Current management of Clostridioides (Clostridium) difficile infection in adults: a summary of recommendations from the 2017 IDSA/SHEA clinical practice guideline
Key words: Clostridioides difficile, Clostridium difficile, guidelines, management



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Current management of Clostridioides (Clostridium) difficile infection in adults: a summary of recommendations from the 2017 IDSA/SHEA clinical practice guideline
Clostridioides (formerly Clostridium) difficile infection (CDI) is the most common cause of health care–associated infectious diarrhea in the developed world. The Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America clinical guidelines on CDI were updated in 2017. The update reflects a decline in the incidence of CDI caused by ribotype 027 and an increased incidence of community‑associated CDI, current challenges in CDI diagnosis, the importance of antibiotic stewardship and contact and isolation precautions in infection prevention and control, and many significant changes in CDI management. This review summarizes and examines these new guidelines, how they compare to other recommendations, and more recent data on CDI management.
Introduction
Since its initial description as the cause of pseudomembranous colitis in 1978,1 Clostridioides (formerly Clostridium) difficile has grown in importance to become the most common cause of infectious nosocomial diarrhea in the developed world. Clostridioides difficile infection (CDI) is still associated with significant costs, morbidity, and mortality. Since the release of the 2010 Infectious Disease Society of America (IDSA)/Society for Healthcare Epidemiology of America (SHEA) guidelines on CDI,2 there have been advances and updates in epidemiology, diagnostics, prevention, and treatment of CDI, which are reflected in the recently published 2017 update.3 This review summarizes the data used in the updated guidelines and compares them to CDI guidelines published by other medical associations.
Epidemiology
Clostridioides difficile is a Gram‑positive, spore‑forming anaerobe transmitted via the fecal–oral route. Nontoxigenic and toxigenic forms exist, with the latter producing toxins A and B, which are necessary for CDI.3 Clostridioides difficile is a ubiquitous organism, and most people are presumably colonized with it at some point in their lives, if not multiple times. Most of the time, it results in transient, asymptomatic colonization. When C. difficile causes a disease, as in CDI, it can range from mild self‑limited diarrhea to fulminant colitis with shock. New cases can be defined by location and timing of symptom onset to aid in epidemiologic studies and prevention efforts (Table 1).3
Epidemiologic type | Definition |
Health care facility–onset CDI | Onset >3 days after admission to a health care facility (on or after day 4) |
Community‑onset/Health care facility–associated CDI | Onset in the community or ≤3 days of admission to a health care facility and within 12 weeks of discharge from a health care facility |
Health care–associated CDI | Term used when grouping health care facility–onset and community‑onset/health care facility–associated CDI cases together, as opposed to community‑associated CDI |
Community‑associated | CDI onset in the community or ≤3 days of admission to a health care facility but without an inpatient stay in the prior 12 weeks |
After the year 2000, CDI‑related morbidity, mortality, and costs have increased dramatically. Before 2000, the mortality rate attributable to CDI was less than 1.5%, while after 2000, this increased to between 4.5% and 5.7% during endemic periods and up to 16.7% during epidemic periods.4 There were also dramatic increases in the incidence of CDI. According to the Centers for Disease Control and Prevention in the United States, close to 500000 cases were diagnosed in 2011, with about 29000 associated deaths and an estimated $4.8 billion in unnecessary inpatient costs.5,6 These changes in CDI epidemiology coincided with the identification of a new predominant strain known as 027/NAP1/BI (the name varies based on the type of molecular typing technique, referred to as ribotype 027 from here onwards). This strain is highly fluoroquinolone resistant, is associated with more severe CDI, and is more likely to cause recurrent CDI.7,8 Fortunately, since the 2010 IDSA/SHEA guidelines were released, this more virulent strain has become less prevalent around the world, accounting for less than 10% of cases in England (from >50% in 2007) and less than 20% of nosocomial cases in the United States (from 31% in 2011).9,10 However, the prevalence of this strain in Eastern Europe was found to be higher than in other parts of Europe.11
Patients with health care–onset CDI most often acquire C. difficile after admission to a facility.12 In the health care setting, although C. difficile is approximately 16 times more likely to be transmitted from a patient with CDI than an asymptomatic carrier, there are typically 10 times more asymptomatic C. difficile carriers than patients with CDI.13 It has been estimated that transmission from as few as 1% of asymptomatic carriers can account for as many as 50% of new hospital‑onset CDI cases.14 Carriage duration before clearance is unclear but may be up to several months, while patients who progress to CDI appear to develop disease at a median of less than 7 days after acquisition.15-17 Risk factors for progression to CDI include antibiotic exposures and markers of poor host immunity, including older age, hospitalization duration, and severity of an underlying illness.3,18
In addition to the increased incidence of health care–associated CDI cases since 2000, studies have demonstrated a similar trend in the incidence of community‑associated CDI cases. The 027 strain was the most common cause of health care–associated and community‑associated CDI in the United States in 2011. Similar to the trends mentioned above for health care–associated CDI, the proportion of community‑associated CDI cases due to the 027 strain has been declining since 2011, from 19% to 8%. Moreover, the 027 strain is no longer the most common causative strain of community‑associated CDI in the United States.10 Although patients with community‑associated CDI are typically younger and healthier than those with health care–associated CDI and are less likely to have an identified preceding antibiotic exposure, antibiotic exposures remain the most common identifiable risk factor. In fact, patients with community‑associated CDI tend to be older and have more health care exposures than people in the community without CDI.19,20
Diagnosis
CDI is a clinical diagnosis based on the patient’s symptoms and risk factors. Testing for C. difficile or toxin production should be targeted at higher‑risk patients who have clinically significant diarrhea that is otherwise unexplained. Various definitions of diarrhea have been used over the years, and none have been validated.3,18,21 More important than the number of diarrhea bowel movements within a specified time frame is whether the diarrhea is out of proportion from what might be expected, persistence of diarrhea, and if other concerning signs or symptoms such as abdominal pain or leukocytosis are present. Monitoring for these symptoms is especially important among people with recent antibiotic exposures. If, based on the patient’s signs and symptoms, the pretest probability for CDI is low, then monitoring of the patient is appropriate. If the pretest probability for CDI is moderate to high, then stool should be collected for testing.3,22
Laboratory evidence for CDI involves detection of C. difficile toxin or a toxigenic strain of C. difficile from stool (Table 2). Toxin detection methods include enzyme immunoassays (EIAs) for toxins A and B and cell culture cytotoxicity assay (CCNA), which is considered the gold standard for detecting toxin. Toxin‑based EIAs have fast turnaround but historically have had variable performance with moderate specificity and lower sensitivity. Of note, some older EIAs only detect toxin A, which may miss up to 20% of CDI cases caused by toxigenic C. difficile that produce only toxin B. Therefore, in general such assays should be avoided.3 Compared with older EIAs, modern toxin‑based assays that detect both toxins A and B have improved performance and generally have very good positive and negative predictive values.2,23 CCNAs involve applying a filtered stool sample to a monolayered cell culture and monitoring for a cytopathic effect after at least 24 hours of incubation. Although historically CCNAs have had higher sensitivity and specificity than toxin EIAs, they are slower, more labor intensive, nonstandardized, and operator dependent.3,23 It is important to emphasize again that CDI is a clinical diagnosis because patients may be asymptomatic carriers who have detectable toxin but without disease.
Test | PPV | NPV | Substance detected |
Toxigenic culture | Low | High | C. difficile spores or cells |
Nucleic acid amplification test | Low | High | C. difficile toxin genes |
Glutamate dehydrogenase | Low | High | C. difficile conserved common antigen |
Cell culture cytotoxicity neutralization assay | High | Moderate | Free toxin |
Toxin A and B enzyme immunoassay | Moderate | Moderate | Free toxin |
Clostridioides difficile organism detection methods include EIAs for glutamate dehydrogenase (GDH), nucleic acid amplification tests (NAATs) (eg, polymerase chain reaction), and toxigenic bacterial culture (TC). All of these assays test for the presence of the bacteria but do not detect the free toxins that cause CDI. GDH EIAs detect the GDH antigen produced by all C. difficile strains (both toxigenic and nontoxigenic). GDH EIAs overall have high sensitivity but lower specificity for CDI as they cannot distinguish toxigenic from nontoxigenic strains and need to be combined with a toxin‑based test.3,23 NAATs identify the presence of toxigenic C. difficile by detecting toxin genes. Because NAATs detect genes but not the free toxin necessary for CDI, they have a lower positive predictive value for CDI than toxin‑based assays. However, NAATs overall have high sensitivity and negative predictive value for CDI.3,23 Unlike the faster turnaround from EIAs and NAATs, TC involves incubation of stool samples on selective agar for several days before organism identification. Like GDH assays, TC needs to be combined with a toxin‑detection step to confirm toxin production. When done properly, TC is the gold standard for detecting toxigenic C. difficile organisms in stool.3,23
Recommendations for a single optimal laboratory test are lacking due to limitations in the current literature, such as nonstandardized reference standards, underpowered design, and unclear prevalence and definitions of disease.3,23 These are important considerations especially because clinical definitions and comparisons between different reference standards can substantially impact assay interpretation, test relevance, and diagnostic accuracy and can have significant epidemiologic, clinical, and financial consequences for hospitals, patients, and physicians.22,24-26
The 2017 IDSA/SHEA guidelines address C. difficile diagnostics based on pretest probability for CDI in the patient population being tested.3 The NAAT is not recommended as a standalone test when criteria for patient testing are not clear or if other causes of diarrhea may be present, because of data demonstrating that patients with C. difficile detected in stool by the NAAT but negative for C. difficile toxin have similar rates of adverse events, recovery, recurrence, mortality, and duration of symptoms as patients with stool negative by both NAAT and toxin assay.24-27 In the case of undifferentiated samples of stool submitted to a laboratory for CDI diagnostics, the 2017 guidelines recommend using a stool toxin test (higher specificity and positive predictive value) as part of a multistep algorithm with an initial screening test that has high sensitivity and negative predictive value (GDH or NAAT) over NAAT alone. If the highly sensitive screen is negative, CDI is essentially ruled out. Stools positive both by the screening and toxin assays should be interpreted as consistent with the presence of CDI. If the screen is positive and toxin test is negative, it is consistent with a patient colonized with C. difficile, and the patient is unlikely to have CDI. However, in a patient population with higher pretest probability for CDI (ie, pre‑agreed criteria for likely symptomatic CDI stool samples), NAAT as a standalone diagnostic test or toxin assay as part of a multistep algorithm can be used. Due to the aforementioned paucity of high‑quality studies, these recommendations remain weak in strength. There are insufficient data for any recommendation on other biomarkers for infection, such as fecal leukocytes, lactoferrin, or calprotectin.3
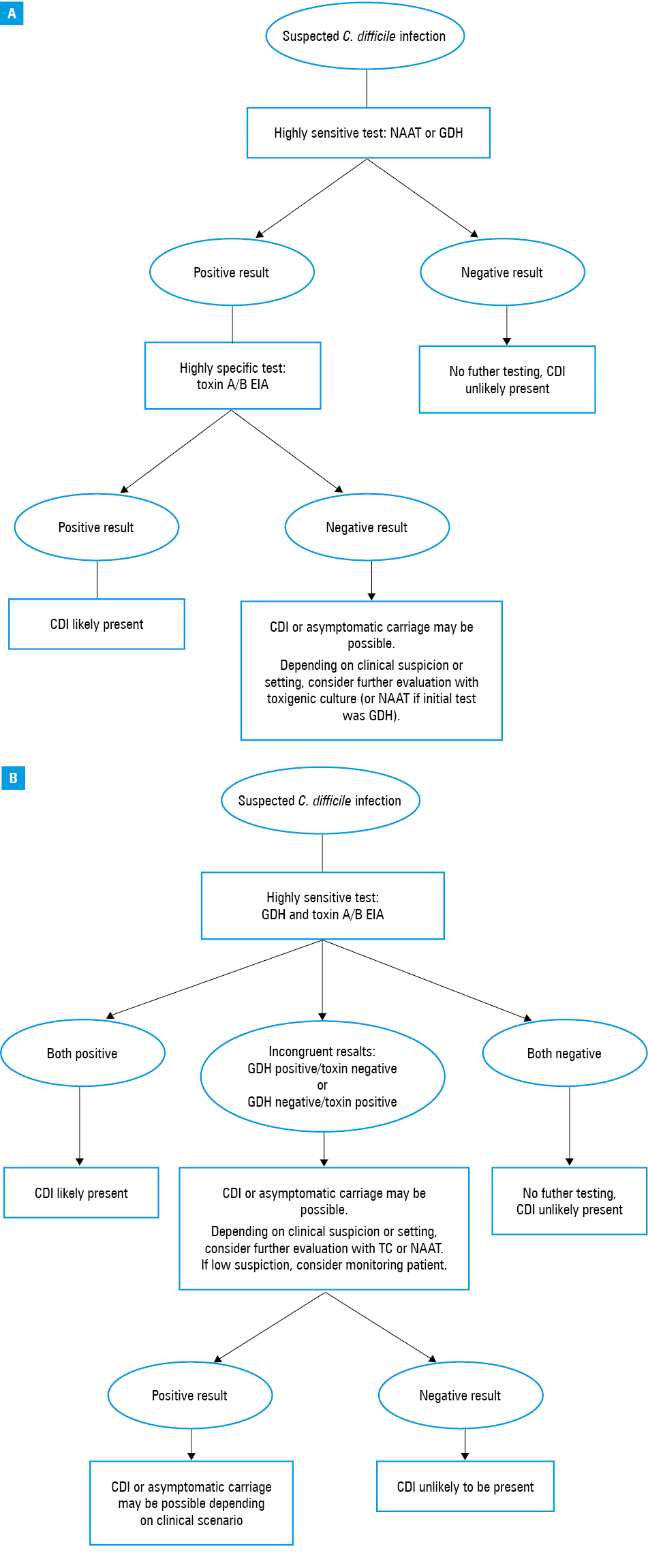
The latest IDSA/SHEA guidelines on diagnostics also update and supplement other recent recommendations. The 2013 American College of Gastroenterology (ACG) guidelines agree that only diarrheal samples from appropriate patients should be tested but recommends NAATs over toxin‑based EIAs unless as part of a multistep protocol with GDH EIAs.18 However, the ACG guidelines fail to comment on the low positive predictive value of NAATs when used alone. The 2016 European Society of Clinical Microbiology and Infectious Diseases (ESCMID) update for C. difficile diagnosis suggests that all unformed stool samples from appropriate patients received in laboratory should be tested to increase yield, and, due to the limited positive predictive value and negative predictive value for any single test, now recommends against any single‑step testing in preference for a 2‑step algorithm starting with a highly sensitive test (NAAT or GDH EIA) followed by a more specific test (toxin EIA) or simultaneous GDH and toxin EIA (Figure 1Aand 1b).23 Notably, in cases that are NAAT/GDH positive but toxin negative, the ESCMID guidelines suggest further consideration of other causes of symptoms before treatment. These cases may represent patients who have toxin levels below the detection limit, asymptomatic carriage of toxigenic C. difficile, or non–toxin‑producing C. difficile (if GDH positive and toxin negative). Further testing is suggested in situations when clinical suspicion for CDI remains high.23
All previously mentioned society guidelines advocate avoiding testing asymptomatic patients (unless for epidemiologic studies), automatic repeat testing for the same diarrheal episode, and testing for cure.3,18,23 Automatic repeat testing results in a significant drop in positive predictive value.3,28 Recurrence commonly occurs and should be retested like an initial episode, though ideally with toxin‑based tests, given the possible persistence of toxigenic strains after treatment.3,29
Infection prevention and control
Strategies for CDI prevention and control largely fall under methods to prevent transmission and those that decrease the risk of CDI if transmission or acquisition occurs. Transmission prevention encompasses early detection and environmental controls such as hand hygiene, contact precautions and isolation, and environmental cleaning. Decreasing the risk of developing CDI is currently accomplished through antibiotic stewardship.
Recommendations for early detection and environmental controls in the 2017 IDSA/SHEA update remain mostly consistent with those of the 2010 IDSA/SHEA and 2018 ESCMID guidelines.2,3,30 Patients who are suspected of or have CDI should be placed into contact precautions and isolated in private rooms with separate toileting facilities if possible. When it is not feasible to do this, it is reasonable to cohort patients with CDI together. These patients should also have single‑use or dedicated equipment to themselves.31-33 Isolation measures should stay in place for at least 48 hours after diarrhea resolves.3,34 During outbreaks, contact precautions can be extended until discharge. Providers should wear gowns and gloves and perform adequate hand hygiene before and after contact with CDI patients. Gowns and gloves must be worn for all encounters, even if direct contact with the patient is not expected, because the area surrounding the patient can be contaminated with C. difficile spores.3
One area of controversy is the preferred method of hand hygiene after caring for a patient with CDI. Alcohol‑based hand rubs (ABHR) do not kill or remove C. difficile spores.35 Although soap and water is superior to ABHR in removing C. difficile spores from contaminated hands,36 generally it may not be as effective as wearing gloves, which prevent initial soiling and significantly decrease overall spore burden.33,34 This may be why most studies have not found reductions in the incidence of CDI when soap and water is the preferred method of hand hygiene. As such, the 2017 IDSA/SHEA guidelines recommend either ABHR or soap and water for hand hygiene in endemic settings after caring for a patient with CDI.3
Another area of controversy in C. difficile prevention and control is whether and how often sporicidal agents should be used to clean the environment. The 2017 IDSA/SHEA guidelines recommend daily cleaning with sporicidal agents (eg, sodium hypochlorite) in outbreaks, hyperendemic settings, and repeated CDI cases in the same room.3 On the other hand, the 2018 ESCMID prevention guidelines suggest daily and terminal disinfection with sporicidal agents in both endemic and outbreak settings, though with a lower strength of recommendation for endemic settings.30 Standard hospital disinfectants, such as quaternary ammonium cleaning agents, do not kill C. difficile spores. Several studies have found reductions in the incidence of CDI when a sporicidal agent was used to clean the environment in an outbreak setting.37-39 Of note, since the 2017 IDSA/SHEA guidelines were drafted, there have been 2 cluster randomized trials that have failed to demonstrate reductions in CDI incidence when additional methods on top of sodium hypochlorite (which was already used at the study hospitals) were used to clean the environment. In one study, cleaning effectiveness was monitored, and feedback was provided if surfaces were not being adequately cleaned.40 The other study used an ultraviolet device for terminal discharge cleaning in addition to the standard sodium hypochlorite.41 Although both studies demonstrated a reduction in C. difficile recovery from environmental surfaces with the enhanced cleaning method being studied, neither found a reduction in CDI incidence. This is likely because most studies have demonstrated or suggested that persistent environmental contamination after discharge contributes to only 2% to 10% of new CDI cases in nonoutbreak settings.14,15 Based on these recent trials, the frequency of using a sporicidal agent should be individualized depending on the unit and institution. Because of shared common facilities and lack of physical barriers between patients, daily sporicidal cleaning may be more important in multipatient wards than in facilities where patients with CDI are able to be housed in private rooms. Ultimately, it is imperative that adequate cleaning takes place to minimize preventable CDI, but “enhanced” efforts in addition to this may not further reduce CDI incidence.
As asymptomatic carriers represent a reservoir for potential C. difficile transmission and acquisition, active surveillance and screening for carriers has been proposed to prevent and reduce transmission.15,42 The greatest evidence for active surveillance for asymptomatic C. difficile carriage comes from a recent study in Quebec, Canada. A single hospital there screened for asymptomatic carriage on admission, and C. difficile carriers were placed into modified contact precautions. There was a 62% drop in the incidence of hospital‑onset CDI (6.9 to 3 CDI cases per 10000 patient‑days) at the study hospital but no changes in the incidence at other hospitals in Quebec.43 However, this study has several important limitations including a single‑center, quasi‑experimental design and the presence of potential confounders that could contribute to reductions in CDI incidence, such as improvements in hand hygiene behaviors observed during the study period and lack of data on individual antibiotic prescribing.44 Notably, the same authors in a more recent study did not find isolation of asymptomatic carriers to be associated with shorter durations of CDI outbreaks.45 More studies are needed before routine implementation is considered. The 2013 ACG, 2018 ESCMID, and 2017 IDSA/SHEA guidelines either do not recommend or note insufficient data to recommend screening for asymptomatic carriers, given the lack of supportive data, cost and person‑time needed to screen patients, and the risk for other unintended consequences, such as overtreatment for diarrhea of unclear etiology in carriers.3,18,30
Minimizing the number, frequency, and duration of unnecessary antibiotic exposures may be the most effective way to decrease the risk of CDI.46 Antibiotic stewardship programs help guide and improve antibiotic prescribing through a variety of methods such as education, audit and feedback, and antibiotic‑use restrictions. Studies on antibiotic stewardship have demonstrated that improved antibiotic utilization leads to a 33% to more than 90% reduction in CDI.3 Antibiotic stewardship has been implicated as the primary reason behind a decrease of approximately 80% in CDI rates in England since 2006.47,48 A targeted reduction of specific antimicrobials based on C. difficile resistance patterns and local antibiograms may hasten recovery during epidemics.3,47 Antibiotic stewardship not only improves resource utilization and patient outcomes but also decreases the risk of CDI, the emergence of antibiotic resistance, and other antimicrobial‑related adverse events.49
Recommendations for probiotics for primary prevention of CDI remain inconclusive, with lack of high‑equality evidence to make a recommendation in the 2017 IDSA/SHEA guidelines. Most studies are small and lack standardization across illness definitions and probiotic preparations. Several meta‑analyses have reported probiotic benefit but utilized the same cohort of studies that have CDI incidence rates up to 20 times the rates in typical populations (about 2%–3% in elderly patients who are hospitalized and are on antibiotics), which may bias towards probiotic benefit.3,4,50-52 Some of the larger trials with CDI rates similar to typical rates have not found a significant benefit for probiotics. Given reports of infections related to organisms such as Saccharomyces and Lactobacilli species involved in probiotic use and mixed data,53-55 the net benefit for probiotics in CDI primary prevention remains unclear.
Treatment
For all cases of CDI, the 2017 IDSA/SHEA, 2014 ESCMID, and 2013 ACG guidelines recommend discontinuing any contributing antibiotics as soon as possible.3,18,21 Studies demonstrate that continued use of antimicrobials is associated with prolonged duration of diarrhea and increased risk for recurrence.56,57 For nonsevere CDI, the current ESCMID guidelines suggest discontinuing offending antimicrobials when able and waiting 48 hours before starting any empiric therapy as many times CDI is self‑limited. Due to concerns for adverse events if treatment is withheld, this is not recommended in the ACG or IDSA/SHEA guidelines.3,18,21 It has traditionally been advised to avoid antimotility agents when patients have CDI, but these can be safely used if the patient does not have ileus and is receiving oral vancomycin or fidaxomicin. Testing for cure should not be done as it is not predictive of treatment failure or risk of recurrence.29,58 Although the 2017 IDSA/SHEA guidelines continue to categorize treatment based on CDI severity, CDI severity stratification remains a challenge as there are no randomized control trials that have prospectively validated specific severity measures. Current recommendations for measures of CDI severity are based largely on expert opinion and retrospective or observational studies.
For an initial episode of CDI, oral vancomycin and fidaxomicin are now recommended in the 2017 IDSA/SHEA guidelines as the main first‑line treatment options regardless of CDI severity (unless fulminant). Metronidazole is no longer considered a first‑line therapy for nonsevere CDI and should be considered for nonsevere CDI only if neither of the first 2 options are readily available (Table 3). The recommendation in the 2010 IDSA/SHEA guidelines to stratify treatment by CDI severity was based primarily on a single‑center trial published in 2007. This study found oral vancomycin to be superior to metronidazole for resolution of severe CDI, but it did not find a significant difference between metronidazole and oral vancomycin for resolution of nonsevere CDI (though there was a trend towards better outcomes with vancomycin).59 Notably, this was the first double‑blind randomized trial of CDI treatment. Lack of blinding, small sample sizes, and increases in severe CDI after the year 2000 may explain why studies prior to 2000 found no differences in treatment outcomes between metronidazole and oral vancomycin.29,60 The 2017 updates in treatment recommendations were based on what are the only multicenter double‑blind, adequately powered randomized controlled trials comparing metronidazole to oral vancomycin published to date. These studies demonstrated vancomycin superiority to metronidazole in overall treatment response regardless of CDI severity.61 Additional supportive data that oral vancomycin is superior to metronidazole include a recent meta‑analysis and a propensity‑matched retrospective cohort study that demonstrated improved survival for oral vancomycin compared with metronidazole.62,63 Considering metronidazole’s unfavorable pharmacokinetics and the changing virulence and epidemiologic patterns of C. difficile over the last 20 years, it is not surprising that metronidazole has had poorer efficacy in these more recent studies and should not be used as a first‑line agent in CDI.
Classification | Criteria | Treatment recommendations |
a Multiply quantity in mg/dl by 88.42 to convert serum creatinine into µmol/l units.
b Typical dosing for per rectum vancomycin is a retention enema of 500 mg in 100 ml saline dosed every 6 hours.
c Sample pulsed‑tapered regimen is 125 mg 4 times daily for 10 to 14 days, 2 times daily for a week, once daily for a week, and then every 2 to 3 days for 2 to 8 weeks. | ||
First episode, nonsevere | Leukocyte count ≤15000 cells/ml and serum creatinine <1.5 mg/dla | Oral vancomycin, 125 mg 4 times daily, for 10 days or oral fidaxomicin, 200 mg twice daily, for 10 days. If neither above are available, oral metronidazole, 500 mg 3 times daily, for 10 days. |
First episode, severe | Leukocyte count >15000 cells/ml or serum creatinine ≥1.5 mg/dl | Oral vancomycin, 125 mg 4 times daily, for 10 days or oral fidaxomicin, 200 mg twice daily, for 10 days |
Fulminant (previously called severe, complicated) | Any of the above and hypotension, shock, ileus, or toxic megacolon. Consider also other factors such as elevated lactate (≥5 mmol/l) or significant leukocytosis (≥25000 cells/ml). | Consider early surgical consultation and vancomycin, 500 mg 4 times daily, orally or by nasogastric tube. If gut motility limited, give vancomycin per rectumb and intravenous metronidazole, 500 mg every 8 hours. |
First recurrence | Recurrent symptoms within 8 weeks after completing therapy | If initially treated with metronidazole, use oral vancomycin, 125 mg 4 times daily, for 10 days.
If initially treated with vancomycin, use a prolonged pulsed‑tapered vancomycinc or fidaxomicin, 200 mg twice daily, for 10 days |
Second or subsequent recurrence | Pulsed‑tapered vancomycin regimenc, or oral fidaxomicin, 200 mg twice daily, for 10 days, or oral vancomycin, 125 mg 4 times daily, for 10 days and then oral rifaximin, 400 mg 3 times daily, for 20 days, or fecal microbiota transplant | |
Although oral vancomycin and fidaxomicin are both first‑line agents for nonsevere and severe CDI in the 2017 IDSA/SHEA guidelines, the 2014 ESCMID guidelines reserve vancomycin and fidaxomicin treatment for CDI cases of high recurrence risk and severe CDI.3,21 The 2017 IDSA/SHEA guidelines do not include recurrence risk as part of its CDI treatment selection stratification for an initial episode of CDI.
Data to support use of fidaxomicin as a first‑line agent for an initial CDI episode or first recurrence are based on 2 large multinational double‑blind randomized controlled studies that demonstrated similar levels of treatment success for fidaxomicin as vancomycin but overall significantly better sustained treatment response (ie, less CDI recurrence) with fidaxomicin.64-66 Patients experiencing an initial episode of CDI or first recurrence were eligible for these trials, but patients with more than 1 recurrence were excluded. A trend towards improved sustained clinical response for the 027 strain was demonstrated in one of the trials but not in the other. More recently, the EXTEND trial comparing extended fidaxomicin dosing with oral vancomycin found a significantly better sustained clinical response for fidaxomicin with the 027 strain.67 A meta‑analysis also demonstrated a trend towards improved survival within 12 days for fidaxomicin compared with vancomycin.68 Some evidence points towards less fecal microbiota disruption as a major cause of decreased recurrence.69
For fulminant CDI (formerly classified as severe, complicated CDI), the 2017 IDSA/SHEA guidelines recommend high‑dose oral vancomycin (500 mg 4 times/d) with intravenous metronidazole and early consideration of surgical intervention.70-73 Vancomycin may be further given per rectum if ileus is present. No evidence specifically addresses high‑dose versus standard‑dose vancomycin in fulminant infection. Based on luminal levels of vancomycin at the 125‑mg dose, one would not expect 500 mg to be more efficacious.58,74,75 Rather, the rationale for administering higher doses of vancomycin is an effort to achieve therapeutic levels in the colon as quickly as possible, recognizing that gut transit time in these critically ill patients may be delayed even in the absence of an overt ileus. In cases of severe colitis, monitoring of serum vancomycin levels may be appropriate in patients with impaired renal function given reports of elevated serum levels with higher doses leading to adverse outcomes.76 Concerns over impaired gut function is why coadministration of intravenous metronidazole is also recommended. Because metronidazole is inferior to oral vancomycin, it should not be administered as monotherapy. Notably, as current studies for fidaxomicin excluded fulminant CDI cases, no data exist to guide usage of fidaxomicin in life‑threatening CDI. When compared to the IDSA/SHEA guidelines, the ESCMID recommends intravenous metronidazole as adjunctive therapy to nasogastric tube or enema‑administered vancomycin only in cases when oral drug administration is not possible.21 Both the ESCMID and IDSA/SHEA suggest an early surgical consultation, especially with significant leukocytosis (≥25 000 cells/ml) or rising lactate levels (≥5 mmol/l), given higher associated mortality.72 Newer surgical interventions include diverting loop ileostomy and colonic lavage with concurrent antibiotics, which show good outcomes when compared with colectomy.73
CDI recurrence arises when symptoms improve or resolve on therapy with reemergence of symptoms within 8 weeks of therapy discontinuation.3,18,21 For the first recurrence when previously treated with metronidazole, the 2017 IDSA/SHEA guidelines recommend patients should be treated with a standard course of oral vancomycin or fidaxomicin. If initially treated with oral vancomycin or fidaxomicin, patients should be treated with a pulsed‑tapered vancomycin regimen or fidaxomicin. Patients with an initial CDI episode or the first recurrence were enrolled in phase 3 fidaxomicin trials, and there were no differences in a decreased risk for recurrence with fidaxomicin whether the patient was experiencing an initial episode or the first recurrence.66,77 For the second and subsequent recurrences, multiple regimens exist, including pulse‑tapered vancomycin, vancomycin followed by rifaximin, and fidaxomicin, but there is limited evidence on their efficacy for multiply recurrent CDI.74,78,79 Metronidazole should be avoided for any recurrence due to lower efficacy and potential risk of neurologic toxicity with prolonged use.80 In cases when patients need systemic antibiotic therapy concurrently or soon after completing CDI therapy, there is limited evidence for secondary prophylaxis with oral vancomycin, and lower doses may be sufficient (eg, vancomycin, 125 mg once daily).74,76
The 2017 IDSA/SHEA guidelines also recommend fecal microbiota transplantation (FMT) for patients with multiply recurrent CDI despite at least 2 antibiotic‑based approaches to prevent recurrent CDI. When used to prevent additional episodes of recurrent CDI, FMT is typically administered after completion of a course of oral vancomycin. Case reports and case series indicate the success of a single dose of FMT to be 65% to 90%.81 Three placebo‑controlled trials of microbial therapy, including FMT, for CDI had an overall relative reduction in recurrence versus placebo of about 50%.82-84 There are several guidelines for donor screening for FMT. At a minimum, donors should be screened for HIV, hepatitis B virus, hepatitis C virus, syphilis, and bacterial and parasitic pathogens in stool.85-89 Potential long‑term sequelae of FMT remains an area of active investigation as our understanding of how the microbiome impacts our metabolic, immune, and cognitive functions continues to expand.
Bezlotoxumab is a human monoclonal antibody against C. difficile toxin B. It was approved by the United States Food and Drug Administration in October 2016 for prevention of recurrent CDI, which was too late for inclusion in the 2017 IDSA/SHEA guidelines. Two multicenter randomized controlled trials demonstrated that the addition of bezlotoxumab to standard‑of‑care CDI antibiotic therapy significantly reduced recurrent CDI compared with placebo. Bezlotoxumab had no impact on treatment success of the qualifying CDI episode. These findings were not affected by an initial CDI therapy choice (eg, metronidazole, vancomycin, or fidaxomicin) in a subgroup analysis.90 A prespecified post hoc analysis of patients at high risk for recurrent CDI (age ≥65 years, prior CDI, immunocompromised, severe CDI based on Zar score ≥2, and infection with virulent ribotypes 027, 078, or 244) demonstrated superiority of bezlotoxumab in preventing recurrent CDI compared with placebo if at least one of these was present, but no benefit to bezlotoxumab if none of these were present.59,91 Ultimately, these factors may be helpful in stratifying patients at risk for recurrence and who may benefit from bezlotoxumab.
Conclusions
CDI continues to be a significant clinical challenge and remains one of the most significant causes of health care–associated morbidity and mortality. Although overall incidence of community‑associated CDI has increased, epidemiological trends in multiple different countries demonstrate a decreasing incidence of ribotype 027 in both community and health care settings. CDI is a clinical diagnosis and depends first on clinical judgment before any testing in order to prevent overdiagnosis and improve pretest probability and interpretability. The optimal diagnostic test or multistep algorithm remains controversial, may be institution specific, and ideally involves discussions with clinicians and the laboratory to obtain proper samples for testing. Current best practices for CDI prevention and control continue to rely on antibiotic stewardship and adherence to contact and isolation precautions. Although asymptomatic C. difficile carriers likely contribute to new cases of CDI, it is currently not recommended to screen for asymptomatic carriage. Treatment recommendations for CDI have significantly changed. Metronidazole is no longer considered a first‑line therapy. Oral vancomycin and fidaxomicin are now considered first‑line therapies for initial episodes of CDI and first recurrence. There is a growing role for fecal microbiota transplant and immunotherapies for recurrent CDI.
- Bartlett JG, Moon N, Chang TW, et al. Role of Clostridium difficile in antibiotic‑associated pseudomembranous colitis. Gastroenterology. 1978; 75: 778‑782.
- Cohen SH, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infect Control Hosp Epidemiol. 2010; 31: 431‑455. | Crossref
- McDonald LC, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin Infect Dis. 2018; 66: e1‑e48.
- Kwon JH, Olsen MA, Dubberke ER. The morbidity, mortality, and costs associated with Clostridium difficile infection. Infect Dis Clin North Am. 2015; 29: 123‑134. | Crossref
- Lessa FC, Mu Y, Bamberg WM, et al. Burden of Clostridium difficile infection in the United States. N Engl J Med. 2015; 372: 825‑834. | Crossref
ARTICLE INFORMATION