 | 0.63 | |
NYHA class III or IV | 9 (9.57) | 36 (31.58) | 56 (45.16) | <0.001 | <0.001 | <0.001 | 0.03 | |
Stroke/TIA | 5 (5.32) | 12 (10.53) | 13 (10.48) | 0.33 | 0.21 | 0.22 | >0.99 | |
Active smoking | 16 (17.02) | 19 (16.67) | 15 (12.1) | 0.09 | 0.2 | 0.49 | 0.02 | |
Previous MI | 43 (45.75) | 52 (45.61) | 44 (35.48) | 0.19 | >0.99 | 0.16 | 0.12 | |
Diabetes | 21 (22.34) | 31 (27.19) | 48 (38.71) | 0.02 | 0.52 | 0.01 | 0.07 | |
Previous CABG | 5 (5.81) | 16 (14.68) | 13 (11.5) | 0.14 | 0.06 | 0.21 | 0.55 | |
Resting HR >75 bpm | 10 (11.63) | 31 (36.05) | 45 (52.33) | <0.001 | 0.003 | <0.001 | 0.13 | |
Pharmacotherapy | Nitrate | 8 (8.51) | 13 (11.4) | 19 (15.32) | 0.3 | 0.64 | 0.15 | 0.45 |
Digoxin | 7 (7.45) | 8 (7.02) | 21 (16.94) | 0.02 | >0.99 | 0.04 | 0.03 | |
ACEI/ARB | 81 (86.17) | 96 (84.21) | 92 (74.19) | 0.047 | 0.85 | 0.04 | 0.08 | |
β-Blocker | 82 (87.23) | 98 (85.97) | 107 (86.29) | 0.96 | 0.84 | >0.99 | >0.99 | |
Spironolactone | 50 (53.19) | 74 (64.91) | 84 (67.74) | 0.07 | 0.09 | 0.04 | 0.68 | |
Diuretic | 67 (71.28) | 96 (84.21) | 107 (86.29) | 0.01 | 0.03 | 0.01 | 0.72 | |
Statin | 76 (80.85) | 95 (83.33) | 95 (76.61) | 0.39 | 0.72 | 0.51 | 0.26 | |
Parameter | Category 1 (n = 94) | Category 2 (n = 114) | Category 3 (n = 124) | P valuea | P value for post hoc category comparisons | |||
1 vs 2 | 1 vs 3 | 2 vs 3 | ||||||
Data are presented as median (interquartile range).
a Kruskal–Wallis test
SI conversion factors: to convert creatinine to μmol/l, multiply by 88.4; CRP to nmol/l, by 9.524; hemoglobin to mmol/l, by 0.6206; NT‑proBNP to pmol/l, by 0.118.
Abbreviations: BMI, body mass index; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; hs‑CRP, high‑sensitivity C‑reactive protein; LVEDD, left ventricular end‑diastolic dimension; LVEF, left ventricular ejection fraction; LVESD, left ventricular end‑systolic dimension; MBP, mean blood pressure; SBP, systolic blood pressure; WBC, white blood cell count; others, see Tables 1 and 2 | ||||||||
Demographic and clinical characteristics | Age, y | 58.69 (50.27–63.63) | 62.9 (57–67.22) | 70.94 (63.19–75.71) | <0.001 | 0.003 | <0.001 | <0.001 |
MHG, kg | 48 (44–52) | 42 (38–48) | 34 (30–38) | <0.001 | <0.001 | <0.001 | <0.001 | |
6MWT, m | 576 (527.25–613.25) | 480 (401.5–539.5) | 384 (288–448) | <0.001 | <0.001 | <0.001 | <0.001 | |
6MWT, SpO2, % | 97 (96–98) | 96 (95–97.75) | 96 (95–98) | 0.13 | 0.42 | 0.15 | >0.99 | |
6MWT, Borg scale | 12 (10–15) | 12 (10–15) | 12 (10–15) | 0.3 | >0.99 | 0.37 | >0.99 | |
BMI, kg/m2 | 28.05 (26.21–31.03) | 29.41 (26.02–31.65) | 27.62 (24.77–31.19) | 0.17 | >0.99 | 0.96 | 0.18 | |
HR, bpm | 63.08 (58.59–69.1) | 68.49 (61.44–75.09) | 71.33 (63.09–76.86) | <0.001 | 0.007 | <0.001 | 0.11 | |
SBP, mm Hg | 112.85 (105.19–123.65) | 112.03 (102.14–126.42) | 108.64 (98.3–124.45) | 0.32 | >0.99 | 0.64 | 0.56 | |
DBP, mm Hg | 70.42 (63.65–75.77) | 70.26 (64.42–77.15) | 68.5 (60.76–76.45) | 0.23 | >0.99 | >0.99 | 0.26 | |
MBP, mm Hg | 83.9 (78.17–91.24) | 83.44 (76.26–92.38) | 81.42 (72.81–91.47) | 0.23 | >0.99 | 0.7 | 0.3 | |
Laboratory test results | Creatinine, mg/dl | 1.05 (0.91–1.22) | 1.03 (0.92–1.21) | 1.26 (1.02–1.51) | <0.001 | >0.99 | <0.001 | <0.001 |
eGFR, ml/min/1.73 m2 | 76.54 (64.82–91.33) | 77.36 (65.24–88.39) | 60.27 (47.96–78.59) | <0.001 | >0.99 | <0.001 | <0.001 | |
Ionized calcium, mmol/l | 5 (4.8–5.15) | 5 (4.8–5.2) | 4.95 (4.7–5.13) | 0.34 | >0.99 | 0.85 | 0.50 | |
NT‑proBNP, pg/ml | 458.9 (258.55–859.5) | 753.15 (332.78–1651.75) | 1747 (636.55–3329) | <0.001 | 0.06 | <0.001 | <0.001 | |
hs‑CRP, mg/l | 1.8 (1–3.2) | 1.6 (1–2.6) | 2.4 (1.1–5.23) | 0.02 | >0.99 | 0.16 | 0.02 | |
Hemoglobin, g/dl | 14.9 (14–15.7) | 14.7 (13.8–15.3) | 14.15 (13.1–14.9) | <0.001 | 0.43 | <0.001 | 0.03 | |
WBC, 109/l | 7.37 (6.22–9.21) | 7.28 (5.98–8.65) | 7.43 (6.43–8.65) | 0.74 | >0.99 | >0.99 | >0.99 | |
Echocardiographic findings | LVEDD, mm | 60.4 (54.65–67.8) | 61.85 (55.63–68.83) | 60.4 (54.28–68.28) | 0.6 | >0.99 | >0.99 | 0.98 |
LVESD, mm | 50.2 (44.18–57.9) | 52.55 (44.53–58.88) | 51.55 (43.58–61.43) | 0.88 | >0.99 | >0.99 | >0.99 | |
Left atrial diameter, mm | 42.9 (39.2–46.3) | 44.6 (40.4–49.2) | 44.75 (40.2–51.1) | 0.03 | 0.14 | 0.03 | >0.99 | |
LVEF, % | 33.32 (27.33–44.39) | 31.35 (23.89–37.94) | 31.98 (23.18–40.62) | 0.07 | 0.08 | 0.23 | >0.99 | |
Aortic root diameter, mm | 22.95 (20.7–24.7) | 22.6 (21–24.3) | 22.4 (20.33–24.5) | 0.69 | >0.99 | >0.99 | >0.99 | |
Right ventricular diameter, mm | 28.4 (26.6–32.1) | 29.3 (26.43–32) | 29.6 (26.25–33.35) | 0.71 | >0.99 | >0.99 | >0.99 | |
Septal diameter, mm | 11.2 (9.7–12.58) | 11.1 (9.73–12.3) | 11.3 (9.9–12.73) | 0.63 | >0.99 | >0.99 | >0.99 | |
Left ventricular posterior wall diameter, mm | 11.5 (10.43–13.08) | 11.75 (9.68–13.2) | 11.45 (9.8–13.3) | 0.96 | >0.99 | >0.99 | >0.99 | |
Mitral E wave deceleration time, ms | 220.5 (169–272) | 204 (160–284) | 188 (151.5–256) | 0.18 | >0.99 | 0.2 | 0.86 | |
E to e' | 6.74 (5.06–9.57) | 8.13 (5.86–10.86) | 8.21 (5.85–11.71) | 0.03 | 0.06 | 0.07 | >0.99 | |

ANCOVA, adjusted for age, diabetes, and smoking status, was performed for continuous variables with significant Kruskal–Wallis results (Table 4). After adjustment, the patients in category 3 maintained significantly higher resting HR, creatinine, log10 NT‑proBNP, and hemoglobin levels, and LA diameter than those in category 1 (all P <0.05). A sensitivity analysis utilizing rank ANCOVA confirmed that these specific differences were statistically robust and not driven by non‑normal data distributions (Supplementary material). Conversely, while parametric ANCOVA showed no significant difference for high‑sensitivity CRP (hs‑CRP), the rank ANCOVA demonstrated higher ranked hs‑CRP in the category 3 patients (P = 0.001), suggesting that outliers masked this inflammatory signal in the raw data.
Parameter | Category 1 (n = 94) | Category 2 (n = 114) | Category 3 (n = 124) | P value for post hoc category comparisons | ||
Category 1 vs 2 | Category 1 vs 3 | Category 2 vs 3 | ||||
Data are presented as estimated marginal mean (SE) adjusted for age, current smoking status, and diabetes. Post hoc pairwise comparisons are shown for significant group differences.
SI conversion factors: see Table 3
| ||||||
HR, bpm | 64.38 (1.09) | 68.68 (0.93) | 72.18 (0.96) | 0.008 | <0.001 | 0.04 |
Creatinine, mg/dl | 1.16 (0.04) | 1.1 (0.03) | 1.27 (0.03) | 0.85 | <0.001 | <0.001 |
Log10 NT‑proBNP, pg/ml | 2.76 (0.05) | 2.89 (0.05) | 3.09 (0.05) | 0.005 | <0.001 | <0.001 |
hs‑CRP, mg/l | 4.35 (1.05) | 3.71 (0.9) | 5.94 (0.92) | 0.51 | 0.59 | 0.2 |
Hemoglobin, g/dl | 14.54 (0.15) | 14.44 (0.13) | 14.21 (0.13) | 0.15 | <0.001 | 0.004 |
Left atrial diameter, mm | 42.91 (0.81) | 44.66 (0.69) | 45.67 (0.71) | 0.1 | 0.01 | 0.37 |
Logistic regression analysis, similarly adjusted, examined the association between increasing CPR severity (per 1‑category increase from 1 to 3) and key clinical outcomes (Table 5). A higher CPR category was strongly associated with greater odds of advanced HF symptoms (NYHA class III–IV; OR, 2.6), chronic AF (OR, 1.53), tachycardia (HR >75 bpm; OR, 2.44), and increased use of digoxin (OR, 1.99) and diuretics (OR, 1.53). Conversely, the use of ACEIs or ARBs was less likely with higher categories (OR, 0.6). The use of spironolactone was more frequent in higher categories, though this association did not reach significance (OR, 1.36; 95% CI, 0.99–1.88; P = 0.06).
Dependent variable | OR | 95% CI | P value |
Results are presented as odds ratios with 95% CI for each 1‑category increase in heart failure functional severity (from Category 1 to 3), based on univariate logistic regression adjusted for age, diabetes, and current smoking status. Only binary variables with significant differences in the Fisher exact test are included.
Abbreviations: see Table 2 | |||
NYHA class III or IV | 2.6 | (1.78–3.8) | <0.001 |
Chronic AF | 1.53 | (1.06–2.2) | 0.02 |
Digoxin use | 1.99 | (1.17–3.39) | 0.01 |
Diuretic use | 1.53 | (1.02–2.29) | 0.04 |
ACEI/ARB use | 0.6 | (0.4–0.91) | 0.02 |
Spironolactone use | 1.36 | (0.99–1.88) | 0.06 |
Resting HR >75 bpm | 2.44 | (1.64–3.64) | <0.001 |
Discussion
Our findings demonstrate that assessing both physical endurance and muscle strength enables identification of distinct clinical phenotypes in men with systolic HF. Using simple and widely available measures—MHG and 6MWT—we propose a practical and promising categorization system that stratifies patients into 3 functional categories. This system appears clinically relevant, as it effectively distinguishes patients with progressively more severe clinical profiles.
In particular, the patients in category 3, representing the lowest CPR, showed markedly poorer exercise tolerance, weaker muscle strength, enlarged LA, elevated NT‑proBNP levels, and a higher prevalence of NYHA class III–IV symptoms. These patients also required more frequent use of diuretics and aldosterone antagonists. Their older age, along with higher rates of AF and diabetes—both known contributors to impaired mobility—likely add to their functional limitations.
Importantly, logistic regression analysis confirmed that each 1‑category increase in functional severity (from category 1 of the patients with higher endurance and muscle strength to category 3) was significantly associated with adverse clinical features, including NYHA class III–IV symptoms, chronic AF, elevated resting HR, and greater use of digoxin and diuretics. These findings suggest potential clinical utility of this straightforward classification based on functional performance.21
Elevated NT‑proBNP levels suggest prolonged increased cardiac load in the category 3 patients. While the cross‑sectional design precludes causal inference, the observed profile in category 3 suggests several plausible, interrelated pathophysiological mechanisms that warrant further investigation. This may reflect underlying diastolic dysfunction, indicated by enlarged LA (long‑term remodeling) and borderline higher E/e'. Renin‑angiotensin‑aldosterone system activity might also be elevated.22 More advanced diastolic and systolic dysfunctions in this group limit exercise tolerance and compromise cardiac output. Additionally, poorer renal function, lower hemoglobin level, higher resting HR despite similar β-blocker use, increased inflammation (higher hs‑CRP level confirmed via rank sensitivity analysis) may further impair muscle function.
Importantly, adjusted ANCOVA and logistic regression analyses confirmed that the category 3 patients, even after accounting for age, diabetes, and smoking, showed significantly worse hemodynamic and metabolic profiles. These included higher resting HR, creatinine and NT‑proBNP levels, and LA diameter, and lower hemoglobin level, consistent with HF progression. Logistic regression further indicated that progression to worse functional categories was associated with a higher likelihood of advanced HF symptoms (NYHA class III–IV), AF, tachycardia, and greater use of diuretics and digoxin, while ACEI/ARB use declined, likely reflecting both increased disease burden and therapeutic limitations. A significantly greater spironolactone use in category 3 vs category 1 suggests that these patients required more diuretics. Our findings underscore the clinical value of categorizing HF patients by muscle strength and endurance status as a simple and informative approach to stratifying both clinical risk and patient phenotype, closely aligned with disease severity and treatment intensity.
The category 3 patients exhibited a higher resting HR despite comparable β-blocker use. Regarding BP, we observed no significant differences among the studied men, suggesting no association between skeletal muscle dysfunction types and BP. However, existing literature indicates that various training modalities, except aerobic interval training, may reduce BP pressure in prehypertensive and hypertensive patients.23 Specifically, isometric training and running were most effective for lowering SBP and DBP. Unfortunately, comparable data on patients with HF remain scarce.
Despite comparable body mass index (BMI) across the categories, the patients in category 3 had significantly worse muscle function. This suggests that skeletal muscle dysfunction might precede cardiac cachexia and sarcopenia in HF, even in the absence of weight loss or reduced BMI. As HF progresses, sarcopenia and frailty may develop with preserved or increased fat and water mass, masking muscle wasting on BMI assessment.24 Worse CPR in the category 3 patients cannot be explained by statin use or abnormal ionized calcium concentrations, as both parameters were comparable across all categories.
The prognostic value of the skeletal muscle function in HF patients is well established. Izawa et al13 reported an association between reduced MHG and increased mortality in stable HF. Chung et al25 found that patients with advanced HF and reduced muscle strength had a higher mortality risk after ventricular assist device implantation. McGrath et al26 showed that the risk of developing chronic HF increases with lower muscle strength. Our findings are consistent with the concept that muscle function impairment in HF may involve heterogeneous pathophysiology. We hypothesize that this could reflect nonuniform dysfunction across muscle fiber types (eg, predominant type 2A vs type 2X deficits), a possibility that requires direct confirmation in future mechanistic studies utilizing muscle biopsy or advanced imaging. Prior studies suggest prognostic associations of muscle strength and exercise capacity in HF; however, the prognostic value of the CPR construct itself requires prospective validation.
Potential therapeutic interventions to improve muscle strength and exercise capacity in systolic heart failure
CPR can be improved in patients with advanced systolic HF. Cardiac rehabilitation and training with repeated endurance and resistance exercises are recommended for HF patients.27 Hormone therapy (testosterone or growth hormone) may increase muscle mass and strength,28 and dietary supplementation (creatine, branched‑chain amino acids) shows promise.29-31 Additionally, trimetazidine, a metabolic modulator, has been shown to improve skeletal muscle performance in HF.32 The claim that improving the condition of patients with HF can improve their clinical outcome to the level of patients without sarcopenia is speculative and requires further research.
By complementing traditional risk scores and clinical assessments, our simple classification might enhance phenotype‑driven decision‑making and help tailor therapeutic strategies, particularly in outpatient settings where rapid, functional evaluation is essential.
Practical implications and future directions
Despite their limitations, our findings offer immediate, practical implications for clinical assessment. The proposed CPR categorization, derived from 2 rapid bedside tests (<10 min total), provides a simple framework for phenotyping men with HF with reduced EF (HFrEF) during a routine visit. Identifying a patient in category 3 could prompt a more comprehensive evaluation for frailty, occult sarcopenia (even with normal BMI), and treatable contributors, such as anemia or elevated HR, and facilitate the initiation of proper adjunctive therapy to improve muscle mass, strength, and endurance. Conversely, a category 1 profile might support the safety of more intensive exercise prescriptions. Future prospective studies are essential to validate these cutoffs, establish their prognostic value for clinical events, and test whether interventions targeted at improving CPR category can modify patient outcomes.
The primary aim of this study was to provide an exploratory, cross‑sectional description of a novel functional construct of CPR. Future prospective studies are now essential to determine the independent prognostic value of the CPR categories for hard clinical end points, such as mortality, and to test whether interventions aimed at improving physical reserve can modify the patient’s category and subsequent clinical trajectory.
Limitations
This study has several limitations. First, it included only men, which limits the generalizability of the findings by excluding women with systolic HF. Given known sex‑based differences in muscle mass, exercise capacity, and HF pathophysiology, future studies should validate this functional classification in women. Second, the cross‑sectional and observational design precludes causal inference; while associations between functional impairment and clinical severity are evident, the directionality of these relationships cannot be established. However, it is likely that the optimal cutoff values for MHG and 6MWT would differ in women with systolic HF.
Third, the use of cohort‑specific median values to define CPR categories limits the immediate external validity of the proposed cutoffs. These thresholds are population‑specific and may not apply universally across cohorts with different demographic or clinical profiles. However, as CPR is a novel construct lacking established thresholds, this data‑driven approach was necessary to enable its initial operationalization and stratification, providing a basis for future validation against clinical outcomes in external populations.
Fourth, although the 6MWT and MHG are practical and widely used tools, they may not fully capture the multidimensional nature of physical function, including balance, coordination, or lower‑limb strength. Incorporating additional performance‑based or imaging assessments could provide a more comprehensive evaluation of musculoskeletal health in HF.
Fifth, this was a post hoc, exploratory analysis of a retrospectively assembled cohort. The hypothesis regarding the CPR categorization was generated after data collection, necessitating cautious interpretation and prospective validation. Furthermore, the exclusion of patients unable to complete functional tests may have introduced a selection bias toward a less frail population, potentially limiting the generalizability of the findings to the most severely impaired HF patients. This post hoc analysis reflects a treatment era (2010–2014) when standard therapy for HFrEF primarily included β-blockers, ACEIs or ARBs, and mineralocorticoid receptor antagonists.33 Since then, guideline‑directed medical therapy has evolved to include angiotensin receptor‑neprilysin inhibitors and sodium‑glucose cotransporter 2 inhibitors, which have demonstrated additional benefits in HF management.33 As such, generalizability of our findings to contemporary HF populations may be limited. Nevertheless, our results offer a valuable baseline for understanding functional phenotypes in HF and may help quantify the incremental benefits of newer therapies in future longitudinal studies. The characteristics of HF patients have also changed; contemporary cohorts include a greater proportion of women and patients with preserved LVEF.34
Conclusions
In men with systolic HF, combined deficits in muscle strength and endurance define a distinct clinical phenotype that, in this cross‑sectional analysis, was associated with markers of more advanced cardiac dysfunction, greater comorbidity burden, and more intensive treatment patterns. These functional impairments were independently associated with markers of HF severity, regardless of age, diabetes, or smoking status.
Our proposed, exploratory categorization, based on internally derived cutoffs in MHG and 6MWT, offers a pragmatic method for phenotypic stratification that captures clinically meaningful variation in current HF severity.
As a proof‑of‑concept, incorporating the MHG and 6MWT into routine HF assessments could help clinicians identify patients with pronounced functional impairment who might benefit from a more focused evaluation for frailty and sarcopenia. Given that both tests are rapid, inexpensive, and feasible in most outpatient settings, this approach merits further evaluation in prospective studies.
Future research should prospectively validate these findings, establish outcome‑driven cutoffs, and determine whether this functional categorization provides independent prognostic value for clinical events. Furthermore, interventional studies are needed to evaluate whether therapies aimed at improving muscle function and endurance can modify the CPR category and, ultimately, clinical outcomes.
- Yndestad A, Damås JK, Oie E, et al. Systemic inflammation in heart failure – the whys and wherefores. Heart Fail Rev. 2006; 11: 83‑92.
- Josiak K, Jankowska EA, Piepoli MF, et al. Skeletal myopathy in patients with chronic heart failure: significance of anabolic‑androgenic hormones. J Cachexia Sarcopenia Muscle. 2014; 5: 287‑296. | Crossref
- Philippou A, Xanthis D, Chryssanthopοulos C, et al. Heart failure‑induced skeletal muscle wasting. Curr Heart Fail Rep. 2020; 17: 299‑308. | Crossref
- von Haehling S, Ebner N, Dos Santos MR, et al. Muscle wasting and cachexia in heart failure: mechanisms and therapies. Nat Rev Cardiol. 2017; 14: 323‑341. | Crossref
- Talbot J, Maves L. Skeletal muscle fiber type: using insights from muscle developmental biology to dissect targets for susceptibility and resistance to muscle disease. Wiley Interdiscip Rev Dev Biol. 2016; 5: 518‑534. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION