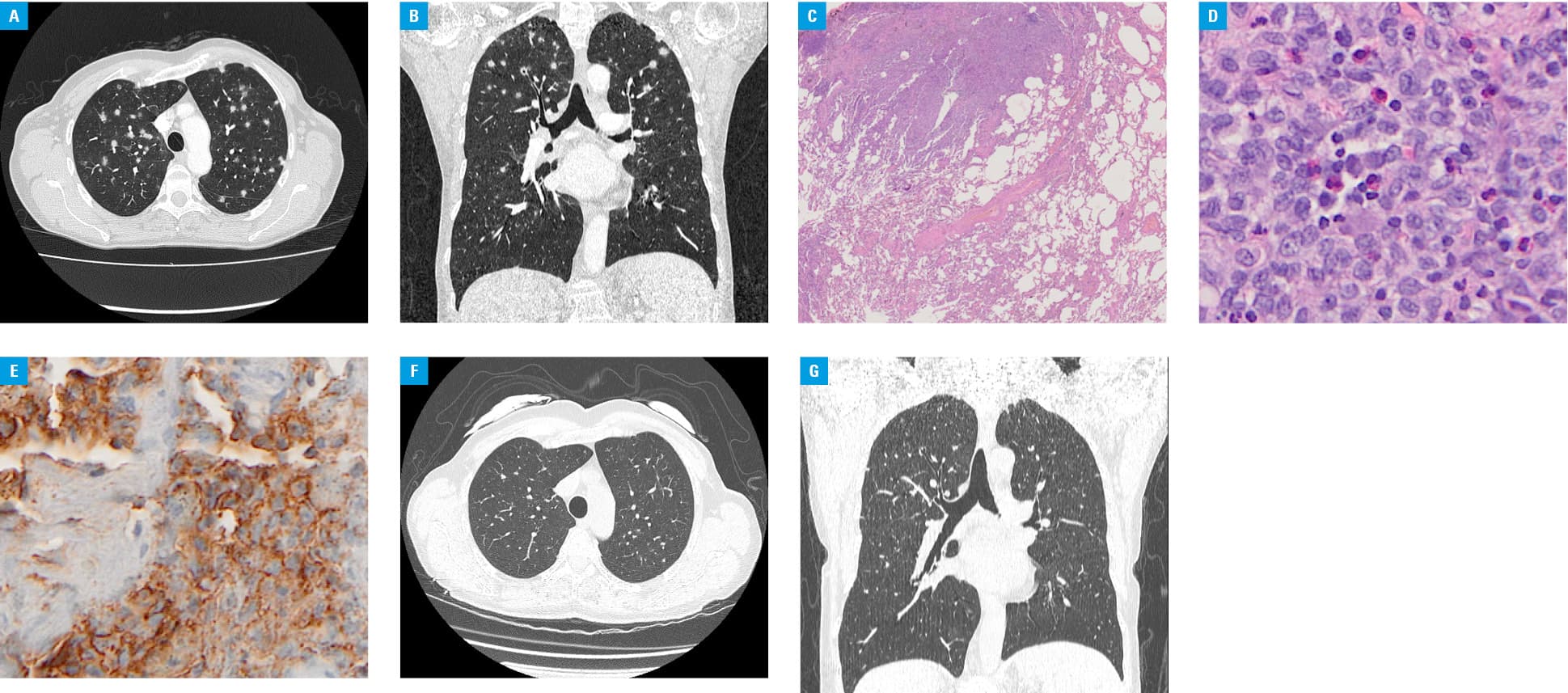
A 59‑year‑old female smoker (20 pack‑years) was admitted to the department of thoracic surgery with a suspicion of breast cancer metastasis to the lung. Two years earlier, she was treated with surgery for left breast invasive ductal cancer (T2N0M0 according to the TNM classification) with estrogen receptor positivity, and subsequently with hormonal therapy. Two months before admission, the patient had a pulmonary infection and was treated with antibiotics. Control chest X‑ray revealed multiple round nodules in both lungs. Chest computed tomography (Figure 1A and 1B) showed multiple small nodules with a centrilobular distribution, and varying degrees of cavitation. The nodules were most prominent in the upper and middle lung zones with no involvement of the supradiaphragmatic regions. There was moderate enlargement of the mediastinal lymph nodes. There were no bone lesions or changes on abdominal ultrasound. A pulmonary function test and 6‑minute walk test revealed normal results (forced expiratory volume in 1 second, 83% predicted; forced vital capacity, 99% predicted; total lung volume, 108% predicted; and transfer factor for carbon monoxide, 76% predicted). The patient underwent video‑assisted thoracoscopy, and histological examination of the lung sample revealed infiltration of large cells with folded nuclei forming granulomas (Figure 1C and 1D). These cells were positive for CD1a antigen (Figure 1E), establishing a diagnosis of Langerhans cell histiocytosis (LCH). The patient stopped smoking, and high‑resolution computed tomography (HRCT) of the chest (Figure 1F and 1G) showed substantial partial regression of the lesions.
Pulmonary LCH (PLCH) is a rare disease caused by clonal proliferation and infiltration of various organs by abnormal bone marrow–derived Langerhans cells.1-3 It usually affects patients at a mean age between 30 and 40 years. In a group of adult patients with PLCH, approximately 90% had a history of smoking.2 Langerhans cell histiocytosis may be limited to the lungs, or the lungs may be just one of the many involved organs, both at the time of diagnosis and during follow‑up.1-3 In 20% of patients, PLCH is detected incidentally as an abnormality on chest radiography, and an additional 15% to 30% of patients have a pneumothorax as their first symptom. HRCT can reveal centrilobular nodules, nodules with or without cavitation, and initially thick‑walled cysts of various shapes that are often confluent. As the disease evolves, the cysts become larger and thin‑walled. In the majority of adult patients (~90%), the costophrenic angles are spared. Isolated multiple nodular lesions are rare and seen in only 10% of cases.1-4 The most important treatment for PLCH is smoking cessation, which leads to partial regression and further stabilization in approximately 50% of patients.1-4
There is a strong correlation between LCH and malignancy (~30%),5 which precedes LCH development in 56% of patients. In contrast to the mean age of the general population of PLCH patients, patients with LCH coexisting with malignancy are diagnosed at an age between 50 and 60 years.5
This case involved an older patient with a history of malignancy and HRCT findings suggesting disseminated cancer. The remarkable regression after smoking cessation alone supports the critical role of this treatment strategy in PLCH.
- Radzikowska E. Pulmonary Langerhans cell histiocytosis in adults. Adv Respir Med. 2017: 85; 277‑289. | Crossref
- Vassallo R, Ryu JH, Schroeder DR, et al. Clinical outcomes of pulmonary Langerhans cell histiocytosis in adult. N Eng J Med. 2002; 346: 484‑490. | Crossref
- Girschikofsky M, Arico M, Castillo D, et al. Management of adult patients witch Langerhans cell histiocytosis: recommendations from an expert panel on behalf of Euro‑Histio‑Net. Orphanet J Rare Dis. 2013; 8: 1‑11. | Crossref
- Tazi A, de Margerie C, Naccache JM, et al. The natural history of adult pulmonary Langerhans cell histiocytosis: a prospective multicentre study. Orphanet J Rare Dis. 2015; 10: 30. | Crossref
- Ma J, Larid JH, Chau KW, et al. Langerhans cell histiocytosis in adults is associated with a high prevalence of hematologic and solid malignancies. Cancer Med. 2019; 8: 58‑66. | Crossref
ARTICLE INFORMATION