Sex-related survival outcomes after unprotected left main percutaneous coronary intervention: evidence from the BIA-LM registry
Key words: coronary artery disease, left main coronary artery, percutaneous coronary intervention, registry, special populations



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Sex-related survival outcomes after unprotected left main percutaneous coronary intervention: evidence from the BIA-LM registry
Introduction: Sex‑related differences in outcomes after left main coronary artery (LMCA) percutaneous coronary intervention (PCI) remain incompletely understood, particularly in real‑world settings.
Objectives: This study evaluated the impact of sex assigned at birth on long‑term clinical outcomes after LMCA PCI in the largest single‑center registry in Poland.
Patients and methods: We retrospectively analyzed 998 patients who underwent LMCA PCI between 2007 and 2022. The end point was 5‑year all‑cause mortality. Survival analyses were performed in the overall cohort and after propensity score matching (PSM) and inverse probability of treatment weighting (IPTW).
Results: The final cohort included 814 patients, of whom 228 (28%) were women. In the whole population, there was no difference in 5‑year mortality between men and women (hazard ratio [HR], 1.31; 95% CI, 0.99–1.73; P = 0.06). PSM resulted in 471 pairs, and IPTW generated a weighted cohort of 469 patients (131 women [28%]). After PSM, men showed higher mortality (HR, 1.64; 95% CI, 1.28–2.11; P <0.001), consistent with IPTW analysis (HR, 1.71; 95% CI, 1.04–2.83; P = 0.04). Exploratory subgroup analyses demonstrated higher mortality among men with heart failure (HR, 2.25; 95% CI, 1.66–3.04; P = 0.002), those undergoing rotational atherectomy (HR, 4.15; 95% CI, 2.25–7.65; P <0.001), and those treated for 2 or more lesions (HR, 2.02; 95% CI, 1.44–2.83; P <0.001).
Conclusions: Men experienced worse long‑term survival than women after adjustment for clinical and procedural confounders. Mortality risk was higher among men with heart failure, multivessel disease, and those undergoing rotational atherectomy, highlighting the importance of considering sex‑based differences in LMCA management.
Introduction
Ischemic heart disease (IHD) constitutes a major cause of death worldwide, and remains the leading determinant of mortality among women.1,2 Clinical manifestation of IHD typically occurs approximately a decade later in women than in men, a delay partly linked to hormonal factors and the potentially protective effects of estrogen, though evidence remains inconclusive. Conversely, the marked increase in cardiovascular risk observed after menopause is well established. Women are also exposed to sex‑specific cardiovascular risk factors, including early menarche, preterm delivery, pre‑eclampsia, and gestational diabetes mellitus.1,3 Furthermore, they more often present with atypical features, such as dyspnea or fatigue, potentially contributing to diagnostic delays.1,3-5 Although biological mechanisms have long been emphasized in explaining sex‑based disparities in cardiovascular care, growing evidence highlights the role of sociocultural determinants, including communication dynamics, psychosocial stress, and the patient–physician relationship.1,3
The left main coronary artery (LMCA) represents one of the most critical anatomical sites in coronary artery disease (CAD). Historically, coronary artery bypass grafting (CABG) has been the gold standard in the treatment of LMCA disease, offering durable clinical outcomes. However, advances in percutaneous coronary intervention (PCI) have positioned PCI as a viable alternative in appropriately selected patients.2,6
The anatomical and physiological differences associated with sex introduce further complexity to the decision on revascularization treatment.3 This observation aligns with the growing emphasis in contemporary cardiovascular medicine on personalized clinical management, in which sex is increasingly recognized as an important determinant of therapeutic decision‑making.7,8 Notably, being a woman has been identified as an independent predictor of long‑term mortality following PCI, and has subsequently been incorporated into the SYNTAX II score, a validated clinical tool to guide revascularization strategies.9 However, follow‑up of landmark randomized trials, including EXCEL (Evaluation of XIENCE Versus Coronary Artery Bypass Surgery for Effectiveness of Left Main Revascularization), FREEDOM (Future Revascularization Evaluation in Patients with Diabetes Mellitus: Optimal Management of Multivessel Disease), and BEST (Randomized Comparison of Coronary Artery Bypass Surgery and Everolimus‑Eluting Stent Implantation in the Treatment of Patients With Multivessel Coronary Artery Disease) demonstrated that the treatment effect of PCI vs CABG on mortality over 3 to 8 years did not significantly differ between women and men,10 raising questions regarding the validity of sex as a prognostic determinant within the SYNTAX II model and the potential need for its reassessment.
Despite several randomized trials comparing PCI and CABG in patients with LMCA disease, the influence of sex on long‑term outcomes after PCI remains insufficiently characterized. Furthermore, numerous studies have shown that women with CAD often experience worse clinical outcomes than men. It is uncertain, if similar disparities also apply to patients undergoing LMCA PCI. To address this important knowledge gap, we aimed to analyze data from the largest single‑center registry of LMCA percutaneous revascularization procedures in Poland, focusing particularly on whether women have an unfavorable long‑term prognosis following PCI.
Patients and methods
Study population
The design and study population of the BIA‑LM registry were described before.2,11 In brief, out of the 998 patients undergoing LMCA PCI from December 27, 2007 to February 21, 2022, a total of 814 individuals with unprotected (ie, with no prior history of CABG) LMCA stenosis were included. The study flowchart is presented in Figure 1.
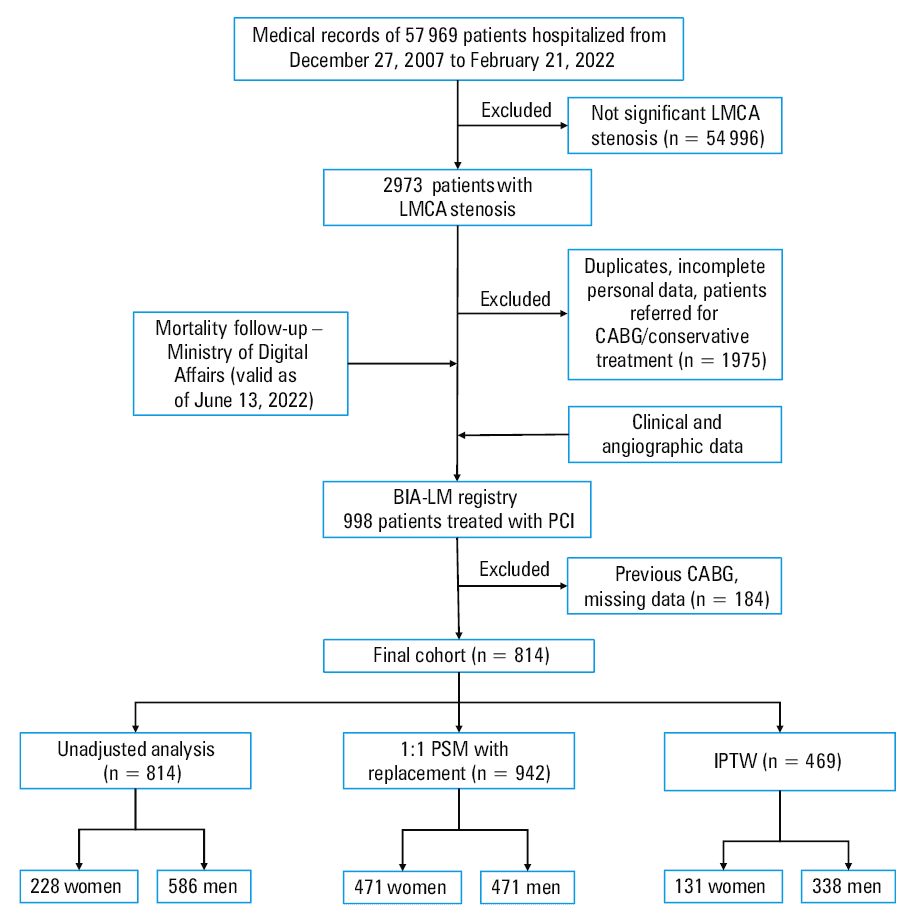
Abbreviations: CABG, coronary artery bypass grafting; IPTW, inverse probability of treatment weighting; LMCA, left main coronary artery; PCI, percutaneous coronary intervention; PSM, propensity score matching
The BIA‑LM registry was approved by the Bioethics Committee of the Medical University of Bialystok, Poland (APK.002.78.2022), and adheres to the 2013 Helsinki Declaration. The study is reported in accordance with the STROBE guidelines (Supplementary material, Table S1). Each patient hospitalized in the Medical University of Bialystok Clinical Hospital has consented to the use of data for research purposes aimed at evaluating the quality of provided services.
Definitions and outcome
The diagnosis of comorbidities was based on the anamnesis, previous reports, and electrocardiograms performed during the hospitalization, as well as on concomitant treatment and laboratory tests for selected diseases. Angiographic lesion characteristics were derived from procedural reports prepared by an interventional cardiologist performing PCI. LM lesion location was categorized as ostial / shaft or distal bifurcation. Distal lesions were defined as those involving the bifurcation into the left anterior descending (LAD) and / or left circumflex artery, including all Medina bifurcation patterns. In the cases of uncertain lesion localization, angiograms were additionally reviewed by 2 investigators (EJD and KG), which was required in 136 cases. A list of all International Classification of Diseases, Tenth Revision diagnostic codes and electronic health records search strategy is provided in Supplementary material.
All‑cause mortality data were obtained for all the patients from the Center for Information Technology, Ministry of Digital Affairs, Poland, and are valid as of June 13, 2022. For statistical analysis, 5‑year observation time was selected. No imputation methods were used for missing values for baseline variables.
Statistical analysis
Categorical baseline characteristics are presented as numbers and percentages. Continuous variables were assessed for normality using the Shapiro–Wilk test, and are reported as mean with SD or median with interquartile range (IQR). Comparisons between the groups were conducted using the χ2 test, the Rao–Scott corrected χ2 test, the Fisher test, the t test, or the Wilcoxon rank‑sum test when appropriate based on the data distribution. Interactions following principal component analysis (PCA) were assessed using the Wald test.
To ensure reduction of bias and confounding, mortality analysis was performed in the overall population and following implementation of propensity score matching (PSM), inverse probability of treatment weighting (IPTW), and PCA. In the first step of PSM, out of the baseline and angiographic variables, we determined mortality predictors with the least absolute shrinkage and selection operator (LASSO) Cox regression using 10‑fold cross‑validation with 100 λ values. The optimal penalty parameter was selected based on the minimum mean cross‑validated deviance. The LASSO cross‑validation plot is presented in Supplementary material, Figure S1. Secondly, multivariable Cox proportional hazard regression was performed and significant variables were included in the final model of one‑to‑one nearest neighbor matching with replacement (caliper of 0.2). As for IPTW, propensity scores were calculated using multiple logistic regression analysis and the variables provided in Supplementary material, Table S2. Weights were truncated on the 1st and 99th centiles to avoid overdispersion and stabilized to reduce variability. Median (IQR) stabilized weight was 1 (0.36–5.57), indicating an absence of extreme weights. Then, the analysis included survival assessment using the weighted univariate Cox proportional hazard regression model in the overall, PSM, and IPTW cohorts. Additional moderation effects and subgroup differences were examined in the cohorts adjusted with PSM and IPTW. The proportional hazard assumption was formally tested using the Schoenfeld residuals, while log‑log survival plots were used as a complementary graphical assessment. Findings from the LASSO cross‑validation, along with graphical displays of the Schoenfeld residuals and log‑log survival plots, are shown in Supplementary material, Figures S1–S8.
PCA was performed as an exploratory complementary analysis to summarize multiple correlated clinical variables into a small number of components reflecting overall clinical risk patterns. PCA was performed for 17 baseline and angiographic variables. Continuous and binary variables were standardized to Z‑scores prior to the analysis. PCA was performed on the correlation matrix using unrotated PC extraction. Eigenvalues, proportion of explained variance, and component loadings were examined to guide component retention. Based on the Kaiser criterion (eigenvalue >1) and clinical interpretability, the first 3 PCs (PC1–PC3) were retained a priori for further analyses. Component scores were calculated for each patient as linear combinations of the standardized original variables. The derived component scores were subsequently entered as continuous covariates into the Cox proportional hazards models to evaluate their association with 5‑year all‑cause mortality, both independently and in conjunction with sex. Additional models included sex‑component interaction terms, and sex‑stratified Cox models were fitted as exploratory analyses.
Results are reported as hazard ratios (HRs) with corresponding 95% CIs. For all analyses, the level of significance was set at a P value below 0.05. All statistical analyses were performed using StataNow/SE packages, versions 18.5 and 19.5 for Mac (StataCorp. 2023. Stata Statistical Software: Release 18).
Results
Baseline characteristics
The final unmatched cohort included 814 patients, of which 228 (28%) were women. Primary indication for PCI in both groups was chronic coronary syndrome (70.1%). In the overall population, women were significantly older (74 vs 70 y), more commonly suffered from hypertension and chronic kidney disease (CKD), while men had lower left ventricular ejection fraction (EF), more often had peripheral arterial disease (PAD), and a history of stroke. Angiographic analysis showed that men had more severe LM stenosis, larger mean diameter of implanted stents, and more often underwent PCI of LM‑LAD.
PSM resulted in 471 pairs, at median age of 70 (62–79) and 72 (66–80) years in men and women, respectively. There was a reduction of imbalances in most of the baseline characteristics, although significant differences, defined as standardized mean difference (SMD) equal to or above 0.2, regarding higher prevalence of PAD, chronic obstructive pulmonary disease, and previous stroke remained. Angiographic data analysis showed higher rates of distal LM stenosis, more severe LM stenosis, 2‑stent PCI technique, and LM‑LAD stenting in men.
IPTW resulted in a weighted pseudopopulation of 469 patients, of whom 131 (28%) were women. The reported IPTW sample size reflected the effective sample size (sum of stabilized weights), rounded to the nearest whole number. The analysis of baseline characteristics showed excellent reduction in disparities with differences regarding only higher rates of PAD and previous stroke in men. As for angiographic data, there were no differences in distal LM narrowing between the 2 groups, but men more frequently had more severe LM stenosis and underwent 2‑stent PCI and LM‑LAD stenting.
After restricting to complete cases for the PCA variables, 459 patients remained, including 123 women (27%). Seventeen standardized variables entered the PCA. The first 3 PCs explained 14.86%, 9.85%, and 8.09% of the variance, respectively (cumulative variance explained by PC1–PC3 = 32.8%; scree plot, full loadings, and eigenvalues are available in Supplementary material, Figure S9 and Tables S3–S6). PC1 represented a global clinical risk phenotype combining age, multimorbidity, and reduced EF, PC2 reflected a metabolic risk profile, and PC3 included anatomical and procedural characteristics.
Detailed information regarding baseline and procedural characteristics in overall and adjusted subgroups is available in Table 1 and Supplementary material, Table S7.
Variable | Unmatched | Propensity score matching | Inverse probability of treatment weighting | |||||||||
Men (n = 586) | Women (n = 228) | SMD, % | P value | Men (n = 471) | Women (n = 471) | SMD, % | P value | Men (n = 338) | Women (n = 131) | SMD, % | P value | |
Data are presented as number and percentage, median (interquartile range), or mean (SD).
Abbreviations: BMI, body mass index; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; DES, drug‑eluting stent; FKBI, final kissing balloon inflation; IABP, intra‑aortic balloon pump; LAD, left anterior descending artery; LM, left main artery; MI, myocardial infarction; PAD, peripheral arterial disease; SMD, standardized mean difference; VD, vessel disease; others, see Figure 1 | ||||||||||||
Age, y | 70 (62–79) | 74 (66–80) | –31.4 | 0.001 | 70 (62–79) | 72 (61–80) | –5.4 | 0.44 | 71 (62–79) | 72 (62–80) | 6.5 | 0.67 |
BMI, kg/m2 | 28 (25–31) | 28 (25–32) | –15.7 | 0.09 | 28 (25–31) | 27 (25–31) | 5 | 0.45 | 28 (25–31) | 27 (25–31) | –5.9 | 0.62 |
EuroSCORE II, % | 1.8 (1–3.7) | 2.4 (1.4–4.5) | –12.1 | 0.16 | 1.8 (1.1–3.8) | 2.4 (1.5–4.2) | –13.7 | 0.046 | 2 (1–3) | 2 (1–4) | –22.9 | 0.24 |
Ejection fraction, % | 45 (34–55) | 52 (40–58) | –48.7 | <0.001 | 45 (33–55) | 45 (34–55) | –1.7 | 0.81 | 49 (38–55) | 48 (36–55) | –5.9 | 0.68 |
Myocardial infarction | 167 (30.4) | 77 (36) | –12 | 0.17 | 143 (30.4) | 155 (32.9) | –5.4 | 0.4 | 101 (29.9) | 48 (36.5) | –14 | 0.17 |
Hypertension | 442 (83.2) | 190 (91.4) | –24.7 | 0.009 | 391 (83.2) | 396 (84.1) | –3.2 | 0.66 | 287 (84.9) | 109 (83.4) | 3.9 | 0.7 |
Heart failure | 309 (59.6) | 108 (52.6) | 14.1 | 0.11 | 280 (59.6) | 299 (63.5) | –7.9 | 0.22 | 189 (55.8) | 75 (57) | –2.4 | 0.82 |
Hyperlipidemia | 472 (90.9) | 193 (93.7) | –10.7 | 0.25 | 428 (90.9) | 425 (90.2) | 2.4 | 0.74 | 308 (91.1) | 119 (90.7) | 1.4 | 0.89 |
Atrial fibrillation | 133 (26.3) | 47 (21.7) | 10.8 | 0.23 | 124 (26.3) | 139 (29.5) | –7.5 | 0.28 | 76 (22.6) | 28 (21.1) | 3.6 | 0.73 |
PAD | 146 (29.6) | 39 (18.4) | 26.4 | 0.004 | 139 (29.6) | 77 (16.3) | 31.1 | <0.001 | 96 (28.5) | 22 (16.9) | 27.8 | 0.01 |
COPD | 50 (9.6) | 11 (3.4) | 25 | 0.01 | 45 (9.6) | 22 (4.7) | 20 | 0.004 | 26 (7.7) | 9 (7.2) | 1.8 | 0.86 |
CKD | 161 (30.6) | 88 (42.3) | –24.5 | 0.005 | 144 (30.6) | 143 (30.4) | 0.4 | 0.94 | 106 (31.2) | 45 (34.1) |
| 0.55 |
Previous PCI | 231 (42.8) | 88 (44) | –2.5 | 0.78 | 200 (42.8) | 191 (40.6) | 2.3 | 0.73 | 154 (45.6) | 53 (40.3) | 10.7 | 0.31 |
Previous MI | 235 (45.4) | 72 (38.3) | 14.4 | 0.11 | 209 (45.4) | 177 (37.6) | 13.1 | 0.049 | 152 (44.9) | 49 (37.1) | 15.8 | 0.13 |
Previous stroke | 54 (12) | 8 (5.3) | 24.1 | 0.02 | 53 (12) | 26 (5.5) | 20.5 | 0.004 | 39 (11.9) | 4 (3.1) | 33.8 | 0.01 |
Isolated LM lesion | 65 (12.4) | 27 (14.7) | –6.8 | 0.48 | 48 (12.4) | 59 (12.5) | –4.4 | 0.53 | 40 (11.8) | 16 (11.9) | –0.5 | 0.96 |
Distal LM lesion | 514 (87.7) | 199 (87.3) | 10.1 | 0.24 | 429 (91.1) | 402 (85.4) | 18.7 | 0.006 | 309 (91.3) | 115 (87.4) | 12.8 | 0.2 |
1‑VD excluding LM | 167 (34) | 56 (31.5) | 5.4 | 0.58 | 132 (34) | 126 (26.8) | 9.3 | 0.18 | 118 (34.8) | 44 (33.8) | 2.1 | 0.84 |
2‑VD excluding LM | 150 (32.2) | 69 (35.7) | –7.3 | 0.46 | 125 (32.2) | 160 (34) | –11.4 | 0.11 | 110 (32.6) | 46 (35.1) | –5.2 | 0.62 |
3‑VD excluding LM | 108 (21.4) | 37 (18.2) | 8 | 0.42 | 83 (21.4) | 80 (17) | 6.4 | 0.36 | 70 (20.8) | 25 (19.2) | 4.1 | 0.7 |
Rotational atherectomy | 74 (14.9) | 37 (19.4) | –12.1 | 0.16 | 70 (14.9) | 92 (19.5) | –12.4 | 0.06 | 40 (11.8) | 19 (14.5) | –7.9 | 0.44 |
Intravascular imaging | 235 (42) | 87 (42.3) | –0.5 | 0.96 | 198 (42) | 174 (36.9) | 10.3 | 0.11 | 141 (41.6) | 50 (38.1) | 7 | 0.5 |
IABP | 45 (5.1) | 9 (2.9) | 11.5 | 0.22 | 24 (5.1) | 23 (4.9) | 1.1 | 0.88 | 13 (4) | 5 (3.5) | 2.7 | 0.8 |
DES | 502 (90.8) | 201 (94.9) | –15.6 | 0.1 | 426 (90.8) | 429 (91.1) | –1 | 0.89 | 305 (90.3) | 116 (88.3) | 6.5 | 0.53 |
2‑stent technique | 109 (19.4) | 44 (17.9) | 3.9 | 0.66 | 91 (19.4) | 54 (11.5) | 20.4 | 0.001 | 66 (19.7) | 13 (10.2) | 26.9 | 0.01 |
LM stent diameter, mm | 3.81 (0.39) | 3.69 (0.43) | 21 | 0.02 | 3.79 (0.38) | 3.71 (0.43) | 19.9 | 0.002 | 3.82 (0.38) | 3.75 (0.43) | 17.3 | 0.18 |
LM‑LAD stenting | 452 (80.8) | 147 (67.2) | 31.1 | <0.001 | 378 (80.8) | 318 (67.5) | 30.5 | <0.001 | 267 (79.7) | 85 (64.5) | 34.2 | <0.001 |
FKBI | 332 (59.5) | 123 (54.6) | 9.9 | 0.27 | 279 (59.5) | 254 (53.9) | 11.2 | 0.09 | 207 (61.7) | 73 (55.5) | 12.7 | 0.22 |
Treatment of another lesion | 210 (37.4) | 76 (33.9) | 7.3 | 0.42 | 175 (37.4) | 165 (35) | 4.9 | 0.45 | 118 (35.1) | 44 (33.2) | 3.9 | 0.71 |
Potent P2Y12 | 84 (17.2) | 38 (20.4) | –8.2 | 0.36 | 76 (17.2) | 80 (17) | –2.4 | 0.71 | 61 (18) | 24 (18.4) | –1 | 0.92 |
Mortality analysis
In the 5‑year mortality analysis of the overall population, there was no difference in mortality between men and women (HR, 1.31; 95% CI, 0.99–1.73; P = 0.06). After adjusting for baseline confounders using PSM, we found markedly higher mortality rates among men (HR, 1.64; 95% CI, 1.28–2.11; P <0.001). The survival analysis following IPTW confirmed worse outcomes in men (HR, 1.71; 95% CI, 1.04–2.83; P = 0.04). In both PSM and IPTW populations, 30‑day mortality was slightly higher in women (P = 0.36 and P = 0.47, respectively) based on the Cox models restricted to 30‑day follow‑up. A crossover of survival curves was observed at approximately 45 days. The Cox proportional hazard assumption was not violated for all analyses (P = 0.3 for the overall population; P = 0.51 for PSM and P = 0.38 for IPTW). Mortality curves and outcomes for all analyses are presented in Figure 2. Inclusion of distal LM location as a covariate in the outcome models showed results consistent with the primary analysis, with higher 5‑year mortality in men (Supplementary material, Figure S10).
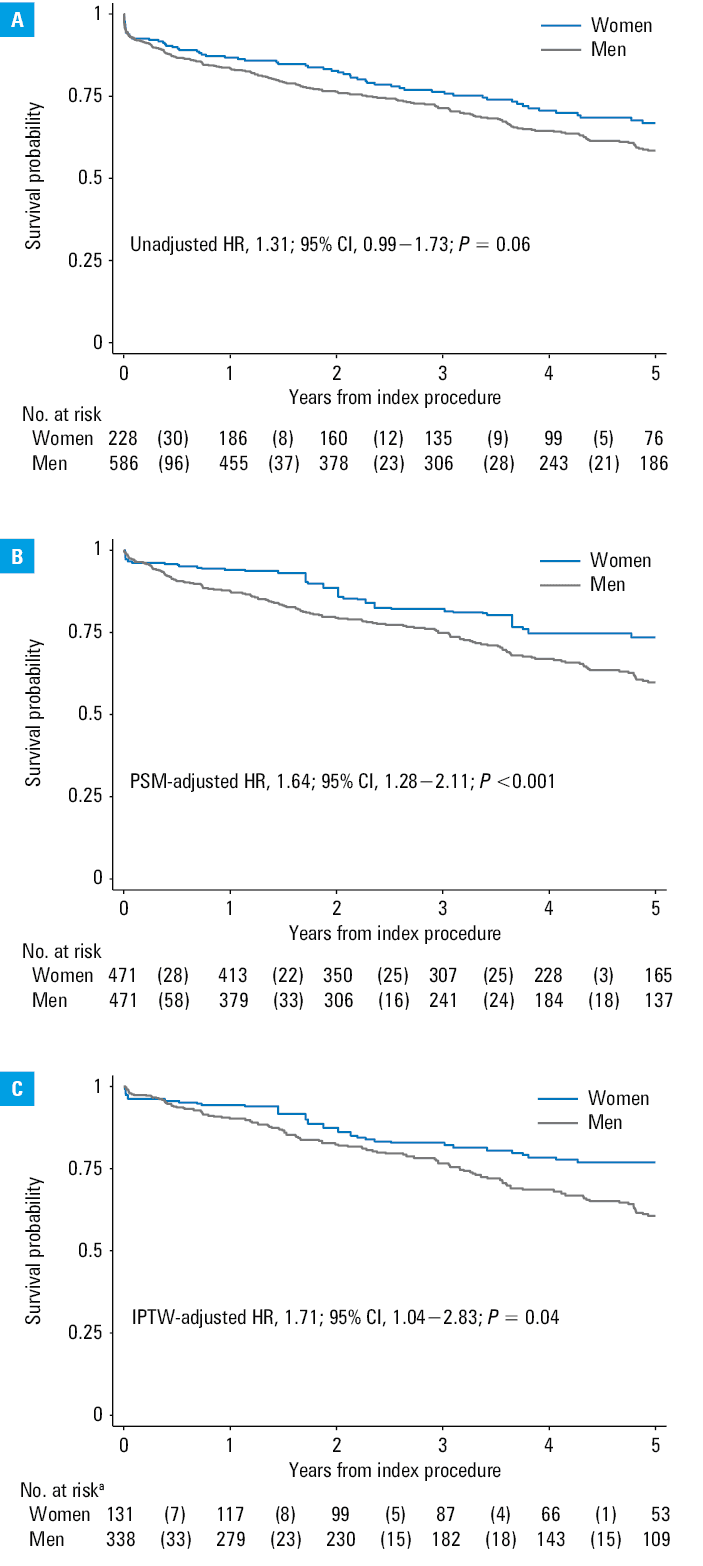
a The number of patients reflects the size of the IPTW‑generated pseudopopulation, rounded to the nearest whole number.
Abbreviations: HR, hazard ratio; others, see Figure 1
The Cox regression after PCA revealed substantial influence of PC1 (HR, 1.57 per 1‑SD increase; 95% CI, 1.39–1.76; P <0.001), whereas PC2 and PC3 were not independently associated with mortality. After model adjustment for PC1–PC3, the effect of sex remained insignificant (HR, 1.57; 95% CI, 0.99–2.48; P = 0.06). Interaction testing demonstrated no substantial PC‑by‑sex interaction (P = 0.75), indicating similar prognostic patterns in women and men. When analyzed separately, PC1 remained a strong predictor of mortality in both subgroups. Among women, PC1 was associated with a 53% increase in mortality per 1‑SD increment (HR, 1.53; 95% CI, 1.14–2.06; P = 0.004), and among men, PC1 showed a comparable effect (HR, 1.57; 95% CI, 1.38–1.79; P <0.001). Neither PC2 nor PC3 predicted mortality in either sex. Detailed results are presented in Supplementary material, Table S5.
Subgroup and interaction analyses
Subgroup analyses performed in the PSM and IPTW cohorts showed consistent directional effects favoring women across most subgroups (Figure 3).
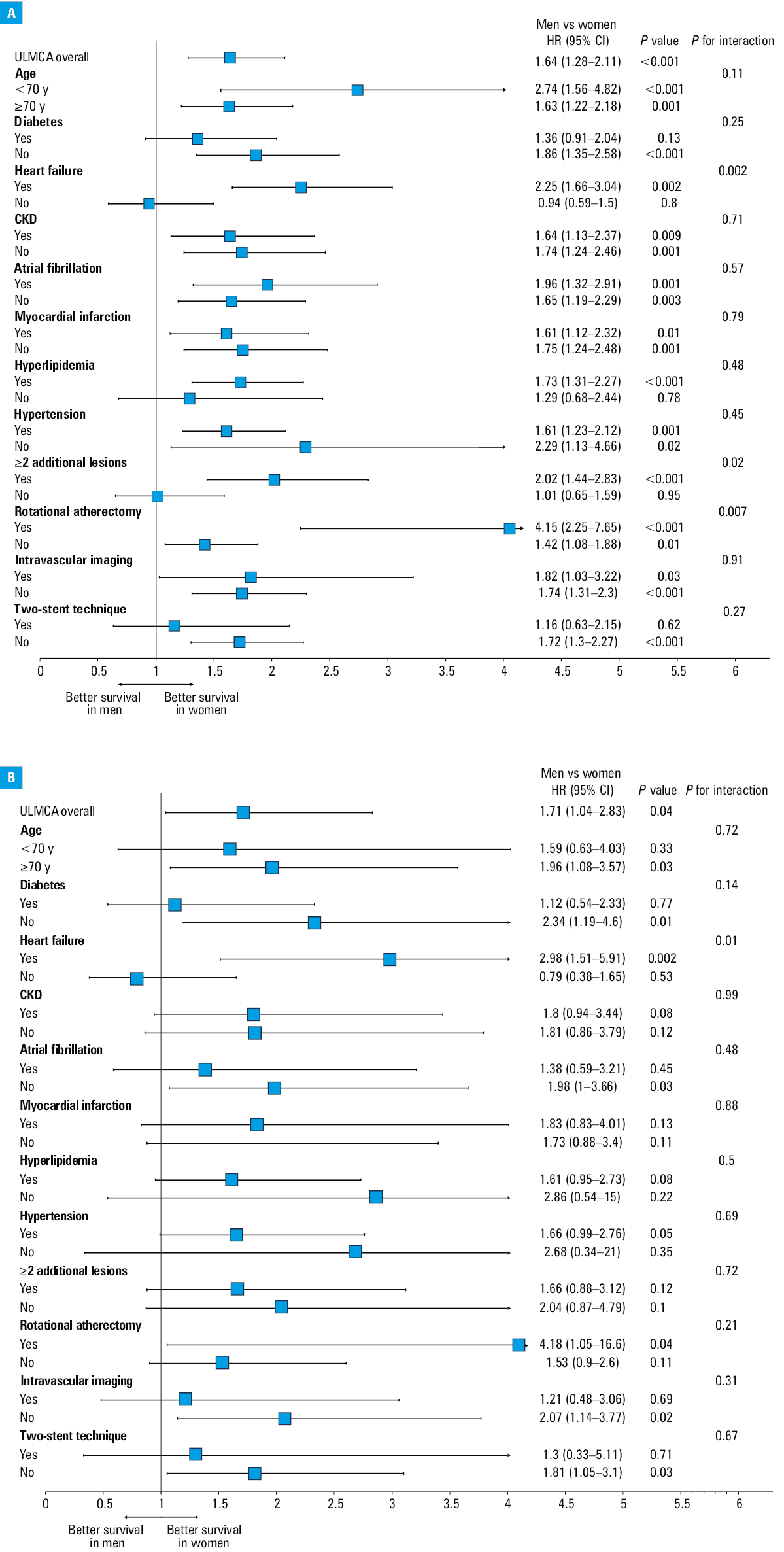
Abbreviations: ULMCA, unprotected left main coronary artery; others, see Figures 1 and 2 and Table 1
Formal interaction testing demonstrated a significant sex‑by‑heart failure (HF) interaction in both cohorts (P = 0.002 for interaction in PSM and P = 0.01 for interaction in IPTW). In the PSM cohort, additional significant interactions were observed for rotational atherectomy (RA; P = 0.007 for interaction) and treatment of at least 2 lesions (P = 0.02 for interaction), indicating a differential effect of sex on mortality across these subgroups.
Forest plots showing outcomes in selected subgroups after PSM and IPTW are presented in Figure 3. In additional interaction analyses, significant sex interactions with distal lesion location and stenosis severity were observed in the PSM‑adjusted model but not in the unadjusted and IPTW‑weighted analysis (Supplementary material, Figure S11).
Discussion
Our study, based on the largest single‑center registry of percutaneous revascularization procedures for LMCA disease in Poland, offers novel insights into sex‑based and comorbidity‑related differences in outcomes following PCI. The key findings of this real‑world cohort analysis are outlined below. First, prior to PSM, there was no difference in 5‑year mortality between men and women. Following PSM, mortality was significantly higher in men. After IPTW adjustment, the association remained directionally consistent and was significant. Importantly, the consistency of the sex effect across multiple analytical strategies strengthens the robustness of the observed association between male sex and worse long‑term survival. Second, a crossover in survival curves was observed approximately 45 days postprocedure, reflecting higher early mortality in women, although this difference did not reach significance. Third, the subgroup and moderation analyses showed consistent directional trends toward better prognosis in women. Fourth, among the patients with HF, those treated with RA, and those with multivessel disease, men had worse outcomes than women.
While most contemporary therapies for CAD demonstrate efficacy across sexes, the foundational evidence largely originates from studies with under‑representation of women. These disparities have drawn increasing attention from the cardiovascular community. The European Society of Cardiology has emphasized the importance of integrating sex‑informed approaches into cardiovascular diagnostics and management. Taken together, there is growing recognition that contemporary medicine must move beyond the “one‑size‑fits‑all” paradigm toward more personalized approaches to care.7
Sex‑based survival differences
Before adjustment, all‑cause mortality did not differ between the 2 groups. However, after applying PSM, long‑term mortality was significantly greater in men, and this association persisted also following IPTW. These findings contrast with those of the IRIS‑MAIN (Interventional Cardiology Research In‑cooperation Society‑left Main revascularization) registry, in which all‑cause death was similar in women and men during long‑term follow‑up after PCI for LMCA.12 In the MITO (Milan and New‑Tokyo) registry, propensity score adjustment also showed comparable rates of all‑cause death between sexes.13 Furthermore, the PRECOMBAT trial (Premier of Randomized Comparison of Bypass Surgery versus Angioplasty Using Sirolimus‑Eluting Stent in Patients with Left Main Coronary Artery Disease) found no sex‑related differences in the long‑term risk of major adverse cardiac and cerebrovascular events at 10 years after revascularization for LMCA disease.14 The SYNTAXES (SYNTAX Extended Survival) study revealed that women had a higher crude rate of all‑cause mortality at 10 years following CABG or PCI revascularization than men, but being a woman was not an independent predictor of 10‑year mortality after adjustment for baseline characteristics.10 Notably, women comprised only around 25% of the enrolled participants, which may have limited the ability to identify sex‑related differences in outcomes.
In our cohort, women were older and more frequently presented with hypertension, consistent with previous large‑scale trials.10,12 Although SYNTAX scores were not assessed in our study, both the EXCEL and SYNTAXES trials demonstrated that women generally exhibited lower angiographic complexity than men, despite a higher prevalence of conventional cardiovascular risk factors.10,15 The underlying mechanisms remain incompletely understood, but potential contributors include hormonal and genetic factors, as well as the size of the coronary vessels.10 In our study, EuroSCORE II remained higher among women even after PSM, and a similar pattern was observed in the PRECOMBAT cohort.14 Conversely, men were more likely to present with PAD and a history of stroke. The higher prevalence of vascular comorbidities among men likely reflects a greater baseline burden of systemic atherosclerosis, and may partially contribute to their increased long‑term mortality risk, as also indicated by the PCA. Prior stroke has been associated with a higher risk of long‑term cerebrovascular and cardiovascular events after PCI,16 while pooled analyses of randomized trials have shown that concomitant PAD is linked to increased adverse cardiovascular outcomes and mortality.17 Another potential mechanism may relate to the higher prevalence of smoking among men. In a contemporary cohort of patients with ST‑segment elevation myocardial infarction (MI) treated with primary PCI, smokers were more often male, and although unadjusted analyses suggested more favorable mid‑term outcomes, adjustment for baseline characteristics identified smoking as an independent predictor of 36‑month mortality.18 Variation in the use and intensity of guideline‑directed medical therapy may also contribute to sex‑specific differences in long‑term outcomes. Previous studies indicate that women with CAD are less likely to receive optimal pharmacologic treatment, including suboptimal dosing of antithrombotic agents, and less frequently achieve target statin therapy despite its similar cardiovascular benefit across sexes.3,4,8 In our registry, no significant sex differences were observed in the use of potent P2Y12 inhibitors; however, detailed data on other medications were not available, preventing a more comprehensive evaluation of potential treatment disparities.
In addition to clinical differences, we observed anatomical disparities between the sexes. Men more frequently presented with more severe LMCA stenosis, which may reflect a more advanced stage of coronary atherosclerosis. Distal LMCA involvement was the predominant lesion location in our cohort (about 87%), consistent with previous LMCA PCI registries, and its distribution was similar in men and women in both the overall and IPTW‑adjusted populations.
Taken together, these discrepancies may reflect heterogeneity in anatomical complexity and disease burden across cohorts; importantly, residual or unmeasured confounding cannot be excluded despite the use of multiple statistical adjustment strategies.
Periprocedural outcomes and early mortality
Periprocedural mortality was numerically higher in women, although this difference did not reach significance. The early separation of mortality curves followed by a crossover at approximately 45 days suggests that distinct mechanisms may underlie early vs late mortality after LMCA PCI. Although detailed data on procedural complications were not systematically captured in our registry, early competing hazards, such as bleeding or vascular complications, may contribute to early mortality differences between sexes. Similar trends were reported in the EXCEL trial, where women undergoing PCI experienced higher rates of periprocedural ischemic and bleeding complications,15 and in the British Cardiac Intervention Society national PCI registry,19 which demonstrated higher in‑hospital mortality and the risk of major bleeding in women despite less complex CAD. Beyond baseline differences, the elevated bleeding risk in women may be partly explained by biological factors, including estrogen‑mediated modulation. Post‑PCI bleeding has been associated with a 3- to 10‑fold increase in both 30‑day and 1‑year mortality, as well as higher rates of MI and stroke.20 In our cohort, even after PSM, stent diameters were larger in men. External studies have demonstrated that women generally present with smaller reference vessel diameters that complicate complex coronary interventions.3 Importantly, the excess risk of complications in women persisted after adjustment for body surface area and nominal stent diameter, indicating that vessel size alone does not fully explain the observed disparities.20 Collectively, these findings support the rationale for sex‑tailored procedural strategies to optimize stent expansion and mitigate periprocedural risk.
Heart failure and rotational atherectomy
In our study, among the patients with HF and RA, worse outcomes were observed in men. The association between HF and adverse prognosis in men is consistent with prior evidence, including a comprehensive meta‑analysis of 94 cohort studies, demonstrating lower rates of all‑cause mortality, cardiovascular death, and HF‑related hospitalizations in women than in men.21
Men are more likely to develop HF with reduced EF (HFrEF), whereas the prevalence of HF with preserved EF (HFpEF) seems higher in women.22 This distinction may have prognostic implications. A Chinese cohort study found that HFrEF was associated with nearly double 5‑year mortality risk than HFpEF.23 Furthermore, among patients with HFrEF, recent data from the Korean Acute Heart Failure Registry indicated that men had an independently higher risk of cardiovascular death, a pattern not observed in the HFpEF population.24 Although our analysis did not differentiate between HFrEF and HFpEF, these phenotype‑specific considerations may partly explain the observed sex‑related differences and warrant further investigation. Beyond HF, another domain in which men exhibited poorer outcomes in our cohort was RA. This observation diverges from some previous studies. For example, Ford et al25 reported a higher incidence of procedural complications in women undergoing RA, whereas adjusted overall long‑term survival free of major adverse cardiac events was comparable between sexes, underscoring the uncertainty regarding sex‑specific prognostic implications in RA.
In our study, the worse outcomes in men may be attributable to greater lesion complexity, particularly a higher calcific burden, as further suggested by the observation of poorer outcomes among men with concomitant multivessel disease. Coronary calcification is more frequently observed in men and increases the technical difficulty of PCI. Extensive calcification can hinder device delivery and optimal stent deployment, potentially contributing to procedural complications.26
Myocardial infarction and chronic kidney disease
In our analysis, we observed similar outcomes in men with MI and those with CKD, as compared to women. Both subgroups are of significant clinical importance, as previous reports showed sex‑based disparities in health care. For instance, elements contributing to worse outcomes among women with MI may include more diffuse symptom presentation, lower attribution to cardiac causes, and social responsibilities, such as caregiving, which may collectively defer prompt care‑seeking and treatment initiation.27
Our findings align with prior evidence demonstrating that when PCI techniques are applied, sex does not independently predict adverse outcomes. In a cohort of patients with acute coronary syndrome undergoing PCI, unadjusted 1‑year mortality was higher among women; however, after multivariable adjustment, being a woman was not associated with an increased risk of death or major adverse cardiovascular events within 1 year.28 In contrast, a large registry‑based analysis of MI prognosis has reported worse outcomes among women, both during hospitalization and long‑term follow‑up.29 A potential explanation may be longer delays from symptom onset to reperfusion in women with acute coronary syndromes, including both prehospital intervals related to later presentation to medical care, and in‑hospital waits driven by system‑level factors.27,30
CKD is a well‑established cardiovascular risk factor. Despite its high prevalence among patients undergoing coronary angiography, individuals with CKD have been consistently excluded from or markedly under‑represented in pivotal trials on revascularization and medical therapy for IHD. Seminal studies, such as SYNTAX (TAXUS Drug‑Eluting Stent Versus Coronary Artery Bypass Surgery for the Treatment of Narrowed Arteries), which have shaped contemporary practice, exemplify this persistent evidence gap.31
In our analysis, long‑term survival did not differ in men and women with CKD, a finding consistent with prior work of Ndrepepa et al32, who also showed, in a large cohort of patients undergoing PCI with up to 10 years of follow‑up, that the adverse prognostic impact of CKD on all‑cause mortality was comparable across sexes, with no evidence of a sex‑specific interaction. Complementary data from the Coronary Artery Disease and Renal Failure registry33 further confirmed that sex was not an independent predictor of long‑term mortality in patients with CAD and impaired renal function, with comparable survival observed in women and men across all CKD stages.
Principal component analysis interpretation
PCA, performed as an exploratory complementary analysis, identified a dominant axis of clinical risk, reflecting multimorbidity and frailty, which were the strongest predictors of 5‑year mortality, and showed a comparable prognostic effect in women and men. The absence of significant PC‑by‑sex interactions indicates similar risk gradients across sexes.
Importantly, inclusion of PCA components did not attenuate the sex effect observed in PSM and IPTW analyses, suggesting that differences in baseline clinical risk do not explain the residual sex‑related mortality difference. This finding implies that other factors, such as anatomical, procedural, or biological sex‑specific mechanisms not captured by PCA, may contribute to outcome disparities.
Overall, these supplemental results support the concept that while global clinical risk strongly determines prognosis, it does not fully account for sex‑related differences in long‑term outcomes following contemporary interventional management.
Strengths and limitations
Main limitations of the BIA‑LM registry were reported earlier,2,11 and are inherent to the observational design of the study. The first and most important issue is related to the baseline differences between the analyzed groups. However, in order to reduce bias, we used 3 statistical methods, PSM, IPTW, and PCA, which significantly reduced disparities and enhanced the value of our findings. Although these approaches are well established, we are aware that unmeasured factors may still remain and influence the results. It is important to acknowledge that this registry originates from a single, high‑volume tertiary center, which supported reliable data, but caution is required when extrapolating the findings or comparing them with other studies. Moreover, the study period spans the years 2007–2022, during which substantial advancements in PCI techniques, stent technology, adjunctive pharmacotherapy, and intravascular imaging occurred. These temporal changes may have influenced procedural strategies and clinical outcomes, and should be considered when interpreting the results. Selection of all‑cause mortality as a primary end point ensures robustness of findings and facilitates comparison with other registries. However, sex‑at‑birth is known to influence factors beyond mortality, such as vascular complications, which were not available for this analysis.
Moreover, data on certain clinical variables, including the SYNTAX score, and medication adherence were unavailable, potentially affecting risk stratification and subgroup interpretation. In addition, although the analyses stratified by HF, multivessel disease, and RA suggested potentially meaningful trends, these observations should be interpreted with caution as exploratory and hypothesis‑generating only. The study also did not provide information on the number of patients referred for CABG by a heart team, those who declined surgery, or those managed conservatively, including whether these pathways differed between women and men. While such data could provide additional context, the registry was designed to assess long‑term outcomes in patients who underwent PCI, rather than to evaluate sex‑related differences in treatment selection.
Conclusions
The analysis of the largest single‑center LMCA PCI registry in Poland showed that after adjustment for confounders, men may have worse prognosis than women. Men were at a particularly increased risk of mortality among the patients with HF, multivessel disease, and those undergoing RA. The outcomes of this study suggest the need for further consideration of sex‑at‑birth as one of the key factors of treatment personalization and qualification for invasive treatment. Nevertheless, due to the observational nature of the study, all causal inference must be drawn with caution.
- Aggarwal NR, Patel HN, Mehta LS, et al. Sex differences in ischemic heart disease: advances, obstacles, and next steps. Circ Cardiovasc Qual Outcomes. 2018; 11: e004437. | Crossref
- Kralisz P, Dąbrowski EJ, Dobrzycki S, et al. Long‑term impact of diabetes on mortality in patients undergoing unprotected left main PCI: a propensity score‑matched analysis from the BIA‑LM registry. Cardiovasc Diabetol. 2025; 24: 175. | Crossref
- Gaudino M, Di Franco A, Cao D, et al. Sex‑related outcomes of medical, percutaneous, and surgical interventions for coronary artery disease: JACC Focus Seminar 3/7. J Am Coll Cardiol. 2022; 79: 1407‑1425. | Crossref
- Venditti V, Bleve E, Morano S, Filardi T. Gender‑related factors in medication adherence for metabolic and cardiovascular health. Metabolites. 2023; 13: 1087. | Crossref
- Kampka Z, Szczerba R, Bula K, et al. Clinical characteristics and outcomes of young patients with acute myocardial infarction: the YAMI registry. Pol Arch Intern Med. 2025; 135: 16921. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION