Atrial fibrillation (AF) is still too often framed as a disorder of rhythm alone. In clinical practice, however, AF rarely exists in isolation. It commonly coexists with vascular disease, renal dysfunction, diabetes, obesity, and heart failure, creating a phenotype that extends well beyond the electrocardiogram.1,2 Contemporary conceptual frameworks have formalized this overlap within the construct of cardiovascular‑kidney‑metabolic (CKM) syndrome, emphasizing the biological interdependence of cardiovascular disease, chronic kidney disease, and metabolic dysfunction.1
The prospective cohort study by Mantovani et al,3 published in this issue of Polish Archives of Internal Medicine, is a timely and important contribution. By examining CKM multimorbidity in 1236 patients with AF, the authors shift the discussion from AF as an isolated arrhythmia to AF as a manifestation of systemic diseases. More than half of the cohort had at least 1 CKM condition, underscoring how deeply AF is embedded in multisystem illness.
This reframing is not merely conceptual. Modern AF care has increasingly moved toward structured, holistic management beyond rhythm alone, as reflected in the Asia Pacific Heart Rhythm Society, European Society of Cardiology, and American College of Cardiology / American Heart Association AF guidelines recommending integrated care models, such as ABC (Atrial fibrillation Better Care), SOS (Stroke risk reduction, Optimize comorbidities and risk factors, Symptom Management) or CARE (Comorbidity and risk factor management, Avoidance of stroke and thromboembolism, Rate and rhythm control, Evaluation and dynamic reassessment) pathways.4 Mantovani et al3 extend that logic by suggesting that the substrate of AF itself may be inseparable from the CKM continuum.
The most compelling finding of the study is the clear stepwise relationship between CKM burden and adverse outcomes. Compared with patients without CKM conditions, those with 1, 2, and 3 CKM conditions had progressively higher adjusted risk of the composite end point of all‑cause death, acute coronary syndrome, ischemic stroke or transient ischemic attack, and hospitalization for heart failure. The adjusted hazard ratio rose from 1.56 in patients with 1 CKM condition to 1.98 and 2.55 in those with 2 and 3 conditions, respectively, indicating that CKM burden is not merely common in AF, but clinically and prognostically meaningful.3
The phenotype analysis adds important nuance. Cardiovascular‑containing phenotypes appeared to confer the greatest excess risk, whereas isolated metabolic disease was associated with a comparatively lower‑risk profile.3 This heterogeneity suggests that not all CKM constellations are equivalent and that the cardiovascular component may mark a more advanced or clinically consequential stage of systemic injury in patients with AF.
These observations also align with emerging data across ethnic groups. A large multicenter Taiwanese cohort of 17 378 anticoagulated AF patients showed that increasing CKM‑domain burden was associated with progressively higher risk of ischemic, bleeding, heart failure, renal, and mortality outcomes, and with a greater number of years of life lost, supporting the broader prognostic relevance of CKM complexity in AF (Figure 1).5 Still, the distinct strength of the study by Mantovani et al3 lies not simply in confirming a prognostic gradient, but in linking that gradient to atrial structure.
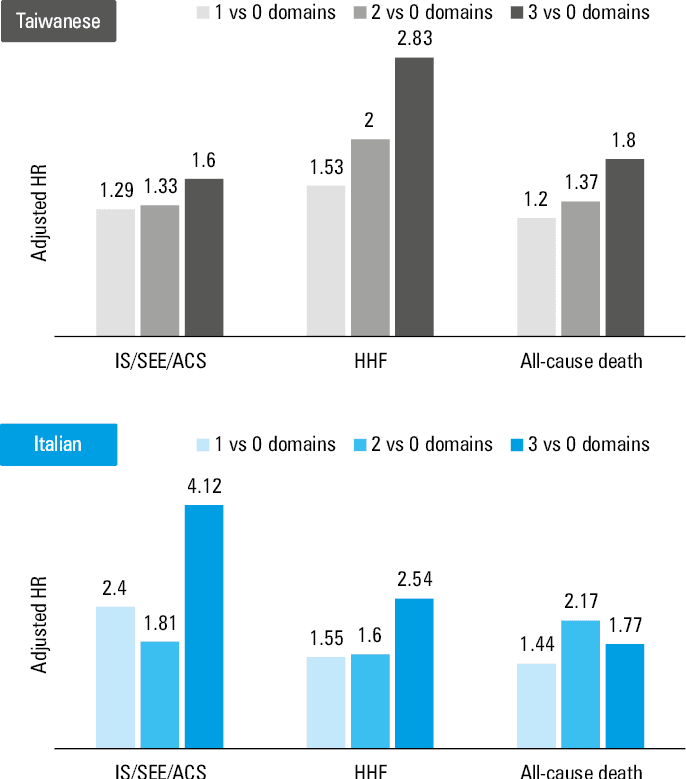
Abbreviations: ACS, acute coronary syndrome; HHF, hospitalization for heart failure; HR, hazard ratio; IS, ischemic stroke; SEE, systemic embolic event
One of the most valuable contributions of this study is its demonstration that CKM multimorbidity is associated with left atrial (LA) remodeling. In the echocardiographic subset, the proportion of patients with LA dilation progressively increased in parallel with higher CKM burden. Specifically, the prevalence of severe LA dilation increased from 24.2% up until 40% and 40.5% in patients with 2 or 3 CKM conditions, respectively.3
This structural association provides biological plausibility for the observed prognostic gradient. CKM multimorbidity likely promotes atrial remodeling through multiple converging pathways, including chronic pressure overload, vascular stiffness, metabolic inflammation, endothelial dysfunction, neurohormonal activation, and the myocardial consequences of renal impairment.6 Through these mechanisms, the LA becomes more than the chamber in which AF occurs; it becomes a target organ of CKM disease. This interpretation is also congruent with the broader CKM framework proposed by the American Heart Association, which positions CKM disease as a progressive, interconnected continuum rather than an isolated condition.1
That idea deserves emphasis. AF may not simply coexist with CKM syndrome; it may represent one of its cardiac manifestations. By connecting CKM burden with measurable atrial remodeling, Mantovani et al3 suggest that the substrate of AF is, at least in part, the cumulative structural expression of multisystem disease.
The clinical message is straightforward: CKM burden should not be regarded as background information in AF care. It appears to shape prognosis, influence atrial structure, and likely affect therapeutic response. Conventional AF frameworks remain essential, but they may not fully capture the biological complexity of patients whose risk is driven by overlapping cardiovascular, renal, and metabolic disease.
This point is reinforced by the treatment patterns observed in the study. The patients with greater CKM burden were less likely to receive antiarrhythmic drugs and had a more complex overall pharmacologic profile, reflecting both more advanced disease and the therapeutic challenges of multimorbidity.3
Accordingly, the study supports a more integrated model of AF care. This is consistent with evidence supporting structured AF care pathways, including the ABC approach and mobile health–enabled integrated care, both of which have been associated with improved outcomes in randomized and observational settings.7-9 Routine assessment of CKM burden may therefore help identify the patients who warrant closer surveillance, earlier upstream intervention, and more deliberate multidisciplinary management. The point is not that CKM assessment should replace conventional stroke and bleeding risk scores, but that it may refine and extend them by capturing a broader background of disease.
This broader framing may also help explain why early rhythm‑control strategies seem especially relevant in patients with substantial cardiovascular comorbidity. Trials and secondary analyses have shown that early rhythm control can improve cardiovascular outcomes, including in patients with a higher comorbidity burden.10,11 Mantovani et al3 did not test rhythm‑control strategy directly, but their findings reinforce the view that AF outcomes are shaped not only by the arrhythmia, but also by the systemic milieu in which it occurs.
Several limitations should temper interpretation of the results. First, this was a prospective but single‑center observational study, and causality cannot be established. Second, the definitions of CKM conditions were pragmatic and clinically usable, yet incomplete. Albuminuria was not incorporated into the kidney domain, and the metabolic domain was focused on diabetes rather than the broader spectrum of metabolic dysfunction. Obesity was also excluded from the primary CKM definition. Third, echocardiographic data were available only in a subset of patients, which may have introduced selection bias. Lastly, residual confounding cannot be totally excluded, particularly with respect to AF burden, treatment intensity, and other unmeasured determinants of risk.
Even with these caveats, Mantovani et al3 should be congratulated on having demonstrated that CKM multimorbidity in AF is common, structurally relevant, and prognostically important. Contemporary external data offer support for the same general direction of association,5 but the distinct strength of the present study lies in the integration of outcomes with LA remodeling. Future work should determine whether CKM profiling improves risk prediction beyond conventional AF scores, and whether therapies targeting CKM pathways can modify atrial remodeling and long‑term outcomes. Until then, this study serves as a timely reminder that, in many patients, the true substrate of AF is broader than rhythm alone.
- Ndumele CE, Neeland IJ, Tuttle KR, et al. A synopsis of the evidence for the science and clinical management of cardiovascular‑kidney‑metabolic (CKM) syndrome: a scientific statement from the American Heart Association. Circulation. 2023; 148: 1636‑1664. | Crossref
- Liao JN, Chan YH, Kuo L, et al. Temporal trends of prescription rates, oral anticoagulants dose, clinical outcomes, and factors associated with non‑anticoagulation in patients with incident atrial fibrillation. Eur Heart J Qual Care Clin Outcomes. 2025; 11: 300‑311. | Crossref
- Mantovani M, Vitolo M, Bonini N, et al. Impact of cardiovascular‑kidney‑metabolic conditions on clinical outcomes in patients with atrial fibrillation: results from a prospective cohort study. Pol Arch Intern Med. 2026; 136: 17255. | Crossref
- Chang HC, Chan YH, Kuo L, Chao TF. Patient care pathways and risk assessments in patients with atrial fibrillation: a comparison of Asian versus non‑Asian cohorts. Thromb Haemost. 2025; 125: 1173‑1180. | Crossref
- Chan YH, Kao YW, Cheng WH, et al. Cardiovascular‑kidney‑metabolic interplay in patients with atrial fibrillation receiving direct oral anticoagulants. Europace. 2026; 28: euag028. | Crossref
ARTICLE INFORMATION