Does rheumatoid arthritis affect the course of chronic hepatitis C and outcomes of antiviral treatment?
2 ,
Key words: direct-acting antivirals, hepatitis C virus, rheumatoid arthritis, sustained virologic response, treatment failure
,
Key words: direct-acting antivirals, hepatitis C virus, rheumatoid arthritis, sustained virologic response, treatment failure

 CC BY 4.0
CC BY 4.0
Does rheumatoid arthritis affect the course of chronic hepatitis C and outcomes of antiviral treatment?
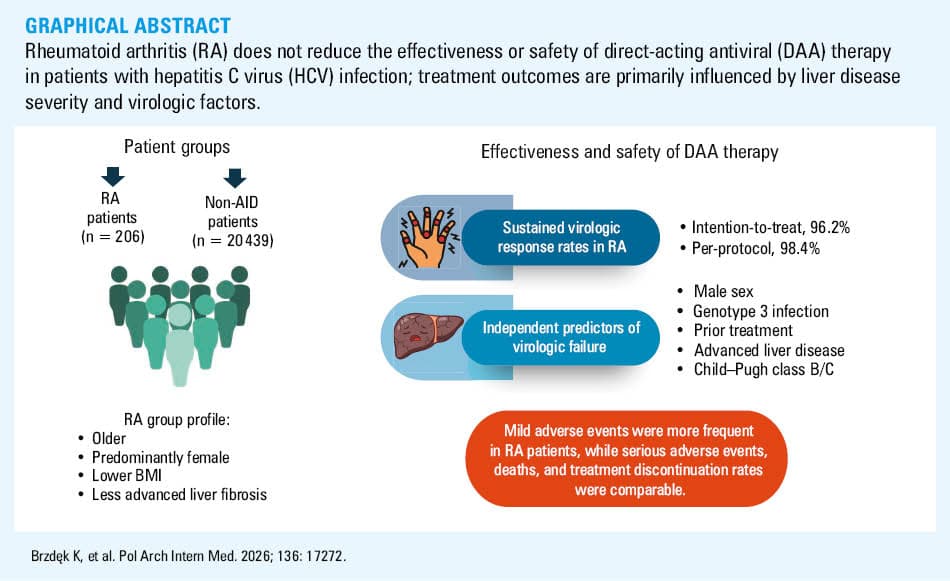
Introduction: Chronic hepatitis C virus (HCV) infection is a systemic disease often associated with extrahepatic autoimmune conditions, including rheumatoid arthritis (RA). Immune dysregulation and immunomodulatory therapy may raise concerns about the effectiveness and safety of direct‑acting antivirals (DAAs), but real‑world data on RA patients are lacking.
Objectives: We aimed to assess whether the presence of RA influences the severity of liver disease and outcomes of DAA therapy in HCV‑infected patients.
Patients and methods: This retrospective multicenter study compared adult HCV‑infected patients with RA and those without autoimmune disease (non‑AID). All patients were treated with DAAs in Polish centers between 2015 and 2024.
Results: Of the 20 645 patients included in the analysis, 206 (1%) had RA. They were older, predominantly female, had lower body mass index, and less advanced liver fibrosis, as compared with the non‑AID group. The sustained virologic response rates were high and comparable between the RA and non‑AID populations (98.4% vs 97.7%). RA was not associated with treatment failure. Independent predictors of virologic failure included male sex, genotype 3 infection, prior antiviral treatment, advanced liver disease, and Child–Pugh class B/C. Mild adverse events were more frequent in the RA patients, while the rates of serious adverse events, death, and treatment discontinuation were comparable.
Conclusions: RA does not contribute to increased severity or progression of HCV‑related liver disease and does not negatively affect the effectiveness or safety of DAA therapy. Liver disease stage and hepatic dysfunction, rather than the presence of RA, are the key determinants of treatment outcomes in patients with chronic HCV infection.
What's new?
This Polish study is the most extensive real‑world analysis to date evaluating the efficacy and safety of direct‑acting antiviral therapy in patients with chronic hepatitis C virus (HCV) infection and concomitant rheumatoid arthritis. The results show that the presence of rheumatoid arthritis does not adversely affect the severity of liver disease caused by HCV. It also does not reduce the chances of patients being cured or increase the risk of serious adverse events, as compared with patients without autoimmune diseases, which was a common observation in the era of interferon‑based therapies used more than a decade ago.
Introduction
According to the latest estimates of the World Health Organization, approximately 50 million people worldwide are living with hepatitis C virus (HCV) infection, and approximately 1 million new cases occur each year.1 Although HCV infection is often asymptomatic, it can lead to chronic hepatitis C (CHC). The most serious consequences of the disease are cirrhosis with the risk of liver failure and hepatocellular carcinoma (HCC).2,3 These complications account for over 242 000 deaths annually, despite the availability of modern, safe, and highly effective direct‑acting antiviral (DAA) regimens.4
In addition to liver‑related injury, HCV affects multiple tissues and organ systems, including the immune, dermatological, vascular, endocrine, and neuropsychiatric systems, resulting in numerous extrahepatic manifestations.5 The most frequently reported conditions include cryoglobulinemia, thrombocytopenia, autoimmune disorders, dermatological lesions, and diabetes mellitus.6 According to available data, 40%–75% of patients with chronic HCV infection develop at least 1 extrahepatic symptom.7,8
Since the discovery of HCV, a link has been consistently reported between contracting the virus and the incidence of autoimmune diseases (AID) among infected individuals. Approximately 70% of patients with chronic infection present with nonorgan‑specific autoantibodies, such as smooth muscle antibodies (5%–91%), antinuclear antibodies (9%–38%), rheumatoid factor (45%–70%), and anticardiolipin antibodies (15%–20%).9,10 Thyroid autoantibodies and cryoprecipitates containing rheumatoid factors are also frequently detected.11 These findings support the hypothesis that HCV may stimulate the immune system, promoting the development of autoimmune disorders.12
Chronic immune dysregulation associated with HCV constitutes a significant risk factor for a variety of AIDs, including rheumatic disorders, such as Sjögren syndrome, systemic lupus erythematosus, and rheumatoid arthritis (RA).13,14 Numerous studies have also indicated a link between HCV infection and an increased risk of RA.15-17 Although the pathogenesis of HCV‑related RA is not fully understood, 3 potential mechanisms have been proposed: direct synovial membrane injury due to viral invasion, induction of autoimmune responses within the synovium, and deposition of immune complexes or cryoglobulins.18
This study aimed to assess whether the presence of RA in patients with chronic HCV infection affects the clinical characteristics, the parameters defining liver disease and HCV infection, and the effectiveness and safety of DAA therapy.
Patients and methods
Study population
We selected the study population from a cohort of all consecutive adult patients who initiated DAA regimens for CHC between July 1, 2015 and December 31, 2024, across 22 specialized hepatology centers in Poland. We performed the analysis based on data from the EpiTer‑2 database, a multicenter, retrospective study evaluating real‑world HCV antiviral therapy, conducted with the support of the Polish Society of Epidemiologists and Infectiologists (www.epiter‑2.pl).
Therapeutic decisions regarding the DAA regimen for each patient were made individually by the treating physician. The choice of treatment depended on the available therapeutic options, and the therapy was administered in accordance with the product leaflet, the protocols of the National Health Fund treatment program, and the recommendations of the Polish Expert Group on Hepatitis C.19-21
Data collection
Data were collected retrospectively via an online platform administered by Tiba Sp. z o. o. (Wrocław, Polska), utilizing patients’ medical records as the primary source of information. Baseline data encompassed both demographic and clinical characteristics, including sex, age, body mass index (BMI), coinfections with HIV and hepatitis B virus, comorbid conditions, liver disease severity, concurrent medications, and prior exposure to antiviral treatment.
Laboratory parameters assessed at treatment initiation included serum concentrations of bilirubin, albumin, and creatinine, alanine aminotransferase activity, hemoglobin concentration, international normalized ratio, platelet count, HCV genotype, and viral load.
The patients included in the study were divided into 2 groups: 1) patients with RA, and 2) patients without RA or any other AID (non‑AID). Patients with autoimmune diseases other than RA were excluded from the analysis to ensure that these would not influence the final results of this study. We subsequently compared these 2 patient subpopulations in terms of baseline characteristics, therapeutic regimens, treatment effectiveness, and safety profiles.
Diagnosis of rheumatoid arthritis
RA is a systemic AID characterized by inflammatory arthritis and extra‑articular involvement. We established the diagnosis of RA following a comprehensive medical interview and an in‑depth analysis of patient clinical records. The disease was diagnosed by rheumatologists in accordance with the criteria of the American College of Rheumatology / European League Against Rheumatism (ACR/EULAR), and the patients with RA remained under the ongoing care of rheumatologists.
Analysis of liver disease severity
We determined the severity of liver disease based on liver stiffness assessment utilizing noninvasive methods for fibrosis quantification. These included real‑time shear‑wave elastography using the Aixplorer system (SuperSonic Imagine, Aix‑en‑Provence, France) and transient elastography with the FibroScan device (Echosens, Aix‑en‑Provence, France). We assessed the fibrosis staging in accordance with the recommendations issued by the European Association for the Study of the Liver (EASL) and the METAVIR classification system.22 We adopted the liver stiffness threshold of 13 kPa as the cutoff value indicative of a high probability of cirrhosis (F4).22
For all patients with cirrhosis, we evaluated the liver function status using the Child–Pugh (CP) score. Additionally, we collected clinical data regarding hepatic decompensation in the past or at the time of treatment initiation, the presence of esophageal varices, a history of HCC, and orthotopic liver transplant.
We conducted the study in accordance with the Declaration of Helsinki, and the use of retrospective data was approved by the Bioethics Committee of the Jan Kochanowski University in Kielce (57/2024). As the investigation was retrospective in nature, obtaining additional patient consent was not obligatory; nonetheless, the participants were asked to submit informed consent forms for inclusion in the therapeutic program.
Assessment of treatment effectiveness
The primary end point of the study and the principal indicator of DAA therapeutic effectiveness was the achievement of sustained virologic response (SVR). It was defined as undetectable HCV RNA at least 12 weeks after completion of therapy. The patients in whom viral genetic material remained detectable at this time point were virologic nonresponders. The individuals who did not undergo HCV RNA testing 12 weeks after treatment were categorized as nonvirologic treatment failures. In accordance with EASL and national recommendations, an HCV RNA level not exceeding 15 IU/ml was adopted as the diagnostic threshold for viral detectability.19,22 We included all patients who started treatment in the intention‑to‑treat analysis. The per‑protocol analysis encompassed only the individuals with available HCV RNA testing data at 12 weeks after treatment completion. Furthermore, we assessed treatment effectiveness in the subgroup of patients whose complete data on both liver fibrosis stage and HCV genotype were available.
Assessment of treatment safety
We evaluated treatment safety throughout the entire therapeutic period and during 12‑week post‑treatment follow‑up. Safety data included all cases of treatment modifications in the form of changes in ribavirin (RBV) dosage or discontinuation, as well as the occurrence of adverse events, serious adverse events, and deaths. We placed particular emphasis on hepatic safety outcomes, including gastrointestinal bleeding, ascites, and hepatic encephalopathy.
Statistical analysis
We executed statistical procedures using Statistica version 13 (StatSoft, Tulsa, Oklahoma, United States) and GraphPad Prism 5.1 (GraphPad Software, Inc., La Jolla, California, United States) packages. We summarized the continuous variables as medians with interquartile ranges (IQRs). We performed intergroup comparisons for continuous nonparametric data using the Mann–Whitney test. The assumption of normal distribution was examined with the Shapiro–Wilk test. We described the categorical variables using absolute frequencies and corresponding proportions. Between‑group comparisons of categorical data were performed with the Pearson χ2 test; when expected cell counts were below 5, the Fisher exact test was applied. Since this analysis was exploratory and descriptive, no adjustment for multiple testing was applied.
Additionally, we utilized multivariable logistic regression models to estimate the probability of treatment failure across the 2 study cohorts. We presented results as odds ratios (ORs) with their respective 95% CIs. A P value below 0.05 was considered significant for all applied tests.
Results
Baseline characteristics of the study population
Our analysis initially included 21 500 patients, of which we excluded 855 due to having an AID other than RA: systemic lupus erythematosus, autoimmune hepatitis, psoriasis, multiple sclerosis, systemic sclerosis, Sjögren syndrome, vasculitis, Graves disease, Hashimoto disease, autoimmune encephalitis, atopic dermatitis, type 1 diabetes mellitus, celiac disease, myasthenia gravis, inflammatory bowel disease, primary biliary cholangitis, and primary sclerosing cholangitis.
Among the 20 645 patients treated for HCV infection included in the analysis, 206 (1%) were diagnosed with RA (Figure 1). The individuals with RA were significantly older than those in the non‑AID group, with a median (IQR) age of 63 (58–68) vs 58 (48–66) years (P <0.001). Women predominated in the RA cohort, comprising 79.6% of the patients, as compared with 51.4% of the non‑AID group (P <0.001). The patients with RA had lower median BMI than those without AID (24.7 [22.8–27] vs 26.8 [24.1–30] kg/m2; P = 0.01; Table 1).

Abbreviations: AID, autoimmune disease; IFN, interferon; RA, rheumatoid arthritis
Parameter | All patients (n = 20 645) | RA group (n = 206) | Non‑AID group (n = 20 439) | P value | |
Data are presented as number (percentage) or median (interquartile range).
SI conversion factors: to convert ALT to μkat/l, multiply by 0.0167; albumin to g/l, by 10; bilirubin to μmol/l, by 17.1; hemoglobin to g/l, by 10; creatinine to μmol/l, by 88.4; HCV RNA to copies/ml, by 5.6.
Abbreviations: ALT, alanine transaminase; BMI, body mass index; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; others, see Figure 1 | |||||
Age, y | 58 (48–66) | 63 (58–68) | 58 (48–66) | <0.001 | |
Age ≥50 y | 10 753 (52.1) | 174 (84.5) | 10 579 (51.8) | <0.001 | |
Sex | Men | 10 544 (51.1) | 42 (20.4) | 10 502 (51.4) | <0.001 |
Women | 10 101 (48.9) | 164 (79.6) | 9937 (48.6) | ||
BMI, kg/m2 | 26.8 (24.1–30) | 24.7 (22.8–27) | 26.8 (24.1–30) | 0.01 | |
Comorbidities | Any comorbidities other than RA | 13 255 (64.2) | 174 (84.5) | 13 081 (64) | <0.001 |
Obesity (BMI ≥30 kg/m2) | 3555 (17.2) | 33 (16) | 3522 (17.2) | 0.65 | |
Arterial hypertension | 6469 (31.3) | 97 (47.1) | 6372 (31.2) | <0.001 | |
Diabetes mellitus | 2317 (11.2) | 25 (12.1) | 2292 (11.2) | 0.68 | |
Non‑HCC malignant tumors | 475 (2.3) | 9 (4.4) | 466 (2.3) | 0.047 | |
Renal disease | 723 (3.5) | 4 (1.9) | 719 (3.5) | 0.22 | |
Concomitant medications other than for RA | 11 817 (57.2) | 161 (78.2) | 11 656 (57) | <0.001 | |
ALT, IU/l | 82 (51–132) | 66.5 (38–134) | 82 (51–132) | 0.17 | |
Albumin, g/dl | 3.9 (3.5–4) | 3.7 (3.5–4) | 3.9 (3.5–4) | 0.03 | |
Bilirubin, mg/dl | 0.9 (0.6–1) | 0.8 (0.7–1) | 0.9 (0.6–1) | 0.37 | |
Hemoglobin, g/dl | 14.2 (13–15) | 13.6 (12.7–14) | 14.2 (13–15) | 0.02 | |
Platelets, × 1000/μl | 124 (85–174) | 153 (105–210) | 124 (85–173) | 0.01 | |
Creatinine, mg/dl | 0.8 (0.7–1) | 0.7 (0.6–1) | 0.8 (0.7–1) | 0.13 | |
HCV RNA, × 106 IU/ml | 0.9 (0.3–2.4) | 0.8 (0.3–1.8) | 0.9 (0.3–2.4) | 0.9 | |
The patients with RA were more likely to present with comorbid conditions other than RA, including arterial hypertension (47.1% vs 31.2%; P <0.001) and non‑HCC malignant tumors (4.4% vs 2.3%; P = 0.047), as compared with the non‑AID group. They were also more often on concomitant medications (other than RA treatment; 78.2% vs 57%, respectively; P <0.001; Table 1).
The medications most commonly used for RA treatment were glucocorticoids (27.2%), methotrexate (MTX; 6.8%), or a combination of both drugs (6.8%; Figure 2). Notably, 36.9% of the patients were not on any disease‑modifying therapy for RA due to remission of the disease at the time of DAA therapy initiation.

Abbreviations: CQ, chloroquine; CsA, cyclosporine; ECU, eculizumab; ETN, etanercept; GC, glucocorticoids; HCQ, hydroxychloroquine; LEF, leflunomide; MTX, methotrexate; SSZ, sulfasalazine
Among laboratory parameters, the patients with RA had significantly lower serum albumin and hemoglobin concentrations, as well as significantly higher platelet counts. Baseline HCV viral load, bilirubin, and creatinine concentrations were comparable in both groups (Table 1).
The predominant HCV genotype (GT) in the entire population was GT1b (74.2%), with a significantly higher prevalence among the patients with RA than the non‑AID individuals. Only 2 patients in the RA group (1%) were infected with GT1a, as compared with 4.9% in the non‑AID group (P = 0.001). The percentage of patients infected with GT3 was also lower in the RA group, but the difference did not reach significance (8.9% vs 13.5%; P = 0.07). Advanced liver fibrosis and cirrhosis (F3–F4) were less common in the patients with RA than in the non‑AID population (30.3% vs 38.4%; P = 0.02). HIV coinfection was significantly less frequent in the RA group (Table 2).
Parameter | All patients (n = 20 645) | RA group (n = 206) | Non‑AID group (n = 20 439) | P value | ||
Data are presented as number (percentage).
| ||||||
Genotype | Patients with available data, n | 19 044 | 191 | 18 853 | – | |
1a | 933 (4.9) | 2 (1) | 931 (4.9) | <0.001 | ||
1b | 14 122 (74.2) | 160 (83.8) | 13 962 (74.1) | <0.001 | ||
1 | 396 (2.1) | 4 (2.1) | 392 (2.1) | 0.8 | ||
2 | 62 (0.3) | 0 | 62 (0.3) | >0.99 | ||
3 | 2556 (13.4) | 17 (8.9) | 2539 (13.5) | 0.07 | ||
4 | 968 (5.1) | 8 (4.2) | 960 (5.1) | 0.57 | ||
5 | 1 (<0.001) | 0 | 1 (<0.001) | >0.99 | ||
6 | 6 (<0.001) | 0 | 6 (<0.001) | >0.99 | ||
Liver fibrosis stage | Patients with available data, n | 19 993 | 198 | 19 795 | – | |
F0 | 605 (3) | 7 (3.5) | 598 (3) | 0.67 | ||
F1 | 7882 (39.4) | 88 (44.4) | 7794 (39.4) | 0.15 | ||
F2 | 3843 (19.3) | 43 (21.8) | 3800 (19.2) | 0.37 | ||
F3 | 2720 (13.6) | 19 (9.6) | 2701 (13.6) | 0.1 | ||
F4 | 4943 (24.7) | 41 (20.7) | 4902 (24.8) | 0.19 | ||
F3–F4 | 7663 (38.3) | 60 (30.3) | 7603 (38.4) | 0.02 | ||
Child–Pugh score B/C in the patients with F4 | 533 (10.8) | 1 (2.4) | 532 (10.9) | 0.12 | ||
History of hepatic decompensation (ascites and / or encephalopathy) | 626 (3) | 5 (2.4) | 621 (3) | 0.61 | ||
Documented esophageal varices in the patients with F4 | 1140 (23.1) | 10 (24.4) | 1130 (23.1) | 0.82 | ||
Hepatic decompensation at the start of therapy (ascites and / or encephalopathy) | 397 (1.9) | 5 (2.4) | 392 (1.9) | 0.6 | ||
History of HCC | 346 (1.7) | 4 (1.9) | 342 (1.7) | 0.78 | ||
Coinfections | HIV coinfection | 1347 (6.5) | 1 (0.5) | 1346 (6.6) | <0.001 | |
HBV coinfection (HBsAg+) | 206 (1) | 0 | 206 (1) | 0.28 | ||
Treatment characteristics
In both groups, most patients were treatment‑naive. The most common therapeutic approach in the RA group consisted of genotype‑specific regimens with the most frequent option of ombitasvir / paritaprevir / ritonavir with or without dasabuvir and with or without RBV (20.6%). However, the sofosbuvir / ledipasvir (SOF/LDV) ± RBV regimen was more frequent in the RA group (P = 0.01). In the non‑AID group, pangenotypic regimens were the most frequently used treatment approach, with glecaprevir / pibrentasvir being the predominant regimen (29.3%); it was also used more often in this group than in the RA patients (P = 0.003; Table 3).
Parameter | All patients (n = 20 645) | RA group (n = 206) | Non‑AID group (n = 20 439) | P value |
Data are presented as number (percentage).
Abbreviations: RBV, ribavirin; others, see Figure 1 | ||||
History of antiviral treatment | ||||
Treatment‑naive | 17 093 (82.8) | 168 (81.6) | 16 925 (82.8) | 0.62 |
Treatment‑experienced | 3552 (17.2) | 38 (18.4) | 3504 (17.2) | 0.62 |
Current treatment regimen | ||||
Current RBV‑containing regimens | 2546 (12.3) | 27 (13.1) | 2519 (12.3) | 0.73 |
Genotype‑specific treatment regimens | 9401 (45.5) | 112 (54.4) | 9289 (45.4) | 0.01 |
Pangenotypic regimens | 11 244 (54.5) | 94 (45.6) | 11 150 (54.6) | 0.01 |
Treatment effectiveness
The effectiveness of DAA therapy in the patients with RA was very high, with SVR reaching 96.2% in the intention‑to‑treat analysis. Six patients (4 women) were lost to follow‑up. The majority of this group was infected with GT1b (n = 4) and was treatment‑naive (n = 5); 1 patient had liver cirrhosis. Most of them completed therapy according to schedule (n = 5). One patient died. After exclusion of these patients, SVR increased to 98.4% in the per‑protocol analysis. These SVR rates were comparable in both groups regardless of sex, HCV genotype, stage of liver fibrosis, and the presence of cirrhosis (Figure 3A and 3B).

Abbreviations: see Figure 1
In univariable analysis of patients with RA, those who achieved a treatment response did not differ significantly from those who did not respond to therapy with respect to the analyzed clinical and virologic variables. Only a history of HCC occurred significantly more often in the nonresponders. In the group of patients with RA, only 3 individuals failed to respond to treatment, including 2 women; all had infection with GT1b and were treatment‑naive. Liver cirrhosis was present in 2 of these patients (Table 4).
Patient | Age, y | GT | F, CP | Current regimen | History of previous therapy | Baseline HCV RNA, × 106 IU/ml | Treatment course | EOT |
Woman 1 | 63 | 1b | 2, A | VEL/SOF | Treatment‑naive | 2.21 | According to schedule | TND |
Woman 2 | 65 | 1b | 4, A | LDV/SOF+RBV | Treatment‑naive | 0.78 | According to schedule | TND |
Man 1 | 53 | 1b | 4, A | LDV/SOF | Treatment‑naive | 1.61 | According to schedule | TD |
We compared the patients who achieved and those who did not achieve a virologic response to DAA therapy based on available data on both the degree of liver fibrosis and HCV genotype (n = 17 623; Supplementary material, Table S1). In the analyzed population, the patients who failed to achieve an SVR were more often male (P <0.001) and had higher BMI (P <0.001). The patients who responded to DAA treatment received genotype‑specific regimens significantly more commonly. In addition, the nonresponder group significantly more often used medications other than those prescribed for RA.
The prevalence of HCC was higher among the nonresponders than in those in whom therapy was successful (3.8% vs 1.4%; P <0.001). The occurrence of RA, arterial hypertension, diabetes mellitus, chronic kidney disease, and malignancies other than HCC was comparable between the 2 groups and did not reach significance. The patients who did not respond to DAA therapy were more often treatment‑experienced (25.5% vs 18.3%; P <0.001). Moreover, among the nonresponders, a history of hepatic decompensation and the presence of decompensated cirrhosis at treatment initiation were more frequently observed (P <0.001).
In the nonresponder group, as compared with the responders, GT3 infection (32.7% vs 12.5%; P <0.001) and liver cirrhosis (F4; 50.5% vs 23.8%; P <0.001) were more prevalent. In contrast, among the patients who achieved a virologic response, GT1b infection (75% vs 58.4%; P <0.001) and low‑grade fibrosis (F1; 40.2% vs 23.6%; P <0.001) were more common. In the subgroup of patients with liver cirrhosis (F4), the nonresponders were more often classified as CP class B or C (22.9% vs 9.2%; P <0.001) and more frequently had esophageal varices (P <0.001).
Logistic regression analysis assessing virologic failure in the entire cohort of patients infected with HCV identified the following significant predictive factors: male sex (OR, 2.3), GT3 infection (OR, 2.9), a history of prior antiviral therapy (OR, 1.4), a history of esophageal varices (OR, 2), cirrhosis (OR, 2), use of medications other than those for RA (OR, 1.3), and CP class B or C (OR, 2.3; Figure 4).

Abbreviations: OR, odds ratio; SVR, sustained virologic response; others, see Figure 1 and Table 1
Treatment safety
In both groups, the proportion of patients who completed antiviral therapy as planned was very high and comparable. We found no significant differences between the analyzed groups in terms of serious adverse events leading to treatment discontinuation or in treatment cessation due to hepatic decompensation. In contrast, the proportion of patients with at least 1 adverse event was significantly higher in the RA group. Mortality was similar across the groups, and none of the reported deaths in either group were considered related to antiviral therapy (Supplementary material, Table S2).
Discussion
This study provides a comprehensive analysis of the clinical characteristics of patients with RA infected with HCV, based on data derived from a nationwide, multicenter database. Data were collected over 10 years, allowing for a robust and in‑depth assessment of both the safety and effectiveness of DAA therapies in the analyzed population. To the best of our knowledge, this is the largest study to comprehensively evaluate the treatment of CHC using various DAA regimens in this specific patient group.
In the present study, all patients received regimens without interferon (IFN), which is an important consideration when interpreting our results in the context of the existing literature. Of note, several publications involving large patient cohorts have reported that IFN therapy may induce inflammatory arthritis, often accompanied by positivity for rheumatoid factor and / or antinuclear antibodies, with symptoms resolving after treatment discontinuation. Notably, the exclusive use of DAA therapy in our study allowed us to avoid the potential confounding effects of IFN on AID activity, including RA.23
In the analyzed cohort, the patients with RA accounted for 1% of the total study population, which is consistent with the global prevalence of RA estimated at approximately 1%, as well as with data from the Global Burden of Diseases, Injuries, and Risk Factors Study 2021, which reported that approximately 17.6 million individuals worldwide are affected by RA.24-26 However, the prevalence of HCV infection in this population may be underestimated due to infrequent or nonsystematic HCV screening, particularly in patients without overt clinical indications for testing.27 Patients with RA in our study were significantly older, with more than 84.5% being over 50 years of age. Women predominated markedly in this group, accounting for 79.6% of the population, which aligns with the typical epidemiological profile of RA as a disease most commonly affecting women over the age of 40 years.28,29
In the analyzed population, the patients with RA significantly less frequently exhibited advanced stages of liver fibrosis and cirrhosis. Fibrosis stages F3–F4 were identified in 30.3% of the individuals with RA, as compared with 38.4% of those without RA (P = 0.02). In addition, episodes of liver decompensation, ascites, and hepatic encephalopathy were less frequent in the RA population. These findings are consistent with reports from other authors, including the results of a clinical study that included 24 245 patients with RA and an equal number of matched controls without RA. In that analysis, the presence of RA was associated with a 16% reduction in the risk of cirrhosis‑related complications.30,31
Based on the conducted analyses, the patients with RA were more frequently diagnosed with HCC. The relationship between HCC occurrence and RA can be explained by several potential pathophysiological mechanisms.32 Importantly, the individuals with RA also developed malignancies other than HCC more often (P <0.047). Available data indicate that systemic rheumatic diseases, including RA, may be associated with an increased risk of malignancies, particularly those of lymphoproliferative origin.33,34 Chronic inflammation may exert a complex influence on carcinogenesis by impairing tumor suppressive mechanisms and inducing premature cellular senescence.32
The coexistence of RA in individuals infected with HIV remains relatively rare. In the analyzed population, HIV infection was significantly more frequent among the patients without RA than those diagnosed with RA (6.6% vs 0.5%), which is in line with the results of previous observational studies.35,36 Nevertheless, isolated cases of RA development after initiation of antiretroviral therapy have been described in the literature and attributed to immune reconstitution inflammatory syndrome.36,37
The medications most commonly used in the treatment of RA were MTX (6.8%), glucocorticoids (27.2%), and their combination (6.8%). In addition, leflunomide, chloroquine, sulfasalazine, hydroxychloroquine, cyclosporine, eculizumab, etanercept, azathioprine, or combinations of these agents were used. This treatment pattern is consistent with current RA management guidelines (EULAR).38 However, one should note that as many as 36.9% of the patients did not receive any disease‑modifying therapy aimed at achieving clinical remission of RA. In our cohort, the frequency of MTX use was lower than expected based on general RA treatment practices in Poland. In a previous study of 1957 Polish RA patients, 91% had received MTX at some point, and for 61% it was the first synthetic disease‑modifying antirheumatic drug used.39 The lower frequency of this specific intervention observed in our study likely reflects caution in prescribing MTX to patients with CHC due to concerns about hepatotoxicity. It is also possible, although highly unlikely, that this lower frequency is in part related to incomplete reporting of MTX use in medical records.
In the analyzed group of patients with RA, the presence of comorbidities was more frequent, as compared with the non‑AID group (P <0.001). The most commonly diagnosed concomitant condition was arterial hypertension, the prevalence of which was markedly higher among the patients with RA (P <0.001). Furthermore, the patients with RA were more likely to use medications other than those prescribed for the underlying rheumatic disease (P <0.001), which may reflect a greater burden of multimorbidity in this population, probably related to this group’s more advanced age.
These findings are consistent with reports from other authors, indicating that chronic immune system activation and persistent inflammation promote the development of additional diseases, particularly cardiovascular conditions.40 The chronic inflammatory process observed in RA may lead to endothelial dysfunction, impaired vascular regulation, and accelerated atherosclerosis, thereby increasing the risk of arterial hypertension.41
Analysis of the distribution of HCV genotypes showed significant differences between the study groups. In the overall population, GT1b was the most frequently identified, whereas GT3 was significantly more prevalent in the non‑AID group. Previous reports regarding the relationship between HCV genotypes and the risk of RA development remain inconclusive and often contradictory.42-44 According to the current state of knowledge, there is no clear evidence confirming a direct association between RA prevalence and a specific HCV genotype, underscoring the need for further research in this area.
While the use of IFN‑based treatment regimens has been limited in the past due to low efficacy and serious safety concerns, the current generation of DAA therapies achieves high SVR rates, is much better tolerated, and is a safe and effective option even for patients with concomitant rheumatic or autoimmune conditions.45
Observational studies conducted among patients with chronic HCV and RA have demonstrated that DAA therapy inhibits viral replication, reduces RA activity, and does not cause serious adverse events. Unlike IFN, DAAs indirectly benefit RA by reducing inflammation through the elimination of HCV.46
Assessment of antiviral treatment effectiveness showed only slightly less favorable outcomes in the patients with RA than in those without this comorbidity. The SVR rate was 96.2% in the RA group and 94.5% in the non‑AID group, with no difference in the intention‑to‑treat analysis (P = 0.3).
Subgroup analyses comparing patients with and without virologic response, regardless of RA status, showed that male sex, GT3 infection, a history of HCC, prior liver decompensation, the presence of decompensation at treatment initiation, and advanced liver fibrosis were associated with virologic failure. The diagnosis of RA itself was not significantly associated with treatment response. These findings are consistent with previous reports highlighting the critical role of liver disease severity in determining the effectiveness of modern antiviral therapies.46-48
In patients with concomitant RA and HCV infection, advanced liver disease may nevertheless limit the ability to achieve full clinical control of RA following viral eradication, potentially due to persistent inflammation and restrictions on the use of intensive immunosuppressive therapy. However, available data indicate that RA itself does not negatively affect the fundamental virologic efficacy of HCV treatment—a finding confirmed by previous analyses.46,47
In multivariable analysis including the entire study population, independent predictors of virologic failure were male sex, GT3 infection, advanced fibrosis (F4), use of concomitant treatment, a history of esophageal varices, CP class B or C, and prior unsuccessful antiviral therapy. RA was not an independent risk factor for virologic failure, which is consistent with available literature data.49,50
In the present study, the overall safety profile of DAA‑based therapies was assessed as favorable due to the low rate of premature treatment discontinuation and good tolerability of the applied regimens. These results are in line with reports on the safety of DAA therapies in patient populations burdened with various comorbidities.51 We found no significant differences between the groups in serious adverse events or mortality. Mild events were more frequent in the RA patients, consistent with the findings of the ORAL (Oral Rheumatoid Arthritis) Surveillance trial, linking higher disease activity to an increased risk of adverse events.51
Limitations
When interpreting the results of this study, several important limitations should be taken into account. The key limitation that should be acknowledged is the paucity of data on RA. We cannot rule out that RA patients treated with currently recommended agents, in particular those with extensive joint involvement, differ from the group defined using medical records in our study. We based the diagnosis of RA on medical records and clinical history rather than on the uniform application of validated classification criteria, such as the ACR/EULAR criteria. However, to our best knowledge, the diagnosis made by rheumatologists was based on validated criteria. Secondly, the retrospective nature of the study and its reliance on actual data may introduce systematic errors leading to an underestimation of the frequency of adverse events. Thirdly, detailed data on RA disease activity, duration, serological status, and extra‑articular manifestations were not available. Fourthly, information on past immunosuppressive therapy was limited, and we only had information on the medications taken during DAA therapy. It should be added that although we had data on steroid and MTX use, data on total treatment duration, cumulative doses, and changes in immunosuppressive therapy before DAA treatment were incomplete. Therefore, it was not possible to conduct a more detailed analysis of the potential impact of different RA treatment strategies on antiviral efficacy and safety. Finally, the RA subgroup represented a relatively small proportion of the overall cohort, and the number of virologic failures within this group was very low. As a result, the statistical power to detect subtle differences in treatment effectiveness or to perform robust subgroup analyses within the RA population was limited.
Despite these restrictions, the study has some significant advantages, supported by its large sample size and data collection from 22 specialized hepatology centers, which enhances the representativeness of the results. Furthermore, detailed patient characterization enabled thorough subgroup analyses, and the low proportion of patients who were lost to follow‑up reduced the risk of selection bias. All these factors, taken together, increase the credibility of the findings and support their broad generalizability to clinical populations treated with DAA‑based regimens.
Conclusions
Patients with RA constitute a small but distinct subgroup among individuals treated for CHC. Despite being older and burdened with more comorbidities, the RA patients had similar liver disease severity and responded to DAA therapy as effectively and safely as the individuals without RA. Multivariable analysis showed that advanced liver disease, presence of esophageal varices, male sex, GT3 infection, prior antiviral therapy, and use of non‑RA medications—but not RA itself—were independent predictors of virologic failure. These findings indicate that RA does not compromise DAA treatment outcomes.
- World Health Organization. Rheumatoid arthritis. https://www.who.int/news‑room/fact‑sheets/detail/rheumatoid‑arthritis. Accessed January 10, 2026.
- Milosevic I, Todorovic N, Filipovic A, et al. HCV and HCC tango—deciphering the intricate dance of disease: a review article. Int J Mol Sci. 2023; 24: 16048. | Crossref
- Martinello M, Solomon SS, Terrault NA, Dore GJ. Hepatitis C. Lancet. 2023; 402: 1085‑1096. | Crossref
- World Health Organization. Hepatitis C. https://www.who.int/news‑room/fact‑sheets/detail/hepatitis‑c. Accessed January 10, 2026.
- Rosenthal E, Cacoub P. Extrahepatic manifestations in chronic hepatitis C virus carriers. Lupus. 2015; 24: 469‑482. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION