Potassium-competitive acid blockers for erosive reflux disease and stress ulcer prophylaxis: a narrative review
Key words: erosive esophagitis, gastroesophageal reflux disease, potassium-competitive acid blocker, stress ulcer prophylaxis, zastaprazan

 CC BY 4.0
CC BY 4.0
Potassium-competitive acid blockers for erosive reflux disease and stress ulcer prophylaxis: a narrative review
Potassium‑competitive acid blockers (P‑CABs) are the first mechanistically distinct oral acid suppressants to challenge proton pump inhibitors (PPIs) in routine practice. By reversibly inhibiting gastric H+/K+-adenosinetriphosphatase without requiring acid activation, they provide rapid onset of action, durable 24‑hour acid control, and decreased dependence on meal timing and CYP2C19 variability. These pharmacologic features are clinically relevant in acid‑related disorders, but the clinical evidence is not uniform across individual compounds. Within the class, the most extensive efficacy and safety data have been collected for vonoprazan, whereas newer agents, including zastaprazan, remain supported by a more limited evidence base. In erosive esophagitis, randomized trials indicate that P‑CABs are effective acid suppressants, but compound‑specific conclusions are more appropriate than broad assumptions of interchangeable class effects. For zastaprazan specifically, phase 3 data show that 20 mg is noninferior to esomeprazole 40 mg at week 8, with higher week 4 healing rates in a predominantly low‑grade population. In contrast, no clinical trials have directly evaluated any P‑CAB for stress ulcer prophylaxis in critically ill adults. Current intensive care unit guidelines continue to support PPIs or histamine‑2 receptor antagonists in patients at a high risk of stress‑related gastrointestinal bleeding, and pantoprazole remains the best‑established benchmark. This review integrates mechanistic, pharmacokinetic, efficacy, safety, regulatory, and guideline data relevant to P‑CABs, with particular attention to zastaprazan, while distinguishing compound‑specific findings from broader class‑level considerations.
Introduction
Gastroesophageal reflux disease (GERD) remains one of the most common chronic gastrointestinal disorders, and erosive esophagitis (EE) is a clinically important phenotype, because it is linked to symptom burden, impaired quality of life, recurrent disease, and long‑term complications.1,2 For more than 3 decades, proton pump inhibitors (PPIs) have been the dominant pharmacologic strategy for acid suppression. Yet, their limitations are well recognized: they require acid‑mediated activation, often need meal‑time–coordinated administration, achieve maximal effect only after repeated dosing, and may provide suboptimal control of nocturnal acid secretion or inconsistent efficacy in patients with rapid CYP2C19 metabolism.1-4 These limitations help explain persistent unmet needs in rapid symptom relief, severe EE, and PPI‑refractory disease.2-4
Potassium‑competitive acid blockers (P‑CABs) have changed this landscape. Unlike PPIs, they inhibit the final step of acid secretion without prior acid activation, and therefore have the potential to provide faster and more predictable acid suppression from the first dose onward.5-8 Vonoprazan established the clinical credibility of the class, and newer compounds, including tegoprazan, fexuprazan, and more recently zastaprazan (JP‑1366; marketed as JAQBO in South Korea) have expanded the development pipeline.6,8-10
The central question is no longer whether P‑CABs are pharmacologically interesting, but where they should be positioned clinically. That question has 2 very different answers depending on the indication. In EE, the evidence base is now substantial and increasingly international.8,9,11,12 In stress ulcer prophylaxis (SUP), by contrast, the pharmacologic rationale is attractive but direct evidence remains essentially scarce.13,14 The purpose of this review is to synthesize the current evidence on P‑CABs with a particular focus on zastaprazan, to compare the class with PPIs in erosive reflux disease, and to critically assess whether the same pharmacology can legitimately be extrapolated to the prevention of stress‑related upper gastrointestinal bleeding in critically ill adults. Because the available evidence is uneven across individual P‑CABs, this review distinguishes between class‑level pharmacologic characteristics and compound‑specific clinical evidence, particularly when discussing vonoprazan and newer agents, such as zastaprazan. This distinction is also important from a practical standpoint, because despite growing international evidence, P‑CABs are not yet established in routine European Union clinical practice, which limits the immediate applicability of these data to European prescribing settings.
Methods
This article was prepared as a structured narrative review rather than as a formal systematic review or meta‑analysis. The aim was to provide a clinically focused synthesis of the evidence relevant to P‑CABs, with particular attention to EE, the emerging evidence base for zastaprazan, and the possible relevance of this class to SUP in critically ill adults. The evidence considered for this review was appraised through March 8, 2026.
Focused literature searches were conducted in PubMed/MEDLINE, Embase, Scopus, and the Cochrane Library from database inception through March 8, 2026, using database‑adapted terms related to P‑CABs, zastaprazan, vonoprazan, tegoprazan, fexuprazan, EE, reflux disease, pharmacology, pharmacokinetics, pharmacodynamics, SUP, intensive care, and critical illness. Additional targeted searches of ClinicalTrials.gov, regulatory documents, prescribing information, guideline statements, and reference lists of key articles were performed. Sources were selected pragmatically for relevance to the clinical questions of interest, with emphasis on peer‑reviewed primary studies, randomized trials where available, pharmacokinetic / pharmacodynamic studies, major regulatory materials, and professional society guidelines. The full search strategy for all databases and targeted sources is provided in Supplementary material, Table S1. As evidence specific to zastaprazan remains limited, selected data from other P‑CABs were included cautiously to provide class context and pharmacologic plausibility, but not as direct proof of compound‑specific effects. No formal study quality scoring or quantitative synthesis was performed. For the specific question of SUP in critically ill adults, the authors did not identify published clinical trials directly evaluating any P‑CAB.
Pharmacologic rationale for potassium‑competitive acid blockers: why the class matters
P‑CABs and PPIs both affect the function of gastric H+/K+-adenosinetriphosphatase (ATPase), but they differ in the ways that have practical clinical consequences. According to current United States Food and Drug Administration (FDA) labeling, vonoprazan suppresses basal and stimulated gastric acid secretion by inhibiting the H+/K+-ATPase in a potassium‑competitive, noncovalent, and reversible manner; it does not require activation by acid and may concentrate in parietal cells in both resting and stimulated states.15,16 The onset of antisecretory activity occurs within 2–3 hours after a single 20‑mg dose, and elevated intragastric pH is maintained for more than 24 hours.16
These class features help explain why P‑CABs can outperform PPIs in early pharmacodynamic comparisons. In healthy CYP2C19 extensive metabolizers, vonoprazan 20 mg produced significantly stronger acid suppression than esomeprazole 20 mg or rabeprazole 10 mg on both day 1 and day 7, demonstrating a rapid first‑dose effect that has been difficult to achieve with PPIs.17 In a night‑time crossover study, both tegoprazan and vonoprazan provided greater nocturnal pH control than esomeprazole, and their acid‑suppressive effects were not dependent on CYP2C19 phenotype to the same degree.18
Zastaprazan fits this mechanistic profile well. In a phase 1 randomized study in healthy participants, zastaprazan was rapidly absorbed, with peak plasma concentrations within approximately 2 hours and an elimination half‑life of about 6–10 hours.4 The percentage of time during which intragastric pH remained above 4 reached 85.19% with 20 mg and 91.84% with 40 mg, as compared with 72.06% for esomeprazole 40 mg.19 Mean gastric pH remained above 4 for most of the 24‑hour observation period at doses of 20 mg or greater, and the 40‑mg dose yielded stronger night‑time acid suppression than esomeprazole 40 mg.19 A dedicated food‑effect cohort showed that a high‑fat meal lowered peak plasma concentration but increased overall exposure and prolonged the antisecretory effect, arguing against a clinically important dependence on premeal dosing.19,20
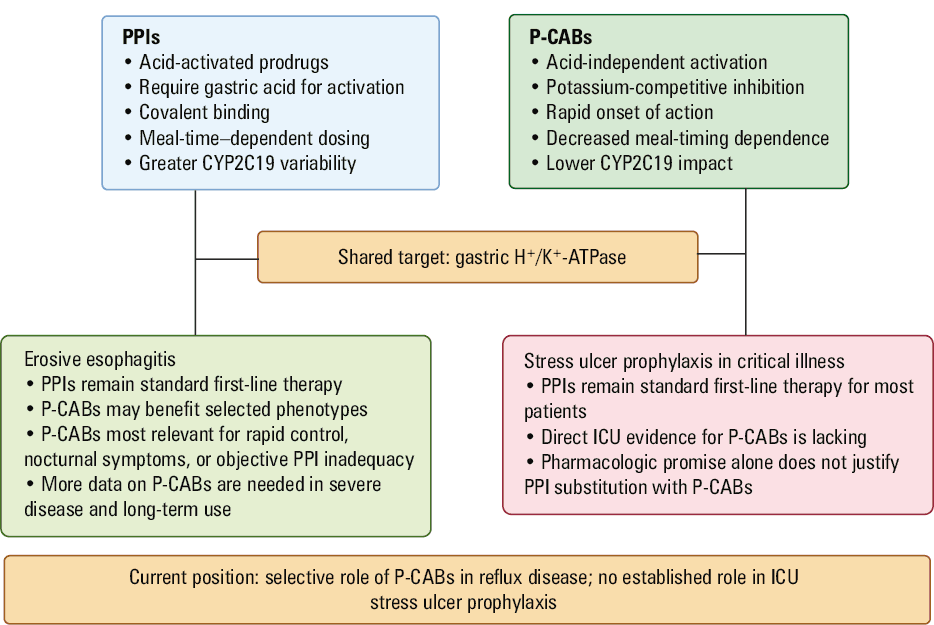
Mechanistically, zastaprazan also appears less vulnerable to CYP2C19‑driven variability than many PPIs. In vitro work suggests predominant metabolism via CYP3A4/3A5, with only minor contributions from CYP1A2, CYP2C8, CYP2C9, CYP2C19, and CYP2D6; major transporter effects appear limited.21 A population pharmacokinetic analysis in healthy volunteers and patients with GERD likewise found no clinically meaningful effect of CYP2C19 phenotype on zastaprazan exposure.19 Collectively, these data support the view that P‑CABs are not merely stronger PPIs, but pharmacologically distinct agents with potentially superior real‑world consistency (Table 1).8,22,23 Their current clinical positioning relative to PPIs in reflux disease and SUP is summarized in Figure 1.
Feature | P‑CABs | PPIs | Likely clinical implication |
Abbreviations: ATPase, adenosinetriphosphatase; P‑CAB, potassium‑competitive acid blocker; PPI, proton pump inhibitor | |||
Requirement for activation | Active without prior acid activation | Prodrugs requiring acid activation in the secretory canaliculus | More rapid and predictable early acid suppression with P‑CABs |
Binding to H+/K+-ATPase | Potassium‑competitive, reversible inhibition | Covalent inhibition after activation | Different onset and offset profiles |
Dependence on meal timing | Generally less dependent on premeal dosing | Typically administered before meals | Potential advantage when dosing adherence is inconsistent |
Early and nocturnal acid control | Stronger day 1 and night‑time suppression | Often slower early effect and less consistent nocturnal control | Potential relevance in rapid symptom relief and nocturnal symptom phenotypes |
CYP2C19 influence | Lower for agents such as zastaprazan, vonoprazan, and tegoprazan | Clinically relevant for several PPIs | More consistent drug exposure and response across genotypes |
Most relevant clinical positioning | Selected patients needing rapid control or with suboptimal response to optimized PPI therapy | Standard first‑line therapy for most acid‑related indications | Use should be guided by clinical phenotype and supporting evidence rather than assumed class superiority |
Abbreviations: ICU, intensive care unit; others, see Table 1
Zastaprazan and class‑level clinical evidence in erosive esophagitis
The clinical evidence for P‑CABs in EE is not equally mature across individual compounds. The most robust randomized and maintenance data are currently derived from vonoprazan, whereas the clinical evidence for zastaprazan remains more limited and is anchored primarily in a single phase 3 trial supported by early pharmacokinetic and pharmacodynamic studies11. Accordingly, findings from other P‑CABs are useful for class context and biologic plausibility, but they should not be interpreted as direct proof of equivalent efficacy for zastaprazan.
For zastaprazan specifically, the key study is a multicenter, randomized, double‑blind phase 3 trial of 300 patients with endoscopically confirmed EE comparing zastaprazan 20 mg once daily with esomeprazole 40 mg once daily for up to 8 weeks.9 In the full analysis set, cumulative healing at week 8 was 97.92% with zastaprazan and 94.93% with esomeprazole, meeting the criterion for noninferiority. Notably, week 4 healing was markedly better with zastaprazan (95.14% vs 87.68%; P = 0.026).9 However, symptom response, GERD‑related quality of life, and overall safety did not differ significantly between the groups. Serum gastrin increased during treatment in both groups and declined after treatment cessation. Importantly, the study population consisted predominantly of patients with low‑grade erosive disease, which limits direct extrapolation to more severe Los Angeles (LA) grade C/D esophagitis.9
The broader class literature indicates that the zastaprazan findings are biologically plausible within the pharmacologic profile of P‑CABs, but the strongest supporting clinical evidence comes from studies on vonoprazan. In a pivotal Japanese trial, vonoprazan 20 mg was noninferior to lansoprazole 30 mg for healing EE by week 8 (99% vs 95.5%), and appeared particularly effective in patients with more severe disease and in CYP2C19 extensive metabolizers.24 In a subsequent 24‑week maintenance trial, recurrence was found in 16.8% of the patients receiving lansoprazole 15 mg, as compared with 5.1% and 2% of those receiving vonoprazan 10 mg and 20 mg, respectively.25 More recently, a randomized trial conducted in the United States and Europe showed that vonoprazan was noninferior, and in some analyses superior, to lansoprazole for healing and maintenance of healing, with the greatest benefit observed in more severe EE.11
Evidence from other compounds remains supportive but still more limited than for vonoprazan. Tegoprazan and fexuprazan each achieved noninferior healing as compared with esomeprazole in phase 3 trials, with broadly comparable symptom outcomes and tolerability.26,27 These studies support the view that potent acid suppression is a reproducible feature of the class, but they do not establish therapeutic interchangeability among individual P‑CABs or validate compound‑specific outcomes for zastaprazan.
At the same time, superiority should not be assumed across all GERD phenotypes. In a European proof‑of‑concept phase 2 trial among symptomatic patients with partial response to a healing dose of esomeprazole, vonoprazan 20 mg and 40 mg did not demonstrate significant efficacy advantages over esomeprazole 40 mg over 4 weeks.8 This finding is clinically important because it cautions against extrapolating EE data to nonerosive reflux disease or symptom‑predominant reflux syndromes.
Early symptom relief is nonetheless one of the most clinically appealing attributes of the class. In a randomized study of patients with EE, heartburn was relieved sooner with vonoprazan than with lansoprazole, complete heartburn relief on day 1 occurred in 31.3% vs 12.5%, respectively, and nocturnal heartburn relief was also more frequent with vonoprazan.28 Although the phase 3 zastaprazan study did not show a between‑group difference in symptom response, its superior week 4 mucosal healing and favorable pharmacodynamic profile leave open the possibility that certain symptom phenotypes, particularly those driven by nocturnal acid exposure or inadequate first‑dose control may still benefit in practice.9,19 Current evidence landscape for zastaprazan, reflux disease, and SUP is summarized in Table 2.
Domain | Evidence base | What can reasonably be concluded | What remains uncertain |
Zastaprazan pharmacokinetics / pharmacodynamics | Early‑phase pharmacokinetics / pharmacodynamics studies19 | Zastaprazan shows rapid absorption and sustained 24‑hour acid suppression, with preserved activity under fed conditions | Findings are based mainly on healthy‑volunteer studies and physiological surrogate end points |
Zastaprazan efficacy in EE | Phase 3 comparative clinical trial data9 | Healing efficacy appears noninferior to esomeprazole at 8 weeks, with a possible earlier healing advantage | Current evidence is driven largely by lower‑grade EE, and superiority for symptom outcomes has not been clearly established |
Vonoprazan‑dominant evidence for severe and maintenance EE | Randomized trials and maintenance studies with other agents in the class11,31,32 | P‑CABs as a class appear effective for mucosal healing and maintenance, including in more severe disease | Extrapolation from class data to zastaprazan should remain cautious until more compound‑specific evidence is available |
PPI‑refractory reflux disease | Small mechanistic and clinical studies33,34 | P‑CABs may offer benefit in selected patients with objectively documented inadequate response to PPI therapy | The evidence base remains limited, regionally concentrated, and insufficient for broad generalization |
International generalizability | Emerging non‑Asian trial experience11,35 | The evidence base is no longer exclusively Asian and is becoming more internationally relevant | Broader geographic validation is still needed, particularly for newer P‑CABs, such as zastaprazan |
SUP: guideline position | Contemporary critical care guidelines14 | Current guideline‑supported prophylaxis remains centered on PPIs or H2RAs in high‑risk critically ill adults | P‑CABs do not currently have an established role in guideline‑based ICU practice |
SUP: outcome benchmark | Contemporary ICU clinical trials with established acid suppression strategies30 | Any future role for P‑CABs in SUP will need to match or exceed the outcome standard already established for current therapy | Direct ICU outcome data for P‑CABs are currently lacking |
Safety, tolerability, and long‑term considerations
For any class that achieves potent, durable acid suppression, efficacy must be balanced against biologic and long‑term safety considerations. The short‑term zastaprazan data are reassuring. In phase 1, single doses up to 60 mg and multiple doses up to 40 mg were safe and well tolerated in healthy volunteers.19 In phase 3 EE, adverse‑event profiles were similar between zastaprazan and esomeprazole, with no major signal suggesting an unfavorable short‑term tolerability profile.9
Hypergastrinemia is the most consistent biologic consequence of strong acid suppression with P‑CABs. In the zastaprazan phase 3 trial, serum gastrin increased during therapy and declined after treatment cessation.9 Class experience indicates that this effect is expected rather than unique. Current FDA labeling for vonoprazan notes increased serum gastrin concentrations during treatment, return toward normal values within 4 weeks after discontinuation, and histologic changes consistent with sustained acid suppression, including hyperplasia of parietal and G‑cells in biopsy specimens collected for up to 260 weeks, without neoplastic changes observed in the labeled dataset.15,16
Long‑term observational reassurance for the class is currently driven predominantly by vonoprazan, and these data should not be interpreted as establishing an equivalent long‑term safety profile for newer agents, such as zastaprazan. In the 5‑year VISION study (Vonoprazan Study in Patients with Erosive Esophagitis to Evaluate Long‑term Safety)36, median gastrin concentrations, parietal cell hyperplasia, and foveolar hyperplasia were greater with vonoprazan than with lansoprazole, but there was no increased risk of malignant epithelial cell alterations or gastric neuroendocrine tumors over the study period. This is reassuring, but it should not be used to claim established long‑term safety for newer agents such as zastaprazan, for which comparable datasets do not yet exist.
Other safety questions are best viewed as class‑labeled or class‑plausible rather than zastaprazan‑specific at present. Vonoprazan labeling includes warnings familiar from other powerful acid suppressants, including acute tubulointerstitial nephritis, Clostridioides difficile–associated diarrhea, bone fracture, severe cutaneous adverse reactions, vitamin B12 deficiency, hypomagnesemia and related mineral abnormalities, and fundic gland polyps.15,16,29 Whether the incidence of these events differs meaningfully between individual P‑CABs, PPIs, and specific patient phenotypes remains unresolved. For a new agent such as zastaprazan, the appropriate conclusion is not that safety concerns are absent, but that long‑term and geographically diverse pharmacovigilance is still needed.8
Which patients might benefit most?
The most plausible clinical niche for P‑CABs is not all‑comer reflux disease, but selected phenotypes in which PPI limitations matter most. These include patients who require rapid symptom control, those with persistent nocturnal symptoms, CYP2C19 rapid or extensive metabolizers, patients with severe EE, and those with objective PPI‑refractory disease.8
Importantly, for most of these proposed clinical niches, supporting evidence is strongest for vonoprazan rather than for the newer P‑CABs such as zastaprazan; therefore, extrapolation across compounds should remain cautious.
Evidence for this targeted positioning is strongest for vonoprazan. Healing and maintenance benefits have been especially compelling in severe EE and in CYP2C19 extensive metabolizers.11,24,25 Small studies in PPI‑resistant reflux esophagitis also suggest that switching to vonoprazan can improve endoscopic healing and symptom scores. In a prospective study, 21 of 24 patients (87.5%) with PPI‑resistant reflux esophagitis achieved healing after 4 weeks of vonoprazan 20 mg, and maintenance with 10 mg prevented relapse in most responders.33 In a randomized study of PPI‑resistant EE, vonoprazan 20 mg and 40 mg markedly increased gastric pH holding time and achieved healing in more than 60% of evaluable patients despite prior PPI failure.34
At the same time, guideline positioning remains deliberately conservative. The 2024 American Gastroenterological Association (AGA) Clinical Practice Update is an expert review rather than a formal systematic guideline, yet it offers useful best‑practice advice.8 It recommends against routine first‑line use of P‑CABs for uninvestigated heartburn or nonerosive reflux disease, and against routine first‑line use in milder LA grade A/B EE. The document allows a stronger role of P‑CABs in selected patients with documented acid‑related reflux who fail twice‑daily PPI therapy and in more severe LA grade C/D EE, while also emphasizing cost, access barriers, and the absence of randomized comparisons against optimized double‑dose PPI strategies.8
For zastaprazan specifically, this is the key translational challenge: the drug already has high‑quality evidence for short‑term EE healing, but its likely greatest value may be in the very subgroups that were underrepresented in the published phase 3 trial.9 Studies accounting for severe EE, night‑time symptoms, documented PPI resistance, and non‑Asian populations would therefore be more informative than another broad noninferiority trial in predominantly low‑grade disease.
Stress ulcer prophylaxis: pharmacologic promise, evidentiary absence
SUP is the domain in which P‑CAB pharmacology is most tempting but its evidence base is the weakest. Stress‑related mucosal damage in critically ill adults arises largely from gastrointestinal hypoperfusion and reperfusion injury, and clinically important bleeding is concentrated in patients with recognizable risk factors, such as coagulopathy, shock, and chronic liver disease.14 Contemporary Society of Critical Care Medicine / American Society of Health‑System Pharmacists guidance recommends either a PPI or an histamine‑2 receptor antagonist for high‑risk critically ill adults, and does not incorporate P‑CABs into routine practice.14
The evidentiary bar for SUP has become higher, not lower. In the REVISE trial (Re‑Evaluating the Inhibition of Stress Erosions: Gastrointestinal Bleeding Prophylaxis in ICU),30 4821 invasively ventilated intensive care unit (ICU) patients were randomized to intravenous pantoprazole 40 mg daily or placebo. Clinically important upper gastrointestinal bleeding occurred in 1% of the patients receiving pantoprazole and 3.5% of those receiving placebo, with no significant difference in 90‑day mortality. In other words, contemporary PPI‑based SUP is not an outdated straw man; it remains supported by a large modern randomized trial.30
Why, then, do P‑CABs still warrant discussion in this space? Because their pharmacology maps neatly onto several theoretical needs of SUP: rapid first‑dose acid suppression, durable overnight and 24‑hour pH control, decreased dependence on meal timing, and reduced CYP2C19‑related variability.5-8 These features could be advantageous in newly intubated patients, in patients with interrupted enteral nutrition, or in the scenarios where immediate acid control is desired. The AGA document indirectly acknowledges this potential by noting that rapid and potent acid inhibition raises the possibility of utility in bleeding gastroduodenal ulcers, even while concluding that evidence is insufficient for first‑line use in that setting and advising against first‑line use in peptic ulcer treatment or prophylaxis more broadly.8
Yet several reasons prevent a scientifically defensible leap from reflux pharmacology to ICU prophylaxis. First, SUP is not simply an acid disease; acid is a modifiable cofactor superimposed on a vascular and systemic critical illness syndrome. Second, the existing P‑CAB evidence comes overwhelmingly from ambulatory oral studies in GERD or peptic ulcer contexts rather than from critically ill patients with shock, organ failure, vasopressor exposure, polypharmacy, and altered enteral absorption.8,14 Third, ICU‑specific safety questions remain unanswered for P‑CABs, including their effects on infection risk, micronutrient abnormalities, and drug‑drug interactions in the setting of prolonged critical illness.14,15,29 Fourth, there are no randomized or even robust observational studies demonstrating that any P‑CAB reduces clinically important stress‑related bleeding in ICU populations.14
Accordingly, the most defensible present position is straightforward: P‑CABs are a promising investigational concept for SUP, but not a routine clinical alternative to PPIs or histamine‑2 receptor antagonists.14 The key gap in the literature is not a nuanced comparative effectiveness problem—it is the absence of direct evidence. Based on the currently available data, the proposed practical positioning of P‑CABs vs PPIs across erosive reflux disease and SUP is summarized in Figure 2.
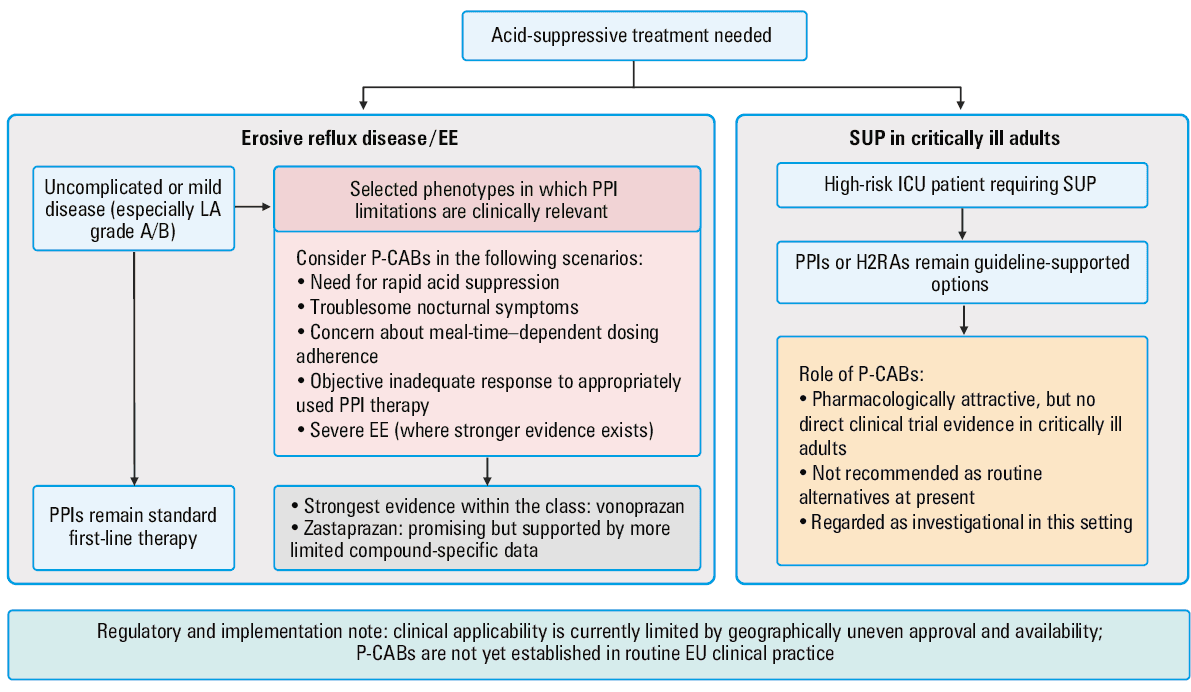
Abbreviations: EU, European Union; LA, Los Angeles; others, see Figure 1 and Tables 1 and 2
Regulatory status and near‑term development
The regulatory trajectory of P‑CABs is clinically relevant, but it also defines an important limitation of the present review. Regulatory approval and real‑world availability remain geographically uneven, and this should temper direct extrapolation to current European practice. In the United States, vonoprazan is approved for healing and maintenance of healing of EE and for use in vonoprazan‑containing regimens for Helicobacter pylori eradication.15,29 By contrast, although regulatory activity for vonoprazan is visible in Europe, P‑CABs are not yet established as components of routine European Union clinical practice.
Zastaprazan has followed a different path. According to the published first‑approval report, it received its first approval in South Korea in April 2024 for the treatment of erosive GERD.10 The same report describes ongoing development in adjacent ulcer‑related indications, including gastric ulcers and prevention of nonsteroidal anti‑inflammatory drug–induced peptic ulcers. These developments may broaden confidence in the compound’s acid‑suppressive profile, but they do not substitute for direct evidence in SUP, nor do they imply current routine availability in Europe.
Accordingly, the present review should be interpreted as clinically informative with respect to an evolving international evidence base and future therapeutic positioning, rather than as a reflection of therapies already incorporated into routine European care pathways. This distinction is particularly important when considering the near‑term applicability of these data to European prescribing practice.
Discussion: clinical positioning and research priorities
The key clinical question is not simply whether P‑CABs provide more rapid acid suppression than PPIs, but whether this pharmacologic advantage translates into clinically meaningful differences for specific agents in specific patient populations. In erosive reflux disease, the available evidence suggests that this may be the case, but the strength of support differs across compounds. At present, the most mature clinical evidence within the class is derived from vonoprazan studies, whereas compound‑specific evidence for zastaprazan remains promising but still comparatively early. For that reason, broader class data should be interpreted as a supportive context rather than as proof of interchangeable efficacy or safety across all P‑CABs.5,6,19
At present, however, P‑CABs should not be viewed as universal replacements for PPIs. This caution is particularly relevant in Europe, where the current routine clinical availability of these agents remains limited, so the practical implications of the available evidence are presently greater for future positioning than for immediate widespread implementation. Conventional PPIs remain effective, familiar, widely available, and supported by extensive long‑term clinical experience. A balanced clinical approach is therefore to consider PPIs as the standard first‑line therapy for most patients with uncomplicated reflux disease, while recognizing that P‑CABs may be particularly useful in selected scenarios, including EE requiring rapid control, prior suboptimal response to appropriately used PPI therapy, troublesome nocturnal symptoms, or situations in which adherence to meal‑time–depending dosing is uncertain.8 Whether this preferential role should extend to severe LA grade C/D esophagitis or to long‑term maintenance treatment with newer agents such as zastaprazan remains to be established more directly.9,11
The situation is different in SUP. In this setting, the evidentiary threshold is appropriately higher, because treatment is preventive, is often used in critically ill patients, and is judged against clinically important outcomes rather than symptom relief or mucosal healing alone.14 Pharmacologic plausibility by itself is insufficient. Before P‑CABs can be reasonably incorporated into ICU practice, they should demonstrate predictable pharmacokinetic and pharmacodynamic performance in critical illness and then be evaluated against contemporary PPI‑based strategies in appropriately designed clinical studies.36 Until such data are available, routine extrapolation from reflux disease to SUP is not supported by the current evidence base.
This distinction helps define a more appropriate place for the class in practice. The relevant clinical message is not that stronger acid suppression should automatically lead to broad replacement of PPIs, but rather that P‑CABs may be better suited to selected acid‑mediated clinical phenotypes, whereas PPIs remain the reference standard where trial evidence, cost‑effectiveness, and guideline support continue to be decisive.8 Such an approach allows for integration of a promising therapeutic class without extending its use beyond the available evidence.
The implications for future research follow directly from this position. In critical care, the priority should be stepwise: ICU‑specific pharmacokinetic and pharmacodynamic studies, early proof‑of‑concept trials in patients at the highest bleeding risk, and subsequently larger comparative trials powered for clinically important upper gastrointestinal bleeding outcomes.37 In reflux disease, future studies should move beyond the current evidence base and include phenotype‑enriched trials in severe EE, nocturnal‑symptom phenotypes, and objectively defined PPI nonresponse, as well as comparisons against optimized double‑dose PPI regimens rather than standard‑dose controls alone.8
Long‑term safety and implementation data will also be important in determining whether early enthusiasm leads to sustained practice change. For zastaprazan, this includes prospective evaluation of hypergastrinemia, gastric histologic effects, infection‑related outcomes, renal events, micronutrient consequences, and real‑world drug‑drug interactions, together with formal health‑economic assessment.9,15,29 Overall, current evidence supports serious consideration of P‑CABs in reflux disease, but it does not yet justify their routine use for SUP in critically ill adults.
Conclusions
P‑CABs represent a clinically relevant therapeutic approach in acid‑related disease, but the evidence base is not uniform across the class. In erosive reflux disease, the most robust clinical data currently come from vonoprazan studies, while zastaprazan is supported by early pharmacologic evidence and a single phase 3 trial showing noninferior healing vs esomeprazole in a predominantly low‑grade EE population.11 Thus, compound‑specific conclusions are more appropriate than broad assumptions of interchangeable class effects. At present, zastaprazan should be regarded as a promising but still less extensively characterized member of the class. By contrast, no P‑CAB currently has direct clinical evidence supporting routine use for SUP in critically ill adults. In addition, because P‑CAB availability remains geographically uneven and these agents are not yet established in routine European Union clinical practice, the immediate clinical applicability of this review to European care settings remains limited.
- Katz PO, Dunbar KB, Schnoll‑Sussman FH, et al. ACG clinical guideline for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol. 2022; 117: 27‑56. | Crossref
- Fass R. Gastroesophageal reflux disease. N Engl J Med. 2022; 387: 1207‑1216. | Crossref
- Spechler SJ, Hunter JG, Jones KM, et al. Randomized trial of medical versus surgical treatment for refractory heartburn. N Engl J Med. 2019; 381: 1513‑1523. | Crossref
- Scarpignato C, Hongo M, Wu JCY, et al. Pharmacologic treatment of GERD: where we are now, and where are we going? Ann N Y Acad Sci. 2020; 1482: 193‑212. | Crossref
- Qiao X, Li P. Potassium‑competitive acid blockers and advances in the management of patients with acid‑related diseases: a narrative review. Front Physiol. 2025; 16: 1655102. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION