Acute pulmonary embolism (PE), the most dangerous manifestation of venous thromboembolism, contributes highly to the global disease burden.1,2 The estimated early mortality risk in PE is used to guide decisions on diagnostic and therapeutic strategies.3 Pulmonary embolism can be classified depending on clot size and location. Saddle embolism is a type of PE with a prevalence of 2.6% to 5.4%.4 Importantly, saddle PE is not a synonym for massive PE, which is restricted to patients with hemodynamic compromise. However, it is associated with higher in‑hospital mortality and risk of delayed decompensation due to clot migration.4,5
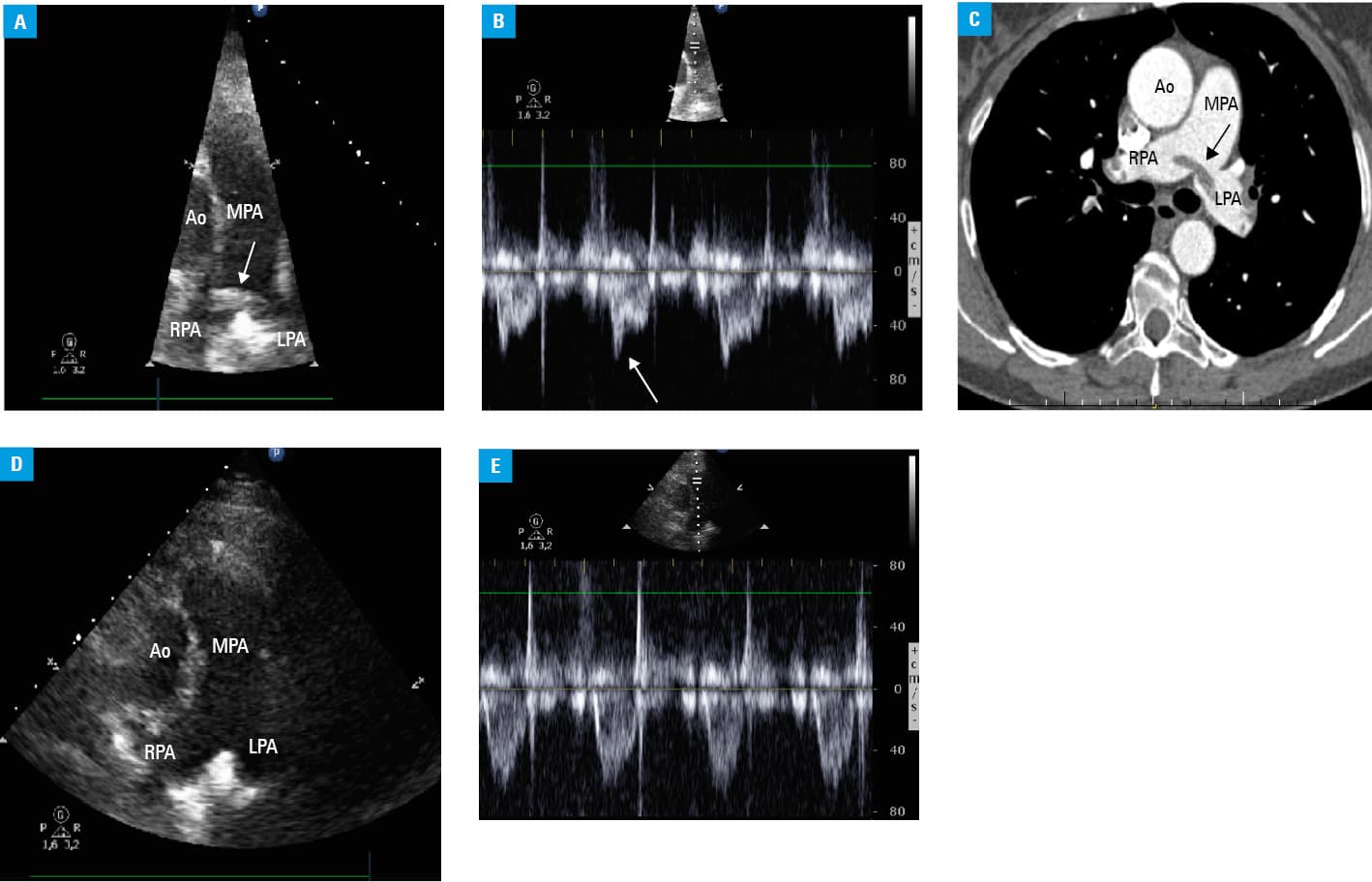
A 61‑year‑old woman presented to the emergency department with 1‑week history of mild exertional dyspnea and left calf pain. Two days before admission, a general practitioner recommended enoxaparin due to suspicion of deep vein thrombosis. On admission, the patient was stable with no resting dyspnea. Physical examination revealed a mild tenderness of left popliteal fossa with a negative Homans sign, without any edema. Electrocardiography showed sinus rhythm, 90 bpm, without any abnormalities. Based on the Wells rule (score, 2) and revised Geneva score (score, 3), the patient was classified as having an intermediate clinical probability of PE. However, transthoracic echocardiography (TTE) showed a mobile thrombus at the bifurcation of the pulmonary artery (Figure 1A). Spectral Doppler echocardiography revealed a short right ventricular outflow tract acceleration time and early systolic notching (Figure 1B). The right ventricular size and function were normal. Ultrasonography revealed also popliteal vein thrombosis. According to the guidelines,3 early mortality risk was assessed by the simplified Pulmonary Embolism Severity Index (score, 0) and biomarker levels (elevated high‑sensitive cardiac troponin and N‑terminal fragment of the prohormone brain natriuretic peptide) as intermediate‑low. Computed tomography angiography confirmed saddle embolus with thrombotic material in both main pulmonary arteries (Figure 1C). Despite formally nonmassive PE presentation, the patient was immediately admitted to the intensive care unit. Treatment with enoxaparin at therapeutic doses followed by rivaroxaban was administered. After 7 days, TTE did not show the thrombus (Figure 1D) and right ventricular outflow tract spectral Doppler signals were normal (Figure 1E).
According to the European Society of Cardiology guidelines,3 the role of TTE in a diagnostic algorithm is limited to suspected PE with shock or hypotension. It is not routinely recommended in stable, low‑risk patients because of its low negative predictive value. In a hemodynamically compromised patient, the search for signs of right ventricular pressure overload or dysfunction and mobile right heart thrombi is helpful in emergency management of primary reperfusion.
The presented case is specific in that TTE allowed us to make an immediate diagnosis of PE and change the risk assessment. Large PE was then confirmed by computed tomography. Quick bedside TTE in patients with a good acoustic window may provide a direct diagnosis and stratify patients as a potentially higher‑risk group. It may also be a useful tool for treatment monitoring.
- Raskob GE, Angchaisuksiri P, Blanco AN, et al. Thrombosis: a major contributor to global disease burden. Arterioscler Thromb Vasc Biol. 2014; 34: 2363‑2371. | Crossref
- Heit JA. The epidemiology of venous thromboembolism in the community. Arterioscler Thromb Vasc Biol. 2008; 28: 370‑372. | Crossref
- Torbicki A, Perrier A, Konstantinides S, et al. Guidelines on the diagnosis and management of acute pulmonary embolism: the Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). Eur Heart J. 2008; 29: 2276‑2315.
- Alkinj B, Pannu BS, Apala DR, et al. Saddle vs nonsaddle pulmonary embolism: clinical presentation, hemodynamics, management, and outcomes. Mayo Clin Proc. 2017; 92: 1511‑1518. | Crossref
- Torbicki A, Galié N, Covezzoli A, et al. Right heart thrombi in pulmonary embolism: results from the International Cooperative Pulmonary Embolism Registry. J Am Coll Cardiol. 2003; 41: 2245‑2251. | Crossref
ARTICLE INFORMATION