Erectile dysfunction and quality of life after myocardial infarction: a cross-sectional study with routine point-of-care penile Doppler ultrasonography
Key words: erectile dysfunction, myocardial infarction, penile Doppler ultrasound, point-of-care ultrasound, quality of life

 CC BY 4.0
CC BY 4.0
Erectile dysfunction and quality of life after myocardial infarction: a cross-sectional study with routine point-of-care penile Doppler ultrasonography
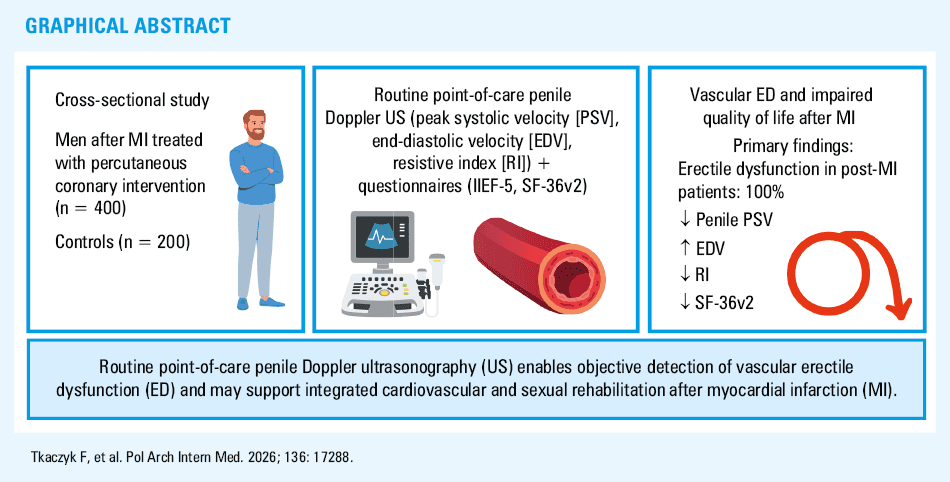
Introduction: Erectile dysfunction (ED) is common in men after myocardial infarction (MI) and is associated with poorer quality of life and systemic vascular disease. Previous studies have primarily relied on questionnaires, rarely including objective assessment of penile hemodynamics.
Objectives: We aimed to assess the quality of life in men with ED after MI treated with percutaneous coronary intervention (PCI), including routine assessment of penile hemodynamics using point‑of‑care resting Doppler ultrasonography.
Patients and methods: This observational, cross‑sectional, single‑center study included 600 men: 400 after MI treated with PCI and 200 without a history of MI/PCI (controls). ED was assessed using the 5‑item version of the International Index of Erectile Function (IIEF‑5) questionnaire, and quality of life was assessed using the 36‑item Short‑Form Health Survey, version 2 (SF‑36v2) questionnaire. Echocardiography, carotid Doppler ultrasound, and resting penile Doppler ultrasound were performed. Associations were analyzed using the Spearman correlation and multivariable linear regression.
Results: All patients after MI had ED. Quality of life scores were significantly lower in the MI group than in the controls globally (mean [SD] SF‑36v2 score, 121.3 [8.9] vs 134.6 [7.5]; P <0.001) and in the physical and mental components. Penile Doppler parameters differed between the groups and correlated with IIEF‑5 scores. In multivariable analysis, the strongest predictor of quality of life was erectile function (IIEF‑5), followed by left ventricular ejection fraction, body mass index, heart rate, and vascular parameters (intima‑media thickness, carotid and penile flow).
Conclusions: ED severity is a major independent determinant of the quality of life in men after MI/PCI. Penile hemodynamic parameters reflect systemic vascular burden and functional status. Integrated ED assessment that includes the IIEF‑5 questionnaire and routine resting penile Doppler ultrasound may enhance risk stratification and post‑MI care.
Introduction
In recent decades, the prognosis after myocardial infarction (MI) has significantly improved; mortality rates in developed countries currently range from 7% to 10% within the first year, and from 15% to 20% within 5 years.1,2 Data obtained from large population‑based cohorts confirm this trend. In the United Kingdom, the annual risk of death after the first MI event was 8.2%, and the 5‑year risk was 17.2%.3 Meanwhile, in Australia, in‑hospital mortality reached 2.2%, with 15.9% of deaths occurring over a 4.5‑year follow‑up period.4 However, the decline in cardiovascular mortality is accompanied by an increasing relative share of deaths from noncardiac causes in long‑term follow‑up, reflecting the chronic nature of the MI consequences.5,6 Contemporary registry data confirm that despite overall improvements in outcomes, important disparities in treatment and prognosis after ST‑segment elevation MI (STEMI) persist, particularly regarding delays in care provision and periprocedural outcomes.7
In acute MI, both STEMI and non‑STEMI (NSTEMI), percutaneous coronary intervention (PCI) is the preferred invasive treatment, as it reduces mortality in comparison with fibrinolysis. In the Danish population, implementation of a primary PCI strategy was associated with a decrease in annual mortality from 10.8% to 7.7%, with current in‑hospital mortality at approximately 2.2%. In patients with MI and reduced left ventricular ejection fraction (LVEF ≤40%), PCI reduces the risk of all‑cause mortality, cardiovascular death, sudden cardiac death, reinfarction, and hospitalization for heart failure.8-10 Conversely, in stable coronary artery disease (CAD), PCI affects neither mortality nor the incidence of MI, but it effectively relieves symptoms and improves quality of life (QoL), particularly in patients with severe angina pectoris.11,12 Recent registry‑based studies further emphasize the prognostic importance of CAD complexity, completeness of revascularization, as well as patient heterogeneity, including younger populations with distinct clinical characteristics and outcomes following MI.13,14
Especially in the first months after MI, QoL deteriorates significantly; the greatest and most persistent decline is observed after spontaneous, rather than periprocedural, infarction.15 European studies indicate that reduced QoL is common in the early postinfarction period and persists or exacerbates in some patients during the first year, especially among those with comorbidities.16 Although revascularization therapy and cardiac rehabilitation may partially improve patient functioning, long‑term QoL after MI is primarily determined by persistent symptoms, cardiac complications, as well as psychosocial and behavioral factors, emphasizing the need for a comprehensive therapeutic approach.17-20 Moreover, metabolic and inflammatory mechanisms, including lipid‑related factors, such as lipoprotein(a), may further contribute to long‑term cardiovascular risk and progression of the disease after acute coronary syndromes.21
Sexual health is a vital component of QoL for patients after MI. According to the American College of Cardiology and the American Heart Association (AHA), sexual functioning is an integral component of QoL, and sexual dysfunction is common in patients with CAD and its risk factors. Sexual activity corresponds to moderate physical activity (3–5 Metabolic equivalents [METS] on the Metabolic Equivalent of Task scale) and can be usually safely resumed approximately 3 weeks after an uncomplicated MI, provided there is a negative result on a stress test.22
Sexual dysfunction, including ED and decreased libido, occurs in approximately 40%–60% of post‑MI patients and is strongly associated with poor QoL, depressive symptoms, and a lower level of illness acceptance.23 Interventions such as sexual counseling, psychological support, and cardiac rehabilitation contribute to the improvement in sexual functioning and QoL after MI.24,25
To date, the relationship between ED, QoL, and objective penile hemodynamics assessed by routine point‑of‑care Doppler ultrasound examination in men after MI treated with PCI has not been jointly investigated.
The aim of this study was to assess QoL in men with ED after MI treated with PCI. Additionally, particular emphasis was put on the role of routine point‑of‑care penile Doppler ultrasonography in the evaluation of ED.
Patients and methods
Study design
This observational, cross‑sectional study comprised 4 stages of data collection and analysis. Stage 1 involved selecting the participants based on their medical interviews, medical records review, and assessment of inclusion and exclusion criteria. Stage 2 focused on collecting clinical, anthropometric, and laboratory data during patient hospitalization. In stage 3, imaging and functional cardiovascular tests were performed. Stage 4 involved the assessment of QoL, sexual functioning, and psychosocial factors using standardized questionnaires. Integrating data from multiple sources enabled cross‑validation and improved reliability of results while minimizing potential bias. The study design is illustrated in Figure 1.
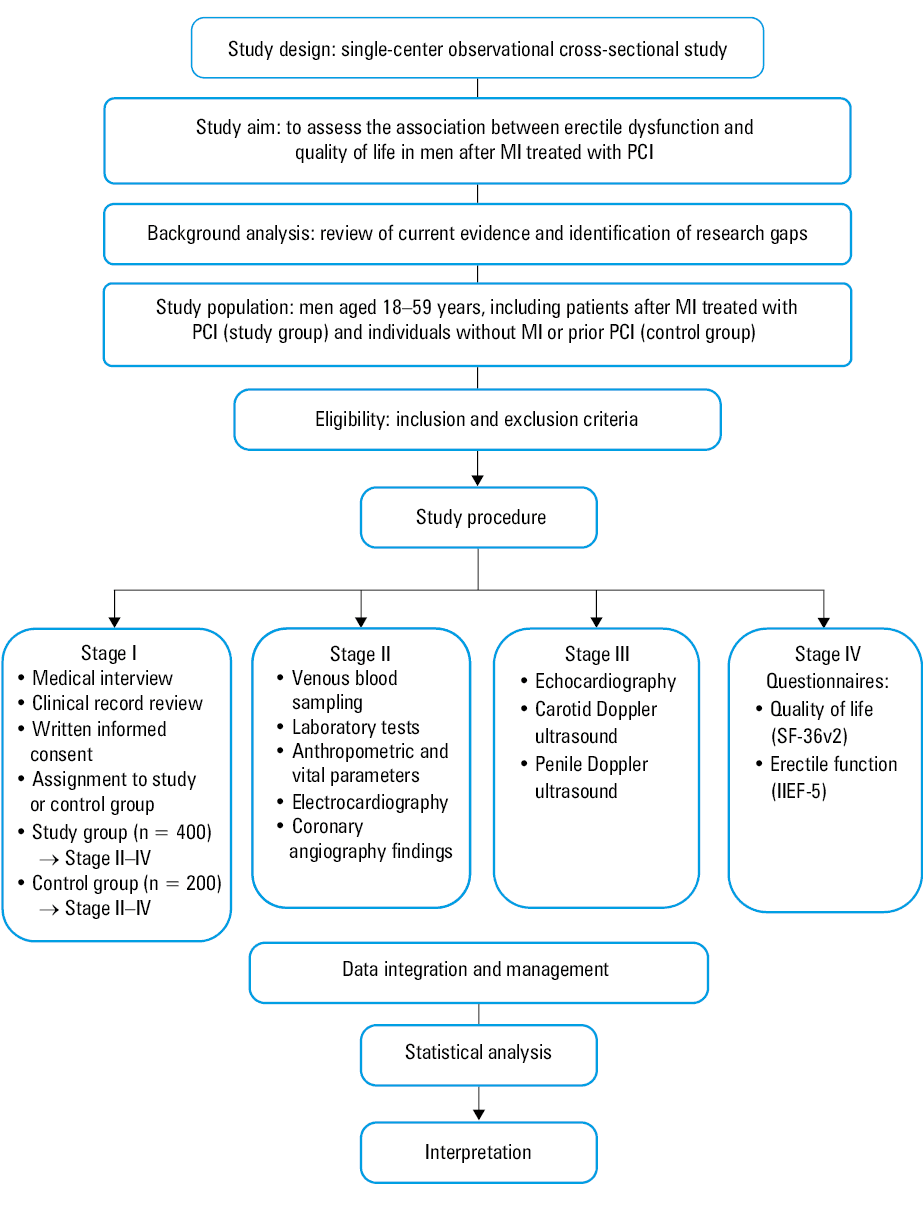
Abbreviations: IIEF‑5, 5‑item version of the International Index of Erectile Function questionnaire; MI, myocardial infarction; PCI, percutaneous coronary intervention; SF‑36v2, 36‑item Short Form Health Survey, version 2
The study was conducted from February 2024 to November 2025 at the Clinical Department of Cardiology, Dr. Tytus Chałubiński Specialist Hospital in Radom, Poland. The study protocol received approval from the Bioethics Committee of the Jan Kochanowski University in Kielce (5/2024). The study was conducted in accordance with the principles of the Declaration of Helsinki and its subsequent amendments. All participants provided written informed consent prior to enrollment. The study was covered by mandatory third‑party liability insurance for medical research.
Participants
The study included men aged 18–59 years with a history of MI, either STEMI or NSTEMI, treated with PCI within the previous 10 years, but no later than 12 months before initiation of the treatment. The patients were recruited during planned hospitalization for cardiological diagnostics. Exclusion criteria comprised a history of or current cancer, a history of or current psychiatric disorder, alcohol dependence syndrome, prior coronary artery bypass grafting, prior stroke, diabetes, hormone therapy within the preceding 12 months, and anticipated inability to comply with study procedures. The control group included individuals without diagnosed cardiovascular disease (CVD) referred for routine cardiological evaluation (eg, preventive assessment or nonspecific symptoms), representing a metabolically healthy reference population. The control group was recruited at the same institution during the study period. The participants were consecutively enrolled and met the same general eligibility criteria as the study group, except for the absence of a history of MI or prior PCI. All participants in the control group followed an identical standardized study protocol. This included clinical assessment, laboratory testing, echocardiography, carotid Doppler ultrasonography, resting pen ile Doppler examination, and completing identical validated questionnaires (5‑item version of the International Index of Erectile Function [IIEF‑5] and 36‑item Short Form Health Survey, version 2 [SF‑36v2]), performed under the same conditions and by the same study team.
Variables
The primary independent variable was the presence of ED, assessed using the IIEF‑5 and classified according to current cutoff scores. The IIEF‑5 is a widely used, validated screening tool for ED, with high sensitivity (0.98) and specificity (0.88); it is available in multiple languages and population‑based versions, and its questionnaire remains open access.26
The dependent variable was QoL, assessed using the SF‑36 questionnaire (license No. QUO‑03978‑C0Q3T0), analyzed both as a global score and within individual domains. The SF‑36v2 is widely recommended in clinical trials and practice as a tool for assessing and monitoring QoL and long‑term treatment outcomes in patients with a history of MI.27
Data sources
Data regarding ED and QoL were collected using standardized self‑assessment questionnaires completed by the participants during hospitalization. Clinical data, including time since MI, left ventricular ejection fraction (LVEF), hemodynamic parameters, body mass index (BMI), laboratory test results, and coronary angiography results, were obtained from medical records. Information regarding lifestyle, sexual activity, and selected psychosocial factors was obtained through a face‑to‑face interview using a structured questionnaire. During hospitalization, the participants underwent point‑of‑care carotid Doppler ultrasound and resting penile Doppler ultrasound using a LOGIQ S7 XDclear 2.0 system (GE Healthcare) equipped with a high‑frequency linear array transducer (7.5–12 MHz). Penile examination was performed in the supine position, in standardized conditions. This included bilateral assessment of the cavernous arteries in longitudinal and transverse projections, as well as recording of flow spectra and basic hemodynamic parameters (peak systolic velocity [PSV], end‑diastolic velocity [EDV]). Patient privacy was maintained during the procedure. All measurements were performed by a single experienced investigator (FT) according to a standardized protocol.
Statistical analysis
Normality of distribution was assessed using the Shapiro–Wilk test. Continuous variables were presented as mean (SD) or median (interquartile range [IQR]), depending on data distribution. Comparisons between the groups were performed using the Welch t test or Wilcoxon rank‑sum test and the χ² test or Fisher exact test. Associations were assessed using the Spearman correlation coefficient. Independent determinants of QoL were identified using multivariable linear regression with backward stepwise selection based on the Akaike information criterion to reduce the risk of model overfitting. Model fit was assessed using R² and adjusted R²; multicollinearity was assessed using variance inflation factors, and normality of residuals using the Shapiro–Wilk test. Confidence intervals are reported at the 95% level. As a sensitivity analysis, propensity score matching was performed using the nearest‑neighbor matching (1:1 ratio) with a caliper of 0.2 of the SD of the propensity score logit. Covariates included age, BMI, blood pressure, heart rate (HR), lipid profile, fasting glucose level, smoking status, and hypertension. Additional multivariable analyses were performed in the entire study population to assess the consistency of the observed associations. Analyses were performed using R (version 4.3.3; R Core Team, 2024). P values below 0.05 were considered significant.
Results
A total of 600 men meeting the eligibility criteria were included in the study, comprising 400 patients with a history of MI treated with PCI (study group) and 200 men without MI and without a history of PCI (control group). As a sensitivity analysis, propensity score matching was performed. In the propensity score–matched cohort (n = 180 pairs), baseline characteristics were well balanced, with all standardized mean differences below 0.1. The differences in QoL between the groups remained significant (mean [SD] SF‑36v2 total score, 122.1 [8.5] in the study group vs 133.8 [7.6] in the control group; P <0.001). Similarly, the associations between ED and QoL, as well as the direction and magnitude of relationships observed in multivariable analyses, remained consistent with the primary findings.
Characteristics of the study population
Baseline clinical, hemodynamic, and biochemical characteristics of the study and control groups are presented in Table 1. As expected, the patients after MI demonstrated a less favorable cardiovascular risk profile than the controls. The median (IQR) age was 45 (37–54) years in the study group and 44 (36–52) years in the control group. The largest group consisted of married men (66%), while the percentages of single and divorced individuals were 23% and 10%, respectively. The vast majority of participants were professionally active (91%). The median time since MI was 50 (26–80) months, indicating a stable population in the long term after coronary revascularization.
Variable | Study group (n = 400) | Control group (n = 200) | P value |
Data are presented as mean (SD) or median (interquartile range), unless indicated otherwise, depending on distribution assessed using the Shapiro–Wilk test.
SI conversion factors: to convert total cholesterol, LDL cholesterol, and HDL cholesterol to mmol/l, multiply by 0.0259; triglycerides to mmol/l, by 0.0113; glucose to mmol/l, by 0.0555.
Abbreviations: BMI, body mass index; BP, blood pressure; CCA‑IMT, common carotid artery intima‑media thickness; HDL, high‑density lipoprotein; HR, heart rate; LDL, low‑density lipoprotein; LVEF, left ventricular ejection fraction | |||
Age, y | 45 (37–54) | 44 (36–52) | 0.27 |
Height, cm | 178.5 (6.6) | 178 (6.9) | 0.4 |
Body weight, kg | 85.1 (11) | 80.3 (10.7) | <0.001 |
BMI, kg/m2 | 26.8 (3) | 25.2 (2.7) | <0.001 |
Systolic BP, mm Hg | 133 (12) | 122 (10) | <0.001 |
Diastolic BP, mm Hg | 83 (8) | 78 (7) | <0.001 |
HR, bpm | 74 (9) | 67 (7) | <0.001 |
LVEF, % | 42 (38–46) | 60 (57–63) | <0.001 |
CCA‑IMT, mm | 1.19 (1.05–1.35) | 0.78 (0.68–0.88) | <0.001 |
Total cholesterol, mg/dl | 198 (172–224) | 176 (160–194) | <0.001 |
LDL cholesterol, mg/dl | 122 (102–146) | 102 (88–118) | <0.001 |
HDL cholesterol, mg/dl | 52 (46–58) | 62 (56–70) | <0.001 |
Triglycerides, mg/dl | 140 (108–180) | 110 (88–132) | <0.001 |
Fasting glucose, mg/dl | 96 (90–101) | 90 (85–95) | <0.001 |
Current smoking, n (%) | 170 (42.5) | 40 (20) | <0.001 |
Hypertension, n (%) | 200 (50) | 10 (5) | <0.001 |
Severity of erectile dysfunction
All patients in the study group (n = 400) met the IIEF‑5 criteria for ED. Mild‑to‑moderate types of ED predominated, affecting 89% of the participants, while moderate ED was found in 11%.
Mean IIEF‑5 score in the study group was 13.9 (1.5) points (95% CI, 13.7–14.1), which corresponds to clinically significant mild‑to‑moderate ED. The lowest scores were observed in the domains of erectile frequency and ability to maintain erection (mean, 2.1 [0.5] and 2.5 [0.6] points, respectively), indicating that insufficient durability of the erectile response was the dominant problem. The sexual satisfaction score was relatively higher (3.3 [0.5] points) as compared with the other domains, suggesting partial preservation of sexual function despite the presence of an organic vascular deficit. In contrast, the participants in the control group demonstrated preserved erectile function, with significantly higher IIEF‑5 scores than the study group (Table 2). Most individuals in the control group failed to meet the criteria for ED.
Parameter | Study group (n = 400) | Control group (n = 200) | P valuea |
Data are presented as median (interquartile range).
a Between‑group comparisons were performed using the Wilcoxon rank‑sum test.
Abbreviations: EDV, end‑diastolic velocity; PSV, peak systolic velocity; RI, resistive index; others see Figure 1 | |||
IIEF‑5 score, points | 15 (12–18) | 24 (23–25) | <0.001 |
PSV, cm/s | 23 (17–27) | 28.5 (26–31) | <0.001 |
EDV, cm/s | 6 (5–9) | 5 (4–6) | <0.001 |
RI | 0.74 (0.65–0.82) | 0.82 (0.78–0.9) | <0.001 |
Quality of life according to the 36‑item Short‑Form Health Survey
QoL assessed with the SF‑36v2 questionnaire was significantly lower in the study group (n = 400) than in the control group (n = 200) across all domains (Table 3). The largest differences were observed in the physical component summary (ie, physical functioning, physical role limitations, bodily pain, and general health), although significant deterioration was also observed in the mental domains (ie, vitality, social functioning, and role emotional limitations). Total mean SF‑36v2 score was 121.3 (8.9) points in the study group and 134.6 (7.5) points in the control group (P <0.001). Summary indicators of physical and mental health were significantly lower in the patients with ED after MI.
Parameter | Study group (n = 400) | Control group (n = 200) | P valuea |
Data are presented as mean (SD).
a Between‑group comparisons were performed using the Welch t test.
Abbreviations: see Figure 1 | |||
Global SF‑36 score | 121.3 (8.9) | 134.6 (7.5) | <0.001 |
Physical component | 58.2 (5.4) | 67.9 (5.1) | <0.001 |
Physical functioning | 55.6 (7.2) | 70.8 (6.3) | <0.001 |
Role physical | 56.3 (8.1) | 69.5 (6.8) | <0.001 |
Bodily pain | 59.8 (7) | 68.7 (6.1) | <0.001 |
General health | 57.9 (6.8) | 69.2 (5.9) | <0.001 |
Mental component | 63.1 (6) | 69.4 (5.7) | <0.001 |
Social functioning | 66.8 (7.5) | 73.9 (6.2) | <0.001 |
Vitality | 62.7 (6.9) | 70.1 (6) | <0.001 |
Mental health | 64.9 (6.4) | 71.0 (5.6) | <0.001 |
Role emotional | 61.5 (7.3) | 68.3 (6.5) | <0.001 |
Clinical and cardiovascular characteristics of the patients with erectile dysfunction
On echocardiography, the patients in the study group demonstrated poorer LV structure and function than those in the control group. Median LVEF was 42% (38%–46%) in the study group and 58% (55%–62%) in the control group. LV diastolic diameter was 5.49 (4.99–6.01) cm in the study group and 4.92 (4.55–5.28) cm in the control group, whereas left atrial diameter was 4.11 (3.37–4.3) cm in the study group and 3.62 (3.28–3.95) cm in the control group. Median E/A ratio was lower in the study group (1.06 [0.78–1.25]) than in the control group (1.28 [1.05–1.46]), indicating more frequent diastolic dysfunction after MI.
On carotid Doppler ultrasound, the intima‑media thickness (IMT) was greater in the study group than in the control group both in terms of the common carotid artery (1.19 [1.05–1.35] mm vs 0.84 [0.72–0.96] mm) and the internal carotid artery (1.13 [0.99–1.29] mm vs 0.79 [0.68–0.92] mm), indicating more severe atherosclerotic changes.
The lipid profile was less favorable in the patients after MI than in the controls. Median total cholesterol level was 198 (172–224) mg/dl in the study group and 182 (165–205) mg/dl in the control group, low‑density lipoprotein level was 122 (102–146) mg/dl and 108 (92–126) mg/dl, high‑density lipoprotein 52.4 (46.3–58.3) mg/dl and 58.9 (52.1–66.4) mg/dl, and triglyceride level was 140.1 (107.7–179.6) mg/dl and 118.6 (92.4–149.3) mg/dl, respectively.
On resting penile Doppler ultrasound, the patients in the study group demonstrated lower PSV and resistive index (RI), as well as higher EDV values than the control group, suggesting impaired cavernous artery hemodynamics in the course of ED. In an analysis stratified by ED severity (IIEF‑5 scale), Doppler parameters differed significantly between the control group, patients with mild‑to‑moderate ED, and patients with moderate ED. These findings demonstrated a gradual decrease in PSV and RI values with increasing ED severity, with an opposite trend for EDV. The IIEF‑5 score correlated significantly with PSV and RI values, confirming the concordance of the questionnaire assessment with objective hemodynamic parameters (Table 4).
Explanatory variable | Quality of life (SF‑36 total score) post‑MI group | ||
β | 95% CI | P value | |
Model R2 =0.62; adjusted R2 =0.6; n = 400. The model was fitted in the post‑MI group The final model was derived using backward stepwise selection based on the Akaike information criterion (AIC). Variables included in the initial model were selected based on clinical relevance and prior literature.
| |||
Constant | 120.96 | 119.05–122.87 | <0.001 |
Age, y | –0.04 | –0.1 to 0.01 | 0.15 |
BMI, kg/m² | –0.36 | – | 0.006 |
IIEF‑5, points | 1.42 | 1.16–1.68 | <0.001 |
Heart rate, bpm | –0.05 | –0.09 to 0 | 0.04 |
LVEF, % | 0.18 | 0.1–0.25 | <0.001 |
LA, cm | –0.51 | –1.73 to 0.72 | 0.42 |
AVV, m/s | 1.49 | 0.07–2.92 | 0.04 |
ICA‑PSV, cm/s | –0.03 | –0.04 to –0.01 | <0.001 |
ICA‑EDV, cm/s | 0.07 | 0.04–0.1 | <0.001 |
ICA flow: turbulent vs laminar | –8.03 |
| <0.001 |
CCA‑IMT, mm | –5.46 |
| <0.001 |
Penile PSV, cm/s | 0.12 | 0.01–0.24 | 0.03 |
Penile EDV, cm/s | –0.14 | –0.31 to 0.04 | 0.12 |
WBC, × 103/µl | –0.52 | –0.78 to –0.27 | <0.001 |
RBC, × 106/µl | –0.47 | –0.75 to –0.19 | <0.001 |
Neutrophils, % | 0.24 | 0.16–0.31 | <0.001 |
Total cholesterol, mg/dl | 0.03 | 0.01–0.04 | 0.004 |
HDL cholesterol, mg/dl | 0.05 | –0.02 to 0.11 | 0.17 |
LDL cholesterol, mg/dl | 0.01 | 0.00–0.02 | 0.03 |
Chlorides, mmol/l | 0.28 | 0.07–0.49 | 0.01 |
Determinants of quality of life: multivariable analysis
Multivariable analysis of the SF‑36v2 summary score performed in the post‑MI group identified several independent determinants of QoL. The strongest positive predictor, as reflected by the magnitude of the regression coefficient (β), was ED assessed by the IIEF‑5 scale, while higher BMI and higher HR values were independently associated with lower QoL. Better LV systolic function remained significantly associated with higher SF‑36v2 scores (Table 4).
In an additional analysis including the entire study population (n = 600), ED was also significantly associated with QoL. In multivariable linear regression analysis, a higher IIEF‑5 score was associated with a higher SF‑36v2 total score, as reflected by the regression coefficient (β = 1.42; 95% CI, 1.21–1.63; P <0.001). Other independent determinants of QoL included LVEF, BMI, and HR.
Discussion
ED and CVD are closely linked through a common pathophysiological basis, primarily encompassing generalized endothelial dysfunction and atherosclerosis. MI is a critical clinical event that not only impacts the physical health, but also the psychosocial functioning and perceived QoL. In the population of patients with CAD, the prevalence of ED is high; its onset may precede the occurrence of coronary symptoms even by several years, suggesting that ED may serve as an early marker of generalized vascular disease.28-30 As expected in a real‑world post‑MI population, the study patients differed from the controls in terms of cardiovascular risk profile and cardiac function. These differences reflect the distinct clinical characteristics of the studied populations and represent a potential source of confounding; however, this was addressed in multivariable analyses and further supported by consistent results in the propensity score‑matched analysis. The consistency of the results between the primary and propensity score‑matched analyses supports the robustness of the observed associations.
The prevalence of ED in the analyzed cohort, assessed, among others, using the IIEF‑5 questionnaire, was 100% and exceeded the values reported in most studies of patients after MI. In a meta‑analysis by Sam et al,28 the incidence of de novo ED after the first MI was estimated at 64.4%, and in prospective studies of patients with STEMI treated with PCI, the rate of ED increased from approximately 50% immediately after the event to 79% within a few months. In other cohorts after acute MI, ED was observed in 76% to 84% of patients during early follow‑up.31 The 100% prevalence of ED observed in the present study should be interpreted with caution and in the context of the study design and population characteristics. The analyzed cohort comprised patients in a stable, long‑term phase after MI, representing a population with established vascular dysfunction. Furthermore, the use of a sensitive screening tool (IIEF‑5) enabled the detection of mild and subclinical forms of ED. Notably, the majority of cases were classified as mild‑to‑moderate, suggesting that this finding reflects a high prevalence of vascular impairment rather than severe clinical dysfunction. Therefore, these results should not be directly generalized to the broader population of patients after MI.
The homogeneous distribution of ED severity, including only mild‑to‑moderate and moderate forms, with no cases of normal function or severe ED, suggests a clinically consistent cohort of men with persistent, primarily vascular dysfunction typical of patients with PCI‑treated CAD. This profile reflects the chronic, stable nature of ED in the long‑term postinfarction period. Simultaneously, interventional data suggest that improvement in sexual function is possible in this population; Palm et al32 demonstrated a 6.7‑point increase in the IIEF‑5 score after 12 weeks of sexual rehabilitation, as compared with standard care.
In the analyzed cohort, QoL was significantly lower than in the control group, both globally (mean total SF‑36v2 score, 121.3 [8.9] in the study group vs 134.6 [7.5] in the control group; P <0.001) and in the physical (58.2 [5.4] vs 67.9 [5.1]) and mental (63.1 [6] vs 69.4 [5.7]) components. The largest differences involved physical functioning and physical role limitations, which is consistent with the observations of Brown et al33 and Huber et al34 in patients with CAD. The association between ED severity and poorer QoL, especially in the physical domain, was also confirmed by Sánchez‑Cruz et al35 and Kriston et al,36 indicating partial mediation by depressive symptoms. A similar profile, that is, greater deterioration of the physical component than the mental one, was also described in a meta‑analysis on cardiac rehabilitation.18 According to Vlachopoulos concept and the AHA/European Society of Cardiology position statements, ED constitutes an important element of QoL and a marker of cardiovascular risk, justifying routine assessment of sexual function and QoL in long‑term care after MI/PCI.37
Objective parameters confirm that there is a close association between ED and generalized vascular disease, consistent with the concept of ED and CVD as manifestations of the same atherosclerotic endothelial injury. The smaller diameter of penile arteries favors earlier manifestation of flow disturbances than in the coronary circulation,38 and a meta‑analysis by Mostafaei et al39 confirms ED as an independent predictor of CVD and MI. The parameters of the study cohort—moderately reduced LVEF (42%), increased IMT (common carotid artery, 1.19 mm; internal carotid artery, 1.13 mm), and penile Doppler profile (PSV, 23.5 cm/s; EDV, 6 cm/s)—indicate generalized atherosclerosis and a vascular type of ED, which is consistent with multiple reports.40-44 The coexistence of atrial fibrillation (17.3%) and an unfavorable metabolic profile further reflects the common inflammatory‑endothelial background of ED and CVD described in population‑based studies.45,46 A crucial methodological aspect is that penile Doppler ultrasound in the present study was performed in resting (flaccid) conditions without pharmacological stimulation. Therefore, PSV values should not be directly compared with standard diagnostic thresholds established for postpharmacological testing. In resting conditions, cavernosal arterial flow is physiologically low (typically 8–15 cm/s), and PSV serves primarily as a screening parameter. As demonstrated by Corona et al,44 resting PSV equal to or above 13 cm/s is associated with a high probability of normal dynamic PSV after pharmacological stimulation. Thus, the lower PSV observed in the study group vs controls likely reflects relative impairment of penile arterial inflow and subclinical vascular dysfunction rather than overt arterial insufficiency. The interpretation of increased EDV results requires consideration of both vascular and functional factors. Elevated EDV may reflect veno‑occlusive dysfunction; however, it can also be influenced by transient functional conditions. Anxiety has been shown to affect penile hemodynamics by impairing relaxation of smooth muscle, leading to delayed or incomplete erectile response and higher EDV values. In addition, structural abnormalities, such as Peyronie disease, may contribute to increased EDV through intracavernosal fibrosis and impaired veno‑occlusive mechanisms. In contrast, current evidence provides no support for a clear direct relationship between testosterone levels and EDV.47 Therefore, increased EDV observed in the present study should be interpreted as reflecting a complex interplay of vascular and functional mechanisms rather than a specific indicator of isolated venous insufficiency.48
ED was strongly associated with reduced QoL in men after MI treated with PCI, independent of other clinical factors. Lower IIEF‑5 scores correlated mainly with a poorer physical component of the SF‑36v2 questionnaire and, to a lesser extent, with the psychological component, which is consistent with earlier observations.34,35 Poorer cardiovascular and vascular parameters (lower LVEF, higher IMT, lower penile PSV) were associated with lower QoL. These results support earlier findings,41,45,46 indicating that ED is associated with a higher vascular burden and poorer well‑being in this population. Importantly, similar associations were observed in the analyses of the entire study population; however, these findings should be interpreted with caution, as they were primarily driven by variability within the study group, while ED was largely preserved in the control group. Given the limited variability of ED in the control group, this analysis primarily reflects between‑group differences rather than within‑group associations.
Taken together, our results indicate that the QoL of men with ED after MI is determined mainly by the severity of ED, cardiovascular function, and the degree of generalized vascular changes, independently of age and other clinical factors. These findings support the concept of ED as an integrative marker of systemic vascular health rather than an isolated urogenital condition.
Clinical implications
ED should be routinely assessed in men after MI treated with PCI because it is common and associated with a poorer QoL and increased vascular burden. Importantly, ED in this population may reflect underlying systemic vascular dysfunction rather than isolated sexual impairment. The diagnosis of ED allows for risk stratification and implementation of targeted interventions, including optimization of cardiovascular treatment and lifestyle modifications, psychosocial support, and structured sexual counseling as part of comprehensive cardiac rehabilitation and standard postinfarction care (Supplementary material, Table S1).
Limitations
This study has several limitations. First, the single‑center, observational, and cross‑sectional design, as well as the selective cohort of men (after MI treated with PCI, excluding those with diabetes or prior coronary artery bypass grafting) limit the generalizability of the results and causal inference. Second, the assessment of sexual function based on the IIEF‑5 score, as well as the absence of hormonal, psychological, and preinfarction data may have influenced the observed associations. Finally, given the observational design and baseline differences between the groups, residual confounding cannot be entirely ruled out. Additionally, the comparatively high number of variables in the multivariable model relative to the number of outcome events may increase the risk of overfitting, notwithstanding the use of the Akaike information criterion–based selection.
Conclusions
The severity of ED was the strongest independent predictor of QoL, showing a significant positive association with both physical and mental SF‑36 components. This confirms the central role of sexual health in the overall well‑being of men after MI. Penile hemodynamic parameters demonstrated an independent positive association with QoL, indicating that the degree of preserved penile perfusion is a clinically relevant marker of the overall vascular and functional status of patients after MI. The use of an integrated ED assessment including the IIEF‑5 score and resting penile Doppler ultrasonography provides complementary clinical data on the vascular and functional status of men after MI.
These results indicate that the assessment of sexual function and resting Doppler ultrasound of the penis should be routinely included in comprehensive care in men after MI. This approach may facilitate early identification of hemodynamic disorders, guide rehabilitation, and improve the QoL in this population.
- Martin SS, Aday AW, Allen NB, et al. 2025 Heart disease and stroke statistics: a report of U.S. and global data from the American Heart Association. Circulation. 2025; 151: e41‑e660. | Crossref
- Christensen DM, Strange JE, El‑Chouli M, et al. Temporal trends in noncardiovascular morbidity and mortality following acute myocardial infarction. J Am Coll Cardiol. 2023; 82: 971‑981. | Crossref
- Scholfield S, Zghebi SS, Rutter M, et al. Trends in mortality and major adverse cardiovascular events following incident acute myocardial infarction. BMC Cardiovasc Disord. 2026; 26: 125. | Crossref
- Nguyen J, Chan N, Hammett C, et al. Survivorship following myocardial infarction in a contemporary Australian cohort: defining cardiac versus non‑cardiac mortality. Intern Med J. 2025; 55: 812‑821. | Crossref
- Abou Hamed A, Gourraud M, Genet T, et al. Prognosis of patients with acute myocardial infarction in the setting of COVID‑19: a French nationwide observational study. Arch Cardiovasc Dis. 2025; 118: 312‑321. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION