Reversible splenial lesion syndrome presenting with syncope and fever in a 26-year-old woman

 CC BY 4.0
CC BY 4.0
Reversible splenial lesion syndrome presenting with syncope and fever in a 26-year-old woman
A 26‑year‑old woman with no significant medical history was admitted with a 3‑day fever, cough, progressive weakness, and recurrent episodes of transient bilateral visual blackouts (presyncope), which she experienced 1 day prior to admission. Each lasted 5 to 10 seconds and occurred 4–5 times. The episodes were not associated with loss of consciousness, seizure activity, or palpitations. On admission, physical examination showed fever (38.2 °C), mild pharyngeal erythema, and normal blood pressure. Neurological examination demonstrated no focal deficits, normal cranial nerves, and intact coordination.
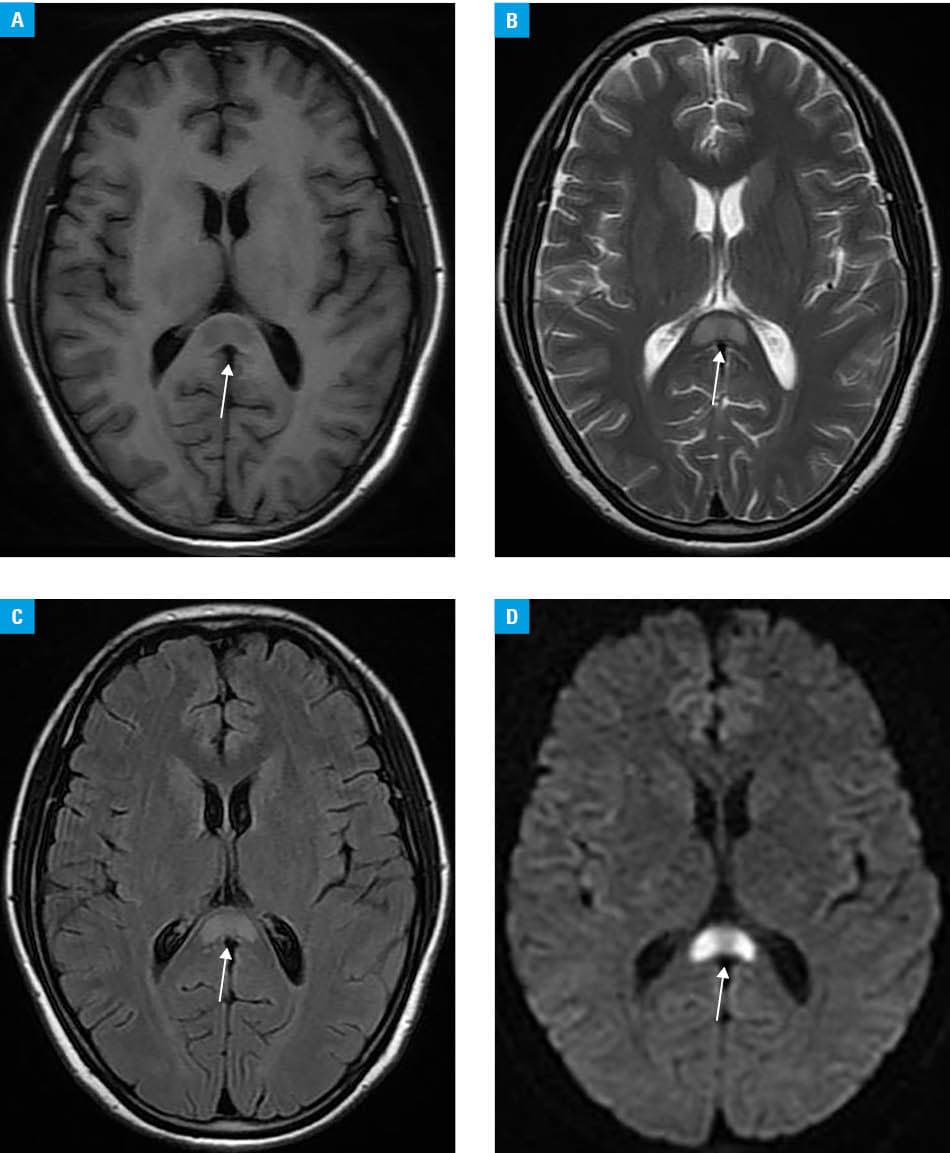
Laboratory test results identified elevated white blood cell count (12.4 × 109/l; reference range [RR], 3.5–9.5 × 109/l) and C‑reactive protein level (48 mg/l; RR <5 mg/l). Chest radiography was unremarkable. Brain magnetic resonance imaging (MRI) performed on the second day of hospital stay demonstrated a well‑circumscribed oval lesion in the splenium of the corpus callosum, appearing hyperintense on diffusion‑weighted imaging, with corresponding low apparent diffusion coefficient values, and hyperintense on T2‑weighted fluid‑attenuated inversion recovery sequences. No contrast enhancement was observed. The findings were consistent with reversible splenial lesion syndrome (RESLES; Figure 1A–1D).
Lumbar puncture showed mild lymphocytic pleocytosis (15 cells/μl; RR, 0–5 cells/μl) with normal protein and glucose levels. Polymerase chain reaction testing for common respiratory viruses from nasopharyngeal swab was positive for influenza A virus. Electrocardiography, transthoracic echocardiography, and 24‑hour Holter monitoring showed no abnormalities. The patient received supportive care with hydration and antipyretics. Her fever resolved within 48 hours, and the episodes of visual blackout ceased completely by day 3 of hospitalization. Follow‑up brain MRI performed 2 weeks after admission showed complete resolution of the splenial lesion. At 3‑month follow‑up, the patient remained asymptomatic, with no recurrence of neurological symptoms.
RESLES is a clinico‑radiological entity characterized by transient lesions in the splenium of the corpus callosum on MRI, often associated with various etiologies, including infection, metabolic disturbances, and antiepileptic drug withdrawal.1 While the condition typically follows a benign course with complete resolution, its clinical presentation can be diverse and occasionally mimic more serious neurological disorders.
Although the exact prevalence of RESLES remains unclear due to its relatively recent recognition and potential underdiagnosis, it has been increasingly reported worldwide. The largest retrospective study to date identified 130 pediatric cases over a 6‑year period in a single region of China, suggesting that RESLES is not extremely rare, particularly in the setting of infection‑related encephalopathy / encephalitis.1 The splenium of the corpus callosum appears particularly vulnerable to metabolic and inflammatory insults due to its high water content and unique vascular supply.2 In our patient, influenza A infection likely served as the triggering event, with fever potentially contributing to the pathogenesis. Although RESLES is frequently associated with encephalopathy or altered mental status, isolated visual symptoms, as described here, are less common but should be recognized to avoid unnecessary diagnostic interventions.3
The condition must be differentiated from acute disseminated encephalomyelitis, high‑grade glioma, and cerebral infarction. The key distinguishing features are the absence of contrast enhancement, a strictly reversible nature of the lesion on follow‑up imaging, and a favorable clinical course.1 Importantly, in young adults with cardiovascular risk factors, the presentation with syncope or presyncope may initially raise concerns for cardiac or cerebrovascular causes, as in this case. Awareness of RESLES can prevent unnecessary invasive procedures and prolonged hospitalization.
- Chen H, Yu X, Chen Y, et al. Reversible splenial lesion syndrome in children: a retrospective study of 130 cases. Front Neurol. 2023; 14: 1241549. | Crossref
- He X, Lin Y, Chen J, et al. Reversible splenial lesion syndrome associated with Graves’ disease and hepatic dysfunction: a case report. Front Neurosci. 2025; 19: 1691469. | Crossref
- Oey NE, Shwe MP, Wang AD, et al. Influenza B–associated mild encephalopathy with reversible splenial lesion in an adult: a case report. Neurol Int. 2025; 17:194. | Crossref
ARTICLE INFORMATION