Critical stenosis of the left main coronary artery in an 82-year-old practicing physician



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Critical stenosis of the left main coronary artery in an 82-year-old practicing physician
According to the official data, about 22% of professionally active physicians in Poland have exceeded the age of 65 years and 10% are over 70 years of age.1,2 In the fields of pediatrics and gynecology, there are more than 40% of physicians older than 65 years of age. The mean age of specialists in the internal medicine is now 51.9 years, slightly above the mean age of Polish physicians, which is now 49.9 years.3 Among the active specialists in internal medicine, 28.5% are in the retirement age, 20.2% are over 65, and 11.7% are over 70 years of age.3
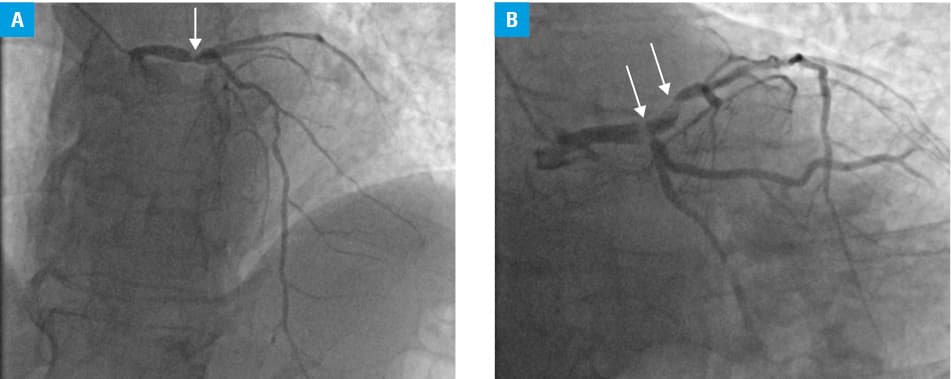
An 82‑year‑old physician with a 10‑year history of arterial hypertension, hyperlipidemia, and type 2 diabetes was referred to our unit for a scheduled angiography due to a 3‑month history of exertional chest discomfort. His concomitant diseases were well controlled with perindopril (5 mg/d), bisoprolol (5 mg/d), torsemide (10 mg/d), amlodipine (5 mg/d), and rosuvastatin (10 mg/d). He has received insulin in a dose of 40 to 50 U/d for 5 years. He was normal weight (body mass index, 26.83 kg/m2), a nonsmoker, and physically active. On admission, his blood pressure was 140/80 mm Hg; total cholesterol level, 130 mg/dl; glycated hemoglobin, 6.3%; and creatinine, 1.0 mg/dl. On echocardiography, the left ventricle was normal in size (53 mm) with slight septal hypokinesis and global ejection fraction of 50%. The symptoms were moderate, not limiting the patient’s activity, and on the previous day, he had consulted 37 patients in a primary care outpatient department. Angiography showed a critical stenosis in the distal part of the left main coronary artery (Figure 1A), with a large thrombus penetrating and occluding the ostium of the left anterior descending and circumflex arteries (Figure 1B). The patient remained in the hospital, and underwent an urgent coronary artery bypass surgery with the left internal mammary artery to the left anterior descending artery and saphenous graft to the circumflex artery. He was discharged on the 6th day after surgery. His recovery and rehabilitation were uncomplicated, and he returned to his office and routine activity 2.5 months after the surgery.
There is a growing shortage of physicians in the Polish medical system, especially in primary care units. However, the basic salary of Polish physicians remains the lowest in Europe as compared with the mean national personal income. The “opt‑out” procedures and so‑called contracts with self‑employed physicians were created as solutions to those deficits. They allow physicians to practice without any control of their work hours, but on the other hand, they eliminate any responsibility that should lie with the institutions appointed to organize medical care and respect the labor law in Poland.
In the recent years, health complications and deaths related to overwork have been discussed mostly in relation to our younger and middle‑aged colleagues, that is, residents and specialists. However, there is no information about the medical consequences of overwork on the growing population of senior physicians who are forced to continue working despite their advanced age.
The growing number of professionally active senior physicians forms a novel group of high‑risk patients because of years of overtime work with responsibility much higher than average. Medical councils in cooperation with occupational medicine authorities should prepare a special program of medical inspection that should be protective but not oppressive for our professionally active senior colleagues.
- Baliński P, Krajewski R. Physicians and dentists in Poland ‑ demographic characteristics. State as of December 31, 2017 . Naczelna Izba Lekarska. 2018. ISBN 978‑83‑948240‑2‑0.
- Janik J. Retired physicians save Polish medical system from a personnel disaster . Rynek Zdrowia. November 9, 2018.
- Jodłowski M, Kędzierski M. Central registry of physicians and dentist in Poland. State as of December 31, 2018 . Naczelna Izba Lekarska.
ARTICLE INFORMATION