A 34‑year‑old man was hospitalized in the Department of Tropical and Parasitic Diseases, Poznan University of Medical Sciences, Poland, due to compensated liver cirrhosis (Figure 1A) in the course of inoperable alveolar echinococcosis (AE). On admission in September 2018, we found an enlarged liver, palm‑tree sign on the skin of the abdominal cavity, and a single spider angioma on the back. Laboratory tests revealed elevated levels of γ-glutamyltransferase, alkaline phosphatase, and unconjugated bilirubin. Additionally, we found microcytic anemia, iron deficiency, low ferritin levels, a prolonged prothrombin time, and increased D‑dimer levels. On imaging, a large focal lesion (78 × 59 mm) was demonstrated, originally occupying liver segments IV and VIII (Figure 1B), with invasion of the diaphragm and right lung segments VII and VIII. The patient was classified as the P4N1M1 group1 according to the PNM (P = parasitic mass, N = involvement of neighboring organs, M = metastasis) classification and class A according to the Child–Pugh score, and he obtained 9 points in the Model for End‑Stage Liver Disease score. He was considered ineligible for surgical intervention and potential liver transplantation.
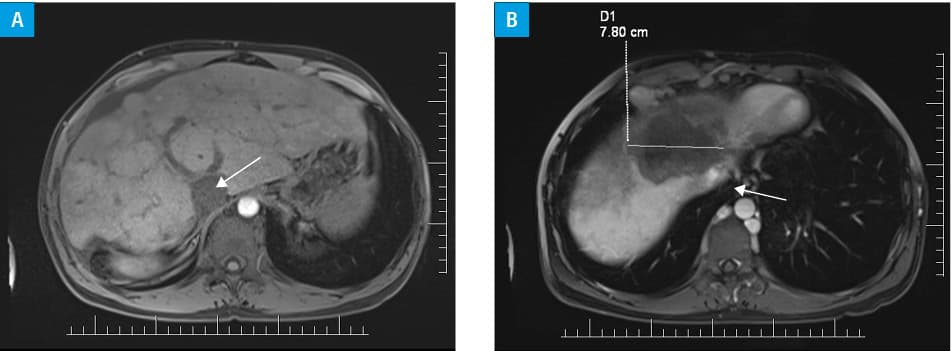
In 2011, AE was diagnosed on the basis of epidemiological data (red foxes observed in household), diagnostic imaging, and a sequential enzyme‑linked immunosorbent assay using Em2 antigen and Western blotting, which confirmed Echinococcus multilocularis infection.2 Alanine and aspartate transferase levels, bilirubin levels, and activated partial thromboplastin time were normal on admission. Abdominal ultrasonography revealed a single gallstone (4 mm in size) and a 92‑mm lesion with calcifications in the liver segment. There was no nodular remodeling of the liver, and hepatitis B and C virus infections were excluded. In 2016, computed tomography angiography revealed collateral circulation (lumbar and paraspinal veins to the azygos vein and hemiazygos vein) and inferior vena cava (IVC) subphrenic constriction. The IVC thrombosis may have formed as a result of the parasitic masses infiltrating the main venous trunks. This condition is rarely described in the course of AE. The patient was treated with albendazole since 2011 in accordance with the current World Health Organization standards, but because of the irregular drug intake, some thrombotic complications occurred.2 In addition to albendazole, he received rivaroxaban. The subsequent imaging studies (February 2018) showed a progression of liver parasitic masses and the presence of satellite foci. We also observed an uncontrasted IVC in the intrahepatic segment (Figure 1B), with persistent thrombotic features, as a result of the irregular drug intake. Acenocoumarol treatment with international normalized ratio monitoring was then implemented. In May 2018, the patient was diagnosed with grade 3 esophageal varices, ligated during gastroduodenoscopy. This was followed by an episode of bleeding from the upper gastrointestinal tract. Anticoagulation treatment was discontinued. Due to the advanced state of the parasitic process, liver cirrhosis, and thrombotic lesions of the main abdominal trunks, the prognosis for survival is poor.
The number of diagnosed cases of AE in Poland has increased significantly.3 The disorder leads to changes in the liver that are often asymptomatic for a long time, imitating the malignant disease.4 The described case indicates that cirrhosis in AE occurs not only because of the direct action of the parasite but also due to its indirect influence on the IVC, thus potentially revealing a new mechanism of liver damage.
- Kern P, Wen H, Sato N, et al. WHO classification of alveolar echinococcosis: principles and application. Parasitol Int. 2006; 55 (Suppl): S283‑S287.
- Brunetti E, Kern P, Vuitton DA, et al. Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop. 2010; 114: 1‑16. | Crossref
- Nahorski WL, Knap JP, Pawłowski ZS, et al. Human alveolar echinococcosis in Poland: 1990‑2011. PLoS Negl Trop Dis. 2013; 7: e1986.
- Vuitton DA, Zhang SL, Yang Y, et al. Survival of Echinococcus multilocularis in the human host. Parasitol Int. 2006: 55 (Suppl): S51‑S55.
ARTICLE INFORMATION