Criss‑cross heart (CCH) is a rare congenital anomaly characterized by crossing of the atrioventricular inflow streams due to abnormal spatial orientation of the ventricles.1-4 Adult presentation is exceptional, particularly in the absence of significant associated structural abnormalities.4,5
A 35‑year‑old man with no prior cardiovascular history presented with several hours of stabbing retrosternal chest pain and severe hypertension (systolic blood pressure of up to 195 mm Hg). Twelve‑lead electrocardiography showed sinus rhythm with first‑degree atrioventricular block and an indeterminate frontal QRS axis (Figure 1A). The high‑sensitivity troponin T level was mildly elevated but stable; creatine kinase and its muscle‑brain isoform levels were normal. The level of N‑terminal pro–B‑type natriuretic peptide was slightly elevated.
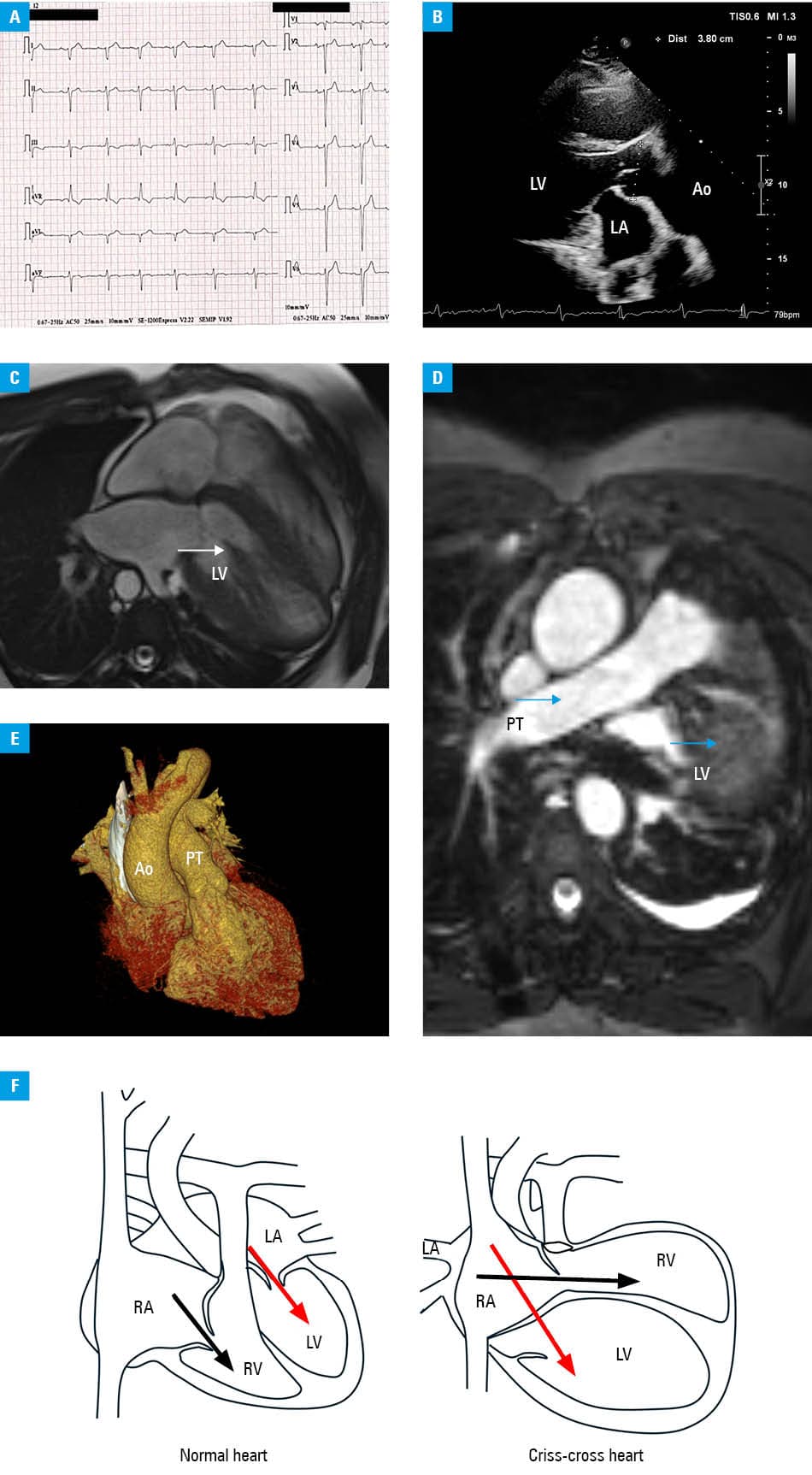
Abbreviations: Ao, aorta; LA, left atrium; LV, left ventricle; PT, pulmonary trunk; RA, right atrium; RV, right ventricle
Transthoracic echocardiography was technically limited by poor acoustic windows and an unusual cardiac position, with the apex displaced posteriorly within the left hemithorax (Figure 1B). Off‑axis imaging and foreshortening likely contributed to the underestimation of left ventricular (LV) systolic function, which was visually assessed as reduced (LV ejection fraction [LVEF], 35%–40%), raising suspicion of cardiomyopathy. Given the discordance between the echocardiographic findings and the atypical cardiac position and electrical axis, cardiac magnetic resonance (CMR) was performed as the next diagnostic step.
CMR demonstrated crossing atrioventricular inflow streams with abnormal ventricular alignment, consistent with CCH, and preserved ventricular size (Figure 1C and 1D). No ventricular septal defect or other major structural abnormalities were identified. CMR excluded active myocarditis (no myocardial edema or late gadolinium enhancement) and showed preserved LVEF (52%).
Coronary computed tomography excluded obstructive coronary artery disease and confirmed normal aortic arch morphology with a tortuous descending aorta (Figure 1E). The patient was managed conservatively with antihypertensive therapy and scheduled for outpatient follow‑up.
This case illustrates that CCH in adults may be hemodynamically uncomplicated and remain undiagnosed until incidental detection. It also highlights that reduced LVEF on echocardiography may result from suboptimal imaging conditions, including foreshortening and off‑axis views, rather than true systolic dysfunction. Multimodality imaging, particularly CMR, plays a key role in clarifying cardiac anatomy and ventricular function in such cases, and may prevent misdiagnosis of cardiomyopathy and unnecessary invasive testing (Figure 1C, 1D, and 1F).
- Ren S, Ma C, Li S. Criss‑cross heart with double‑outlet right ventricle, subpulmonary ventricular septal defect, and bicuspid pulmonary valve. J Clin Ultrasound. 2019; 47: 315‑318. | Crossref
- Kasar T, Ayyıldız P, Türkvatan A, et al. Criss‑cross heart with dextrocardia and transposition of the great arteries: a rare pathology. Turk Kardiyol Dern Ars. 2016; 44: 91. | Crossref
- Taksande AM. Echocardiographic recognition of a criss‑cross heart with double outlet right ventricle. Images Paediatr Cardiol. 2013; 15: 3‑7. | Crossref
- Hoffman P, Szymański P, Lubiszewska B, et al. Crisscross hearts in adults: echocardiographic evaluation and natural history. J Am Soc Echocardiogr. 2009; 22: 134‑140. | Crossref
- Lewin D, Van Praet KM, Nersesian G, et al. Transcatheter aortic valve replacement in a patient with criss‑cross heart. JACC Case Rep. 2022; 4: 934‑940. | Crossref
ARTICLE INFORMATION