Pregnancy-onset, treatment-refractory granulomatosis with polyangiitis with progressive severe tracheobronchial stenosis: remission achieved with avacopan-based combination therapy

 CC BY 4.0
CC BY 4.0
Pregnancy-onset, treatment-refractory granulomatosis with polyangiitis with progressive severe tracheobronchial stenosis: remission achieved with avacopan-based combination therapy
A 23‑year‑old woman with a history of seronegative juvenile idiopathic arthritis and Hashimoto thyroiditis presented at 7 months’ gestation with epistaxis, nasal crusting, hearing loss, and hemoptysis. Juvenile idiopathic arthritis had been diagnosed at the age of 16 years, treated with methotrexate for approximately 1 year, and discontinued more than 1 year before conception. During pregnancy, the patient received no disease‑modifying antirheumatic drugs or thyroid‑directed therapy, as Hashimoto thyroiditis remained euthyroid. Due to progressive respiratory failure, emergency cesarean section was performed, followed by admission to an intensive care unit. Chest computed tomography showed multiple cavitating pulmonary nodules (Figure 1A and 1B), with the largest in the left upper lobe measuring 100 mm × 67 mm × 78 mm, and bronchial ulcerations. Head and neck computed tomography demonstrated pansinusitis involving the frontal, ethmoid, sphenoid, and maxillary sinuses (Figure 1C), alongside fluid‑filled temporal bone pyramids (Figure 1D). Laboratory test results showed proteinase 3‑antineutrophil cytoplasmic antibodies positivity (56 IU/ml) and proteinuria (2+), while sediment examination showed 20–50 fresh erythrocytes / high‑power field and 3–5 dysmorphic erythrocytes / high‑power field, consistent with glomerulonephritis. Bronchial biopsy confirmed necrotizing vasculitis with prominent eosinophilic infiltrates and areas of necrosis surrounded by macrophage clusters, establishing a diagnosis of granulomatosis with polyangiitis (GPA). No relevant environmental, occupational, infectious, toxic, or drug‑related exposures preceding GPA onset were identified.
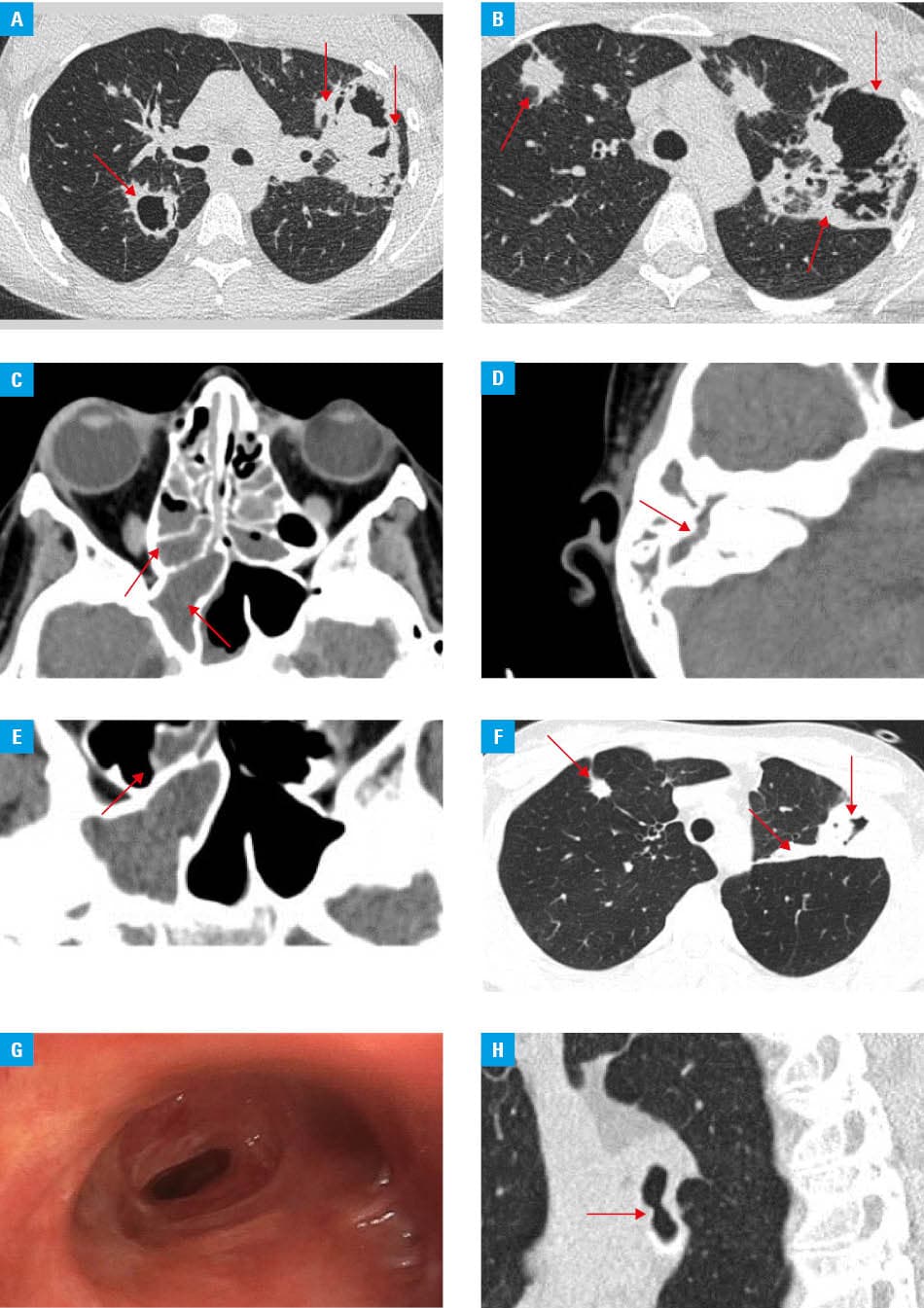
Induction therapy included methylprednisolone pulses and 6 doses of cyclophosphamide. Despite treatment, the patient experienced multiple relapses within 4 months, characterized by fever, pleuritic pain, recurrent hemoptysis, and progressive sinopulmonary lesions (Figure 1E), necessitating treatment escalation to rituximab and periodic intravenous immunoglobulin administration. Although parenchymal lesions regressed (Figure 1F), the course was complicated 10 months from onset by critical membranous tracheal stenosis (narrowed to 2 mm; Figure 1G) and bilateral main bronchi obstruction (Figure 1H), requiring tracheostomy, emergent bronchoscopic dilations, and temporal stenting. These attempts were complicated by bilateral pneumothorax and mediastinal emphysema, leading to intensive care unit readmission.
Due to the refractory airway involvement, the patient required repeated mechanical interventions despite multiple intravenous glucocorticoid pulses and local steroid injections in the preceding months. Repeat bronchial biopsy confirmed persistent mucosal inflammation. This fact led to an introduction of a new treatment protocol with avacopan (a C5a receptor antagonist) combined with a restarted cyclophosphamide regimen (reaching a cumulative dose of 10.7 g). Following avacopan initiation, clinical stabilization was achieved. Auxiliary argon plasma ablation of the left main bronchus was additionally performed but no further steroid injection was necessary. Glucocorticoids were successfully discontinued by month 22. At month 26, the patient remains in clinical remission, with stable airway lumen and significantly improved exercise tolerance, limiting tracheostomy tube usage to strenuous activities, while on maintenance therapy with avacopan and rituximab.
This case illustrates a rare but highly morbid GPA phenotype with rapidly progressive multilevel tracheobronchial stenosis. Airway involvement in GPA may follow a course partly dissociated from systemic inflammatory control, which may explain progression despite regression of parenchymal lung lesions and escalation of immunosuppression.1,2 Current European Alliance of Associations for Rheumatology recommendations support rituximab or cyclophosphamide for organ- or life‑threatening antibody‑associated vasculitis, with glucocorticoid minimization whenever possible.3 Avacopan has demonstrated efficacy as a steroid‑sparing agent for remission induction and sustained remission in antibody‑associated vasculitis, although data specifically addressing fibrotic airway stenosis remain limited.4 Recent Food and Drug Administration and European Medicines Agency communications on avacopan, including serious liver safety signals and ongoing review of ADVOCATE trial data, should be considered when interpreting its use. Our case suggests that, in refractory GPA, avacopan combined with renewed cyclophosphamide, rituximab, and repeated interventional bronchoscopy may enable remission and glucocorticoid withdrawal.2-5
- Brożek‑Mądry E, Szopiński K, Życińska K, Krzeski A. Radiological markers of granulomatosis with polyangiitis with nasal involvement. Pol Arch Intern Med. 2021; 131: 649‑657. | Crossref
- Girard C, Charles P, Terrier B, et al. Tracheobronchial stenoses in granulomatosis with polyangiitis (Wegener’s): a report on 26 cases. Medicine (Baltimore). 2015; 94: e1088. | Crossref
- Hellmich B, Sanchez‑Alamo B, Schirmer JH, et al. EULAR recommendations for the management of ANCA‑associated vasculitis: 2022 update. Ann Rheum Dis. 2024; 83: 30‑47. | Crossref
- Jayne DRW, Merkel PA, Schall TJ, Bekker P; ADVOCATE Study Group. Avacopan for the treatment of ANCA‑associated vasculitis. N Engl J Med. 2021; 384: 599‑609. | Crossref
- Berke I, Keller F, Untersulzner C, et al. Systematic review of efficacy and safety of avacopan in real‑world clinical practice. Kidney Int Rep. 2025; 11: 103753. | Crossref
ARTICLE INFORMATION