Leadless pacemaker implantation planned with computed tomography–based 3-dimensional modeling in a 51-year man with a functional single left ventricle and pulmonary outflow obstruction

 CC BY 4.0
CC BY 4.0
Leadless pacemaker implantation planned with computed tomography–based 3-dimensional modeling in a 51-year man with a functional single left ventricle and pulmonary outflow obstruction
A 51‑year‑old patient with a congenital functional univentricular heart (single dominant left ventricle) has survived into late adulthood without definitive biventricular repair (Figure 1A–1E). Long‑term survival in unoperated single‑ventricle physiology is uncommon; however, selected patients with a “balanced” circulation—frequently involving left ventricular morphology and pulmonary outflow obstruction—may reach late decades of life with preserved functional status.1
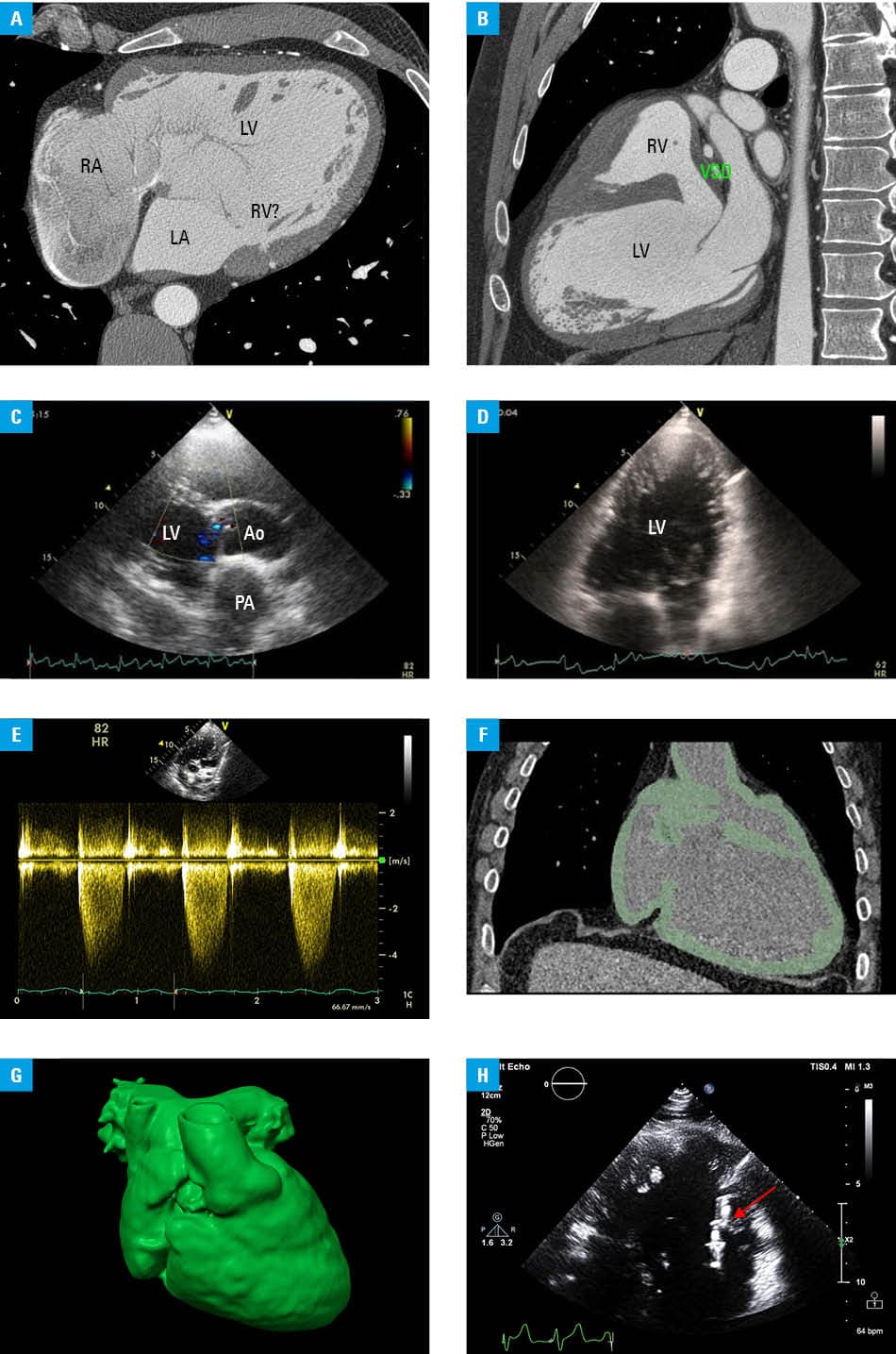
Abbreviations: Ao, aorta; LA, left atrium; LV, left ventricle; PA, pulmonary artery; RA, right atrium; RV, right ventricle; VSD, ventricular septal defect
The patient presented with acquired third‑degree atrioventricular block requiring permanent pacing. In adult congenital heart disease, conventional transvenous or epicardial pacing is often limited by complex anatomy and vascular access constraints. Therefore, leadless ventricular pacing was considered the most appropriate option in this case.2,3
Due to the highly atypical intracardiac anatomy, standard procedural planning tools, such as the Leadless Pacemaker Implantation Score, could not be applied. A patient‑specific 3‑dimensional (3D) model based on cardiac computed tomography (CT) imaging was therefore created to support procedural planning (Figure 1F and 1G).
Importantly, beyond technical preparation, the model enabled identification of a feasible implantation zone within the dominant left ventricle, most likely along the mid‑to‑apical septal region, where sufficient myocardial thickness and stability for device fixation could be anticipated, while minimizing the risk of interference with abnormal inflow structures and avoiding regions of turbulent flow related to the ventricular septal defect.4,5
Based on this planning, the procedure was performed via the femoral venous access, and a leadless pacemaker was successfully implanted. The final device position corresponded well with the preprocedural simulation; it was located in the trabeculated septal portion of the dominant ventricle, providing stable fixation and appropriate electrical parameters.
Immediate postprocedural assessment demonstrated stable device positioning within the trabeculated septal region of the dominant ventricle, with satisfactory electrical parameters and no procedure‑related complications (Figure 1H). At the time of implantation, pacing threshold was 0.75 V at 0.4 ms, R‑wave sensing amplitude was 12 mV, and pacing impedance was 780 Ω.
On the first postimplantation day, device interrogation confirmed stable electrical performance, with preserved pacing threshold of 0.75 V at 0.4 ms, improved sensing amplitude exceeding 18 mV, and impedance of 560 Ω. No device‑related abnormalities or alerts were detected during interrogation.
The device was programmed in the VVIR mode with rate‑responsive pacing enabled, a lower rate limit of 60 bpm, and a maximum sensor rate of 130 bpm. Short‑term follow‑up demonstrated effective ventricular pacing without evidence of device dislodgement, thromboembolic complications, worsening heart failure symptoms, or an increase in pacing threshold. To our knowledge, reports describing CT‑based 3D planning of leadless pacing in long‑term survivors with functionally univentricular physiology remain extremely limited.
- Poterucha JT, Anavekar NS, Egbe AC, et al. Survival and outcomes of patients with unoperated single ventricle. Heart. 2016; 102: 216‑222. | Crossref
- Glikson M, Nielsen JC, Kronborg MB, et al; ESC Scientific Document Group. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy: developed by the Task Force on cardiac pacing and cardiac resynchronization therapy of the European Society of Cardiology (ESC) with the special contribution of the European Heart Rhythm Association (EHRA). Eur Heart J. 2021; 42: 3427‑3520. | Crossref
- Bassareo PP, Walsh KP. Micra pacemaker in adult congenital heart disease patients: a case series. J Cardiovasc Electrophysiol. 2022; 33: 2335‑2343. | Crossref
- Olejník P, Nosal M, Havran T, et al. Utilisation of three‑dimensional printed heart models for operative planning of complex congenital heart defects. Kardiol Pol. 2017; 75: 495‑501. | Crossref
- Martinez‑Sande JL, Gonzalez‑Melchor L, Garcia‑Seara J, et al. Leadless pacemaker implantation with hybrid image mapping technique in a congenital heart disease case. HeartRhythm Case Rep. 2021; 7: 797‑800. | Crossref
ARTICLE INFORMATION