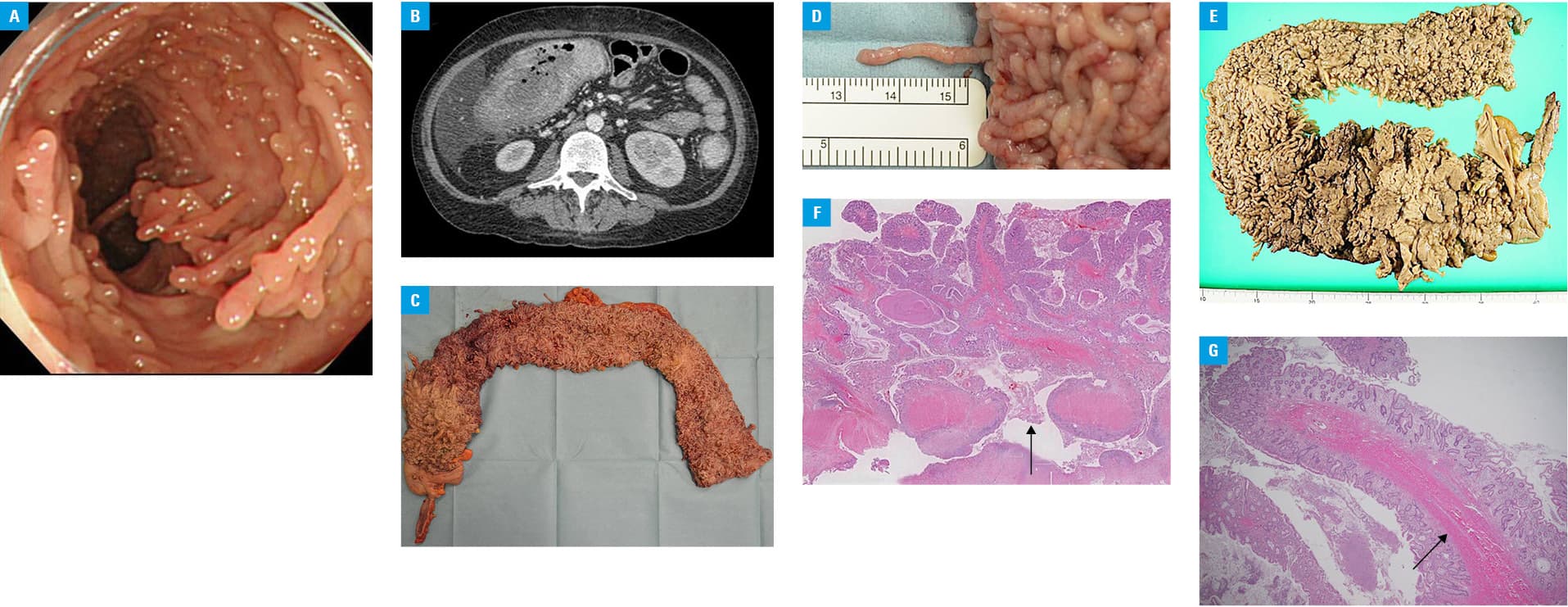
A 39‑year‑old man with a 16‑year history of ulcerative colitis presented with bloody diarrhea. He had not visited the clinic regularly, and colonoscopy at the age of 36 showed filiform polyposis of the entire colon (Figure 1A). On admission, an abdominal computed tomography (CT) scan showed a marked wall thickening of the colon (Figure 1B). Six days later, he had acute onset of severe abdominal pain. Peritoneal signs were noted, and CT revealed free air, suggesting bowel perforation. Thus, the patient underwent emergent colectomy and ileostomy. The postoperative course was uneventful. The entire surface of the resected colon was covered with numerous filiform polyps (Figure 1C–1E), and the perforation site was identified in the ascending colon (Figure 1F). The presence of the fibrovascular core (Figure 1G) confirmed the pathological diagnosis of filiform polyposis.
Postinflammatory polyps (PIPs), also known as “pseudopolyps,” are nonneoplastic lesions originating from the mucosa after repeated periods of inflammation and ulceration connected with excessive healing processes.1 They are usually associated with inflammatory bowel diseases (ulcerative colitis, Crohn disease), intestinal tuberculosis, and diverticular disease. PIPs vary in size, with different patterns of distribution and morphology, and are classified into localized multiple, giant, generalized, and filiform polyposis.2 Filiform polyposis is characterized by numerous finger‑like inflammatory polyps. These polyps form from the residual mucosal areas surrounded by ulcers, and the fecal stream may elongate these tags to create slender forms.2,3 PIPs have been associated with a 2‑fold increased risk of colorectal cancer, but they do not seem to have malignant potential in themselves. It is possible that PIPs may obscure the adequate visualization of neoplastic lesions in endoscopic surveillance or that their presence is just an evidence of previous severe inflammation leading to cancer.1,4,5 Surveillance chromoendoscopy with targeted biopsies at appropriate intervals is the key to detect neoplastic lesions earlier and determine the indications for colectomy.1,5 Surgery is required in cases of cancer, bowel obstruction, or perforation, as in this case. There is a general acceptance that if PIPs without any complications are adequately surveyed during endoscopy, no removal is considered mandatory.1
- Politis DS, Katsanos KH, Tsianos EV, et al. Pseudopolyps in inflammatory bowel diseases: Have we learned enough? World J Gastroenterol. 2017; 23: 1541‑1551.
- Maggs JR, Browning LC, Warren BF, et al. Obstructing giant post‑inflammatory polyposis in ulcerative colitis: case report and review of the literature. J Crohns Colitis. 2008; 2: 170‑180. | Crossref
- Lim YJ, Choi JH, Yang CH. What is the clinical relevance of filiform polyposis? Gut Liver. 2012; 6: 524‑526.
- Dyson JK, Rutter MD. Colorectal cancer in inflammatory bowel disease: what is the real magnitude of the risk? World J Gastroenterol. 2012; 18: 3839‑3848.
- Magro F, Gionchetti P, Eliakim R, et al. Third European evidence‑based consensus on diagnosis and management of ulcerative colitis. Part 1: definitions, diagnosis, extra‑intestinal manifestations, pregnancy, cancer surveillance, surgery, and ileo‑anal pouch disorders. J Crohns Colitis. 2017; 11: 649‑670. | Crossref
ARTICLE INFORMATION