Severe sight-threatening thyroid-associated orbitopathy successfully treated with combined systemic glucocorticoids and intravitreal injections of antibiotics



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Severe sight-threatening thyroid-associated orbitopathy successfully treated with combined systemic glucocorticoids and intravitreal injections of antibiotics
Thyroid‑associated orbitopathy (TAO) is an autoimmune inflammatory process affecting orbital tissues. It is the most frequent extrathyroidal manifestation of Graves disease (GD), with its severe form affecting from 3% to 6% of patients.1
A 59‑year‑old nonsmoking woman was admitted due to vision deterioration and purulent secretion from the eyes observed for 1 week. She was clinically and biochemically hyperthyroid, with undetectably high anti–thyroid‑stimulating hormone receptor antibodies and features of GD on thyroid ultrasound. She had a history of schizophrenia treated by an intramuscular injection of zuclopenthixol depot (200 mg for 21 days) due to noncompliance.
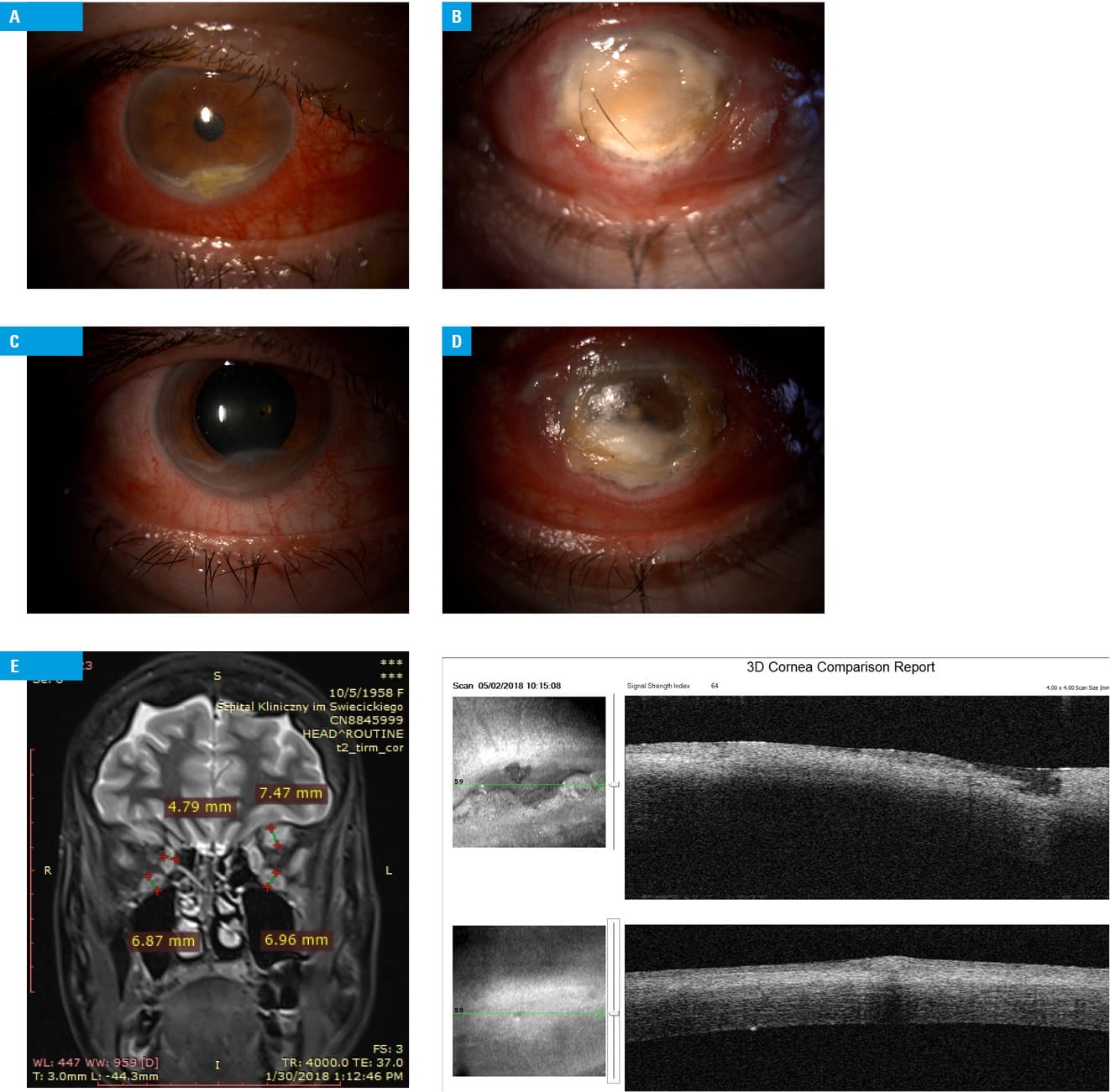
Clinical examination and magnetic resonance imaging (MRI) suggested active TAO (Figure 1A–1C). Regarding the criteria of dysthyroid optic neuropathy, bilateral apical crowding of the optic nerve on MRI and deteriorated visual acuity (0.1 by Snellen chart) in the right eye, but without optic disc edema and only light perception in the left eye, were detected (left optic disc edema could not be evaluated due to corneal lesions).2
The patient received interdisciplinary care of endocrinologists, ophthalmologists, and psychiatrists. First, propranolol (3 × 20 mg/d) and thiamazole (3 × 20 mg/d) were introduced. For TAO, intravenous methylprednisolone (3 g for 3 days) and then oral methylprednisolone (40 mg/d) with intravenous ciprofloxacin (2 × 200 mg) were administered. A decision on continuation of oral glucocorticoid therapy was made with the aim to achieve better compliance following hospital discharge, while olanzapine (10 mg/d) was added as prevention of psychosis. Intravitreal antibiotics (vancomycin, 1 mg; ceftazidime, 2.25 mg) were administered. Artificial tears during the day, eye patches with retinol and dexpanthenol ointment during the night, as well as eye ointment with antibiotics (ofloxacin, moxifloxacin) during the day and night were used under moisture chambers. Once biochemical euthyroidism was achieved, the patient underwent radioiodine therapy but refused consent to tarsorrhaphy or orbital decompression.
At 6‑week follow‑up, a significant improvement was observed (Figure 1D–1F). We noted improved hydrostatic pressure and vascular perfusion, as well as reduced orbital congestion. Asymmetric bilateral proptosis was 16 mm (right eye) and 21 mm (left eye). Motion restriction was still observed (left eye), while in the right eye, a small limitation in extreme gaze was present.
In patients with GD and TAO, restoration of euthyroidism is essential. Although radioiodine is not the first‑line therapy, it was applied in our patient due to concerns about future compliance to pharmacotherapy and lack of consent to thyroidectomy. The risk of TAO exacerbation is lower in nonsmokers3 and might be alleviated with glucocorticoids.4 The management of bacterial keratitis is not widely covered by guidelines on TAO. To the best of our knowledge, this is the first report on the application of intravitreal antibiotic injection in the management of bacterial complications of TAO. Optic neuropathy often requires urgent orbital decompression.1 A novel option for such patients includes rituximab or tocilizumab,5 but it was unavailable at the time.
In conclusion, we demonstrated treatment difficulties in a patient with schizophrenia and GD, hyperthyroidism, and sight‑threatening TAO complicated with bacterial keratitis, where a multidisciplinary therapy and an individualized approach allowed us to avoid enucleation and prevent complete sight loss. Such treatment is recommended only in specialized referral centers.
- Bartalena L, Baldeschi L, Boboridis K, et al. The 2016 European Thyroid Association/European Group on Graves’ orbitopathy guidelines for the management of Graves’ orbitopathy. Eur Thyroid J. 2016; 5: 9‑26. | Crossref
- Miskiewicz P, Rutkowska B, Jablonska A, et al. Complete recovery of visual acuity as the main goal of treatment in patients with dysthyroid optic neuropathy. Endokrynol Pol. 2016; 67: 166‑173.
- Wiersinga WM. Graves’ orbitopathy: management of difficult cases. Indian J Endocrinol Metab. 2012; 16: S150‑S152.
- Ruchała M, Sawicka‑Gutaj N. Advances in the pharmacological treatment of Graves’ orbitopathy. Expert Rev Clin Pharmacol. 2016; 9: 981‑989. | Crossref
- Perez‑Moreiras JV, Gomez‑Reino JJ, Maneiro JR, et al. Efficacy of tocilizumab in patients with moderate to severe corticosteroid resistant Graves orbitopathy: a randomized clinical trial. Am J Ophthalmol. 2018; 195: 181‑190. | Crossref
ARTICLE INFORMATION