Hymenoptera sting in the head and neck region is not a risk factor for grade IV systemic reactions in patients with venom allergy
Key words: grade IV allergic reaction, Hymenoptera insect stings, sting site



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Hymenoptera sting in the head and neck region is not a risk factor for grade IV systemic reactions in patients with venom allergy
Introduction: Hymenoptera insect stings (ISs) in the head and neck (H&N) region are commonly considered to be a risk factor for grade IV systemic reactions (SRs) in patients with Hymenoptera venom allergy (HVA). However, clinical data addressing this issue are scarce.
Objectives: The aim of our study was to verify whether ISs in the H&N region were related to a higher risk of grade IV SRs in patients with HVA.
Patients and methods: This retrospective cross‑sectional study included 195 patients aged 2 to 74 years and treated with venom immunotherapy due to at least a grade II SR to ISs. The study sample comprised 109 adults (56%; mean [SD] age, 41.08 [14.62] years; male, 50.5%) and 86 children (mean [SD] age, 9.53 [4.37] years; male, 72.1%; P <0.001 for age and P = 0.002 for sex). The IS site was divided into 7 categories.
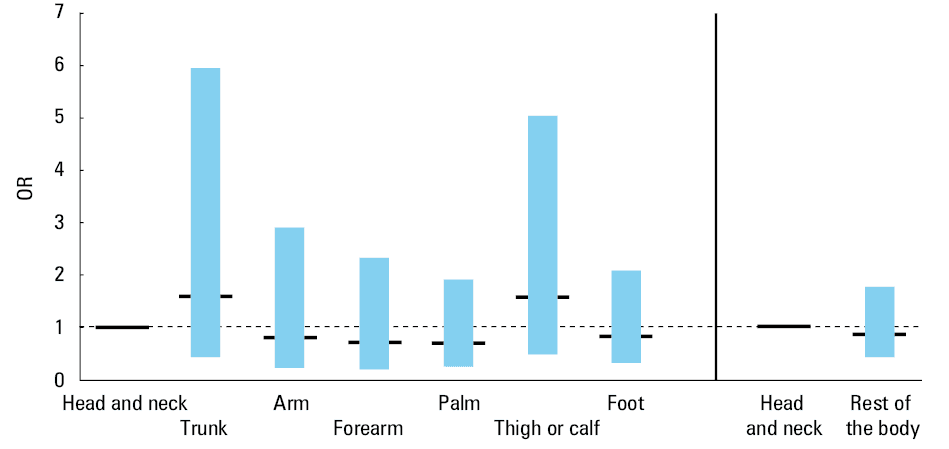
Results: The H&N region was the most common site for the IS (one‑third of the study group). In the entire study population, the risk of grade IV SRs was numerically, though insignificantly higher for ISs in the trunk (odds ratio [OR], 1.58; 95% CI, 0.42–5.92; P = 0.50) and legs (OR, 1.56; 95% CI, 0.49–5.10; P = 0.45), as compared with the H&N region. The H&N region showed a similar risk of grade IV SRs when compared with all the other IS sites combined into a single category (OR, 0.87; 95% CI, 0.43–1.75, P = 0.7).
Conclusions: ISs in the H&N region were not confirmed to be a risk factor for grade IV SRs in patients with HVA, regardless of age and sex.
Introduction
Hymenoptera is a family of insects with membranous wings, whose stings can cause an allergic reaction, mostly mediated by immunoglobulin E. The reaction manifests either as a large local reaction (LLR; 5%–15%, up to 26% of cases) or a systemic reaction (SR; 3%–9% of adults and about 10 times less in children).1 LLRs are defined as edema and erythema at the sting site, exceeding 10 cm in diameter and lasting over 24 hours. On the other hand, SRs include skin, gastrointestinal, respiratory, and cardiovascular symptoms that develop either separately or in any combination of the above. Typically, clinical classification of SR severity is based on a 4‑grade scale, with the leading symptoms ranging from the mildest to the most severe (I, urticaria; II, vomiting; abdominal pain; III, respiratory disorders; and IV, anaphylactic shock).2 This classification applies to all age groups. Both LLRs and SRs are most common in the highly exposed groups, such as beekeepers (LLRs up to 38%, SRs up to 43%).2 According to the European network of severe allergic reactions (Network of Online Registration for Anaphylaxis, NORA) data, insect stings (ISs) are the most common cause of anaphylaxis in adults (51%), and the second one in children (21%).3 Worm et al4 reported that out of all anaphylaxis cases triggered by Hymenoptera, 67.95% were due to wasp stings, and 21.11%, to bee stings. In the case of ISs, the severity of an SR depends on the kind of venom, its dose, and time intervals between stings. There are also other patient‑dependent risk factors, including elevated baseline serum tryptase levels, mastocytosis, adult age, and cardiovascular diseases treated with β-blockers.5 The Hymenoptera stings in the H&N region are commonly regarded as a risk factor for a fatal outcome6;however, some investigators reported that there was no such correlation in adult population.7 There are scarce data addressing this issue in children.8
We decided to verify whether ISs in the H&N region were related to a higher risk of grade IV SRs in patients with Hymenoptera venom allergy (HVA), and to determine whether such an association was age dependent. To the best of our knowledge, no studies have been published on this particular topic so far.
Patients and methods
It was a cross‑sectional retrospective study conducted from 2014 to 2018 at 3 reference centers for HVA management in Poland, including the Department of Pediatrics at the University Children’s Hospital of Cracow, the Department of Clinical and Environmental Allergology in Kraków, and the Department and Clinic of Internal Medicine and Allergology in Wrocław. The study group included 195 patients (age, 2–74 years) with a history of at least grade II anaphylactic reaction (according to the system by Mueller)6 due to an IS, treated with venom immunotherapy (VIT) in one of the above centers. A structured questionnaire (Supplementary material, Appendix S1) was used to collect detailed information on the most severe reaction after an IS that had become a reason for VIT. Adults and children aged 12 years or older completed the questionnaires on their own. In the case of patients younger than 12 years, the questionnaires were completed by their parents. When describing sex groups, the terms “men” and “women” were used for adults, and the terms “boys” and “girls,” for children. The terms “males” and “females” applied to the whole population, regardless of age. The questions referred to general demographic data, such as the patient’s age and sex, and medical history, such as the date of the Hymenoptera sting or the presence of beehives in the neighborhood.
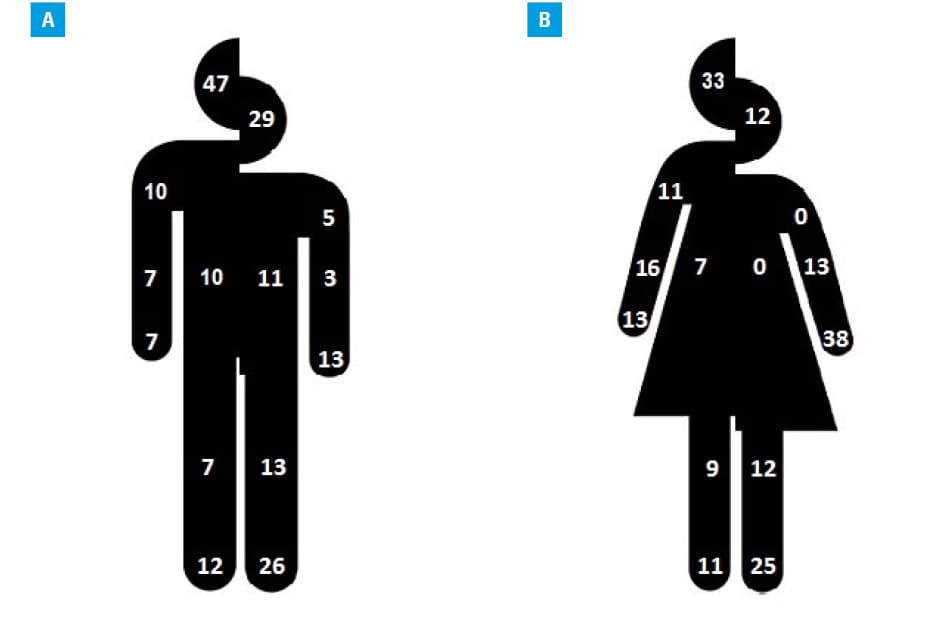
The site of the IS was determined both by pinpointing the place on the front and back side pictures of the body and by written or oral description. The IS sites were further divided into 7 categories: H&N, trunk, arms, forearms, palms, thighs or calves, and feet. The SRs were classified according to the system proposed by Mueller as follows: grade I, generalized urticaria, itching, malaise, or anxiety; grade II, any of the previous ones plus 2 or more of the following: angioedema, chest constriction, nausea, vomiting, diarrhea, abdominal pain, or dizziness; grade III, any of the previous ones plus 2 or more of the following: dyspnea, wheezing, stridor, dysarthria, hoarseness, weakness, confusion, or a feeling of impending disaster; and grade IV, any of the previous ones plus 2 or more of the following: fall in blood pressure, collapse, loss of consciousness, incontinence, or cyanosis.6 In all cases, self‑reported symptoms were verified by medical staff with the original medical records related to an intervention during an SR. The questions concerned the most severe anaphylactic reaction to an IS that resulted in VIT, but we also asked about the number of ISs in the past, the number of insects that caused the reported reaction, and the type of culprit insect, which in Poland could be categorized either as bees (Apis mellifera) or wasps (Vespula vulgaris) with hornets (Vespa crabro) (due to similar venom characteristics). The patient’s place of residence was categorized either as a town or a country, based on a postal code.
The study protocol was approved by the Jagiellonian University ethics committees (No. KBET/126/B/2012). Adult patients, children older than 16 years, and parents of all children provided written consent to participate in the study.
Statistical analysis
The distribution of qualitative variables was presented using frequencies and percentages, whereas quantitative variables were presented as means and SD in the case of normal distribution and as medians and quartiles in the case of nonnormal distribution. The χ2 test was used to examine an association between 2 qualitative variables. The difference in age between study groups was confirmed using the t test for independent samples.
Four logistic regression models were constructed to assess factors influencing the severity of a Hymenoptera sting–induced anaphylactic reaction. Two models compared the odds ratio (ORs) of grade IV SRs related to the sting site subdivided into 7 categories, with the H&N region considered as a reference category. The other 2 models compared the H&N region with all the other regions combined into a single category and considered as a reference. In each pair of the above models, one compared children and adults (18 years of age was the age limit for adulthood) and the other compared the age groups divided by 10‑year intervals, with the youngest one considered as a reference category. All models were adjusted for sex (with men as a reference category), culprit insect (with hornet and wasp as a reference category), and place of residence (with towns as a reference category). Interactions between all variables were tested.
The results with a P value of less than 0.05 were treated as significant. The IBM SPSS Statistics 24 for Windows software was used (IBM, Armonk, New York, United States).
Results
Demographic characteristics
The study included 195 patients with confirmed HVA: 109 adults (56%; mean [SD] age, 41.08 [14.62] years) and 86 children (44%; mean [SD] age, 9.53 [4.37] years, P <0.001). The groups differed with regards to sex (50.5% of male patients among adults and 72.1% of male patients among children, P = 0.002). The number of rural inhabitants was higher compared with their city counterparts, and there was a higher number of boys living in the country regions (P <0.001).
Type of culprit Hymenoptera insects
There was no difference in the types of culprit Hymenoptera insects between adults and children (P = 0.05). The most common Hymenoptera stings in adults were those by wasps (54%), and in children, by bees (54%) (Table 1). Female patients, regardless of their age, were mostly stung by wasps, while in the male population, boys were more frequently stung by bees compared with men (P = 0.01). The beehive location was an important factor, because 73% of the 78 patients stung by bees had a beehive either right next to their house (41%) or in the neighborhood (32%). In the group stung by bees, children had a beehive in their closest surroundings twice more often than adults (53.7% vs 27%), whereas the neighborhood localization resulted in a comparable rate of bee stings in both adult and pediatric populations (31.7% vs 32.5%, P = 0.02). The number of stings in the past varied between 1 and 4; however, the number did not influence the severity of the reaction regardless of age and sex (data not shown). There was a difference in the type of the culprit Hymenoptera insect with respect to the place of residence. In the entire study group, wasp stings predominated in the town population, while bee stings were most common in the rural area (61.5% vs 53.8%, P = 0.01). When the study group was divided by age, a similar pattern was observed in adults (63.9% for wasp stings and 50% for bee stings, P = 0.04), but not in children (52.9% for wasp stings and 56% for bee stings, P = 0.42).
Adults | Children | Total | ||
Data are presented as number (percentage) of patients.
The P value expresses the difference in the type of the culprit insect between children and adults with respect to sex or in the whole group.
Abbreviations: NS, nonsignificant | ||||
Male
P = 0.01 | Wasp | 28 (50.9) | 22 (35.5) | 50 (42.7) |
Bee | 19 (34.5) | 38 (61.3) | 57 (48.7) | |
Hornet | 8 (14.5) | 2 (3.2) | 10 (8.5) | |
Total | 55 (100) | 62 (100) | 117 (100) | |
Female
P = NS | Wasp | 32 (59.3) | 14 (58.3) | 46 (59.0) |
Bee | 21 (38.9) | 9 (37.5) | 30 (38.5) | |
Hornet | 1 (1.9) | 1 (4.2) | 2 (2.6) | |
Total | 54 (100) | 24 (100) | 78 (100) | |
Total
P = 0.05 | Wasp | 60 (55.0) | 36 (41.9) | 96 (49.2) |
Bee | 40 (36.7) | 47 (54.7) | 87 (44.6) | |
Hornet | 9 (8.3) | 3 (3.5) | 12 (6.2) | |
Total | 109 (100) | 86 (100) | 195 (100) | |
Severity of systemic reaction
The most frequent clinical diagnosis in both age groups was the most severe SR (ie, grade IV); however, it was more common in adults than in children (72.5% vs 48.8%) (Table 2). A similar trend was also observed in sex groups (70.9% of men vs 46.8% of boys and 74.1% of women vs 54.2% of girls). There was a difference in the distribution of the severity grades between male adults and children (P = 0.01), but no such difference was observed for the female group (Table 2). There was no difference in the severity of clinical symptoms between wasp and bee stings. The severity of the reaction was not evaluated with respect to concomitant mast cell activation syndrome either in adults or in children.
Gradea | Adults | Children | Total | ||||
Female | Male | Female | Male | Adults | Children | Total | |
Data are presented as number (percentage) of patients.
a P = 0.001 (difference in the severity of a systemic reaction between children and adults) | |||||||
II | 3 (6) | 4(7) | 3(13) | 15(24) | 7 (6.4) | 18 (20.9) | 25 (12.8) |
III | 11 (20) | 12 (22) | 8 (33) | 18 (29) | 23 (21.1) | 26 (30.2) | 49 (25.1) |
IV | 40 (74) | 39 (71) | 13 (54) | 29 (47) | 79 (72.5) | 42 (48.8) | 121(62.1) |
Total | 54 (100) | 55 (100) | 24 (100) | 62 (100) | 109 (100) | 86 (100) | 195 (100) |
Site of the insect sting
Overall, the most frequent IS site was the H&N region (one third of the whole study population). Adults were most often stung in the H&N region, followed by the feet and forearms, while in children, the most common site was the feet, followed by the H&N region and hands (Table 3). The difference in IS sites between children and adults was significant (Table 3). When the study group was divided according to sex, more male patients were stung in the H&N region than females (37.6% vs 26.9%). This trend was observed both in children (29% for boys and 12.5% for girls) and adults (47.3% for men and 33.3% for women). The H&N region was the most frequent IS site in all subgroups except girls, in whom the most common site was the hands (37.5%) (P = 0.02 compared with women, P = 0.03 compared with boys). Two adult individuals, female and male, were stung by a wasp in the lower lip, which resulted in grade IV and grade III SRs, respectively. None of the children were stung in the tongue or mouth.
Sting sitea | Adults | Children | Total |
Data are presented as number (percentage) of patients.
a P = 0.001 (difference in the site of an insect sting between children and adults) | |||
Head and neck | 44 (40.4) | 21 (24.4) | 65 (33.3) |
Trunk | 9 (8.3) | 7 (8.1) | 16 (8.2) |
Arm | 11 (10.1) | 3 (3.5) | 14 (7.2) |
Forearm | 12 (11.0) | 5 (5.8) | 17 (8.7) |
Palm | 11 (10.1) | 17 (19.8) | 28 (14.4) |
Thigh and calf | 9 (8.3) | 11 (12.8) | 20 (10.3) |
Foot | 13 (11.9) | 22 (25.6) | 35 (17.9) |
Total | 109 (100) | 86 (100) | 195 (100) |
The site of the sting in relation to age and sex is shown in Figure 1. There were no significant differences in IS sites between the types of venom allergy groups, regardless of age. The frequency of stings in the H&N region was comparable for wasp and bee stings (30.8% and 35.3%, respectively). In adults, the H&N region was the most common site for wasp and bee stings (29.2% and 57.9%, respectively, P = 0.01). The H&N region was also the most common site for wasp stings in children (33.3%), while bee stings were almost twice less frequent (17%). The foot was the most frequent site for bee stings in children (29.8%). In adults, grade IV SRs occurred most often when the IS site was the trunk (100%), followed by the calf (88.9%) and the H&N region (72.27%). In children, anaphylaxis occurred when they were stung in the arm (66.7%), calf (54.5%), and H&N region (52.4%). In both age groups, regardless of sex, there was no association between the frequency of grade IV SRs and the IS site (P = 0.35 and P = 0.99 for adults and children, respectively).
Multivariable analysis
The analysis of each of the 6 body regions as compared with the H&N region in the whole population showed that the risk of grade IV SRs was numerically, though insignificantly, higher for ISs in the trunk (OR, 1.58; 95% CI, 0.42–5.92; P = 0.5) and legs (OR, 1.56; 95% CI, 0.49–5.10; P = 0.45) in comparison with the H&N region (Figure 2). The analysis of the 6 body parts combined into a single category and compared with the H&N region resulted in a similar risk of grade IV SRs in the H&N region (OR, 0.87; 95% CI, 0.43–1.75; P = 0.7) (Figure 2). There was no significant association between age and IS site; therefore, the relationship between the site of Hymenoptera sting and severity of an allergic reaction was similar in both age groups. The detailed results of the multivariable analysis concerning the association of grade IV SRs and age are available in Supplementary material, Appendix S2.
Discussion
Anaphylaxis, which is an increasingly common topic in epidemiological studies,9-11 is a severe and potentially fatal grade IV SR frequently triggered by ISs. To ensure an appropriate medical intervention, it is important to identify the risk factors for severe reactions. The issue is clinically relevant also for emergency department staff, because ISs in the H&N region often result in serious local edema and are commonly considered to be a risk factor for severe SRs. Objective data on this topic in adults are scarce, and to our knowledge, there has been no research addressing the severity of a reaction to an IS with respect to the sting site in pediatric population or comparing the severity of a reaction to Hymenoptera sting between children and adults with respect to sting site.8 Our study is the first to evaluate the relationship between grade IV SRs and the IS site, with a special focus on the H&N region in the Polish population of children and adults with HVA undergoing VIT. At the end of the study (2018), the total number of VIT‑treated patients in Poland was estimated at 3090, with an adult‑to‑child ratio of 5:1, which means that our study included 4.4% of adults and 17.2% of children of the entire Polish population treated with VIT at the time.12 The current results are comparable with our preliminary data from a previous study, which included half of the current sample.13
Site of insect sting
Previous studies identified a relationship between an IS in the face or neck and grade IV SRs, but the data were not objectively verified.6 Stoevesandt et al14 were the first to evaluate risk factors for severe anaphylaxis, such as IS site, age, comorbidities, baseline serum tryptase levels, and concomitant drugs. In their study, the body regions were divided into 6 categories: H&N, hand, arm, foot, leg, and trunk. The majority of patients (29.7%) had been stung in the H&N region. This is in line with our results, except that girls were stung mostly in the hand. Stoevesandt et al14 identified 4 significant indicators or risk factors for severe anaphylaxis, including elevated baseline serum tryptase levels, absence of urticaria or angioedema during anaphylaxis, time interval of less than 5 minutes from the sting to onset of symptoms, and senior age.14 However, the authors only used a univariate analysis so they could not confirm a causal relationship between the analyzed variables.
Arzt et al7 hypothesized that severe reactions were more frequent following a sting in the H&N region due to the presence of thin reticular dermis. To confirm this, they evaluated the stinger’s depth of penetration in different parts of the body in the murine model. They observed that the stinger in the back got stuck in the rarely supplied reticular dermis, whereas in the face, it reached the deep arteriovenous plexus of the subcutis. In their observation of 847 patients aged 9 to 85 years with confirmed HVA, only 16.3% of patients with severe reactions were stung in the head (P = 0.017), and symptom severity was independent from the IS site.7 The authors concluded that advanced age, elevated baseline tryptase levels, and the absence of cutaneous signs were associated with severe sting‑related SRs, while sting site, sex, and type of venom were not the risk factors.7 These results are in line with our observations. In the univariate analysis, we confirmed that the H&N region was the major site of IS in the total study sample, in adults regardless of sex, and in boys. The IS in the H&N region was not a risk factor for grade IV SRs in any of the age or sex groups. In the multivariate analysis comparing the 6 body sites with the H&N region, the risk of grade IV SRs was nonsignificantly higher for ISs in the trunk and legs. When all the 6 body sites were combined in a single category, the ISs in the H&N region were associated with a nonsignificantly higher risk of grade IV SRs. This relationship was independent of the patient’s age.
There were no significant differences between children and adults in the severity of the reaction with respect to the IS site. Grade IV SRs in adults were most common when the IS site was the trunk, calf, and H&N region, whereas in children, the arm, calf, and H&N region.
High incidence of the IS site in the H&N region might be due to the fact that it is usually an uncovered part of the body. However, the higher incidence of stings in this region in male than in female patients questions the hypothesis that fragrances worn by women attract more stinging insects. This concept was put forward many years ago, but it has not been supported by any peer‑reviewed literature.15 In a study by Braun et al,16 which included 143 Swiss adult residents (age, 19–84 years), the most common site of Hymenoptera sting was the head (22.5%). However, when data were analyzed with respect to the patient’s sex, the most frequent site became the feet and hands in women, and the legs and head in men. In contrast to our study, the authors included patients admitted to the emergency department because of the most recent acute reaction to a Hymenoptera sting. They also used the Mueller’s classification to determine the severity of the reaction to an IS, but they did not evaluate the relationship between the severity and the site of the IS.16
Braun et al16 suggested that ISs occurred in the foot especially in women because they more often wear open sandals and thus have higher skin exposure compared with men, who usually wear closed shoes. In our study, we observed that feet were a frequent site of stings in children. This may result from the fact that children often walk barefoot. It was shown that children were stung in the feet by bees and not wasps, which is surprising because, unlike bees, wasps, in particular the wild ones, build their nests in the ground.17 To avoid an IS in this particular location, some preventive measures were recommended, such as avoidance of barefoot walking.18
In our study, 2 patients reported an IS in the mouth or tongue, which resulted in either grade IV or grade III SR. The most common risk behavior to suffer from Hymenoptera stings in the oral region was drinking sweet beverages or eating; therefore, this should be avoided as a preventive measure.18 In the study by Braun et al,16 there were 11.6% of intraoral stings, mostly due to lack of attention during drinking. Surprisingly, the risk of anaphylaxis following subsequent Hymenoptera stings in patients with a previous LLR, even in the intraoral region, was not much higher than the risk in the general population and ranged from 5% to 15%.19 However, even an LLR due to an IS in the mouth or tongue region might still be fatal because of tissue edema narrowing the upper respiratory tract, which requires an immediate aggressive medical intervention.20
An interesting finding in our study was that girls were predominantly stung in the hand. We hypothesized that it might be due to their defensive behaviors, such as waving hands or covering the face with the hands to protect themselves from the sting. In a Turkish study, the upper limb was also indicated as the most frequent location of IS in children (43%), regardless of sex.8
Demographic data and types of stinging Hymenoptera insect
In Europe, ISs are predominantly caused by wasps, followed by bees and yellow hornets, as reported in original studies as well as in the NORA database.3,4 Our data support previous results that the worldwide incidence of Hymenoptera stings is usually similar regardless of sex in adult population, while among children, boys were up to 3‑fold more frequently stung than girls.21-25 This may result from the fact boys undertake more outdoor activities and risky behaviors than girls or adults working mostly indoors. This is in line with the results of von Moos et al,23 who indicated that living mainly in a rural environment resulted in a high sting incidence not only among beekeepers and their family members, but also outdoor workers with vespid venom allergy. In contrast, indoor occupation and the absence of a beehive in the neighborhood resulted in a very low risk to sting exposure, regardless of the type of venom allergy.23 In an earlier Swiss study, beekeepers and their family members were classified as a group at high risk of ISs as well as severe anaphylaxis from an IS.26 Also in our study, residence in the vicinity of beehives was potentially an additional risk factor for being stung by a bee. We understand that a high number of children exposed to bee stings and stung by a bee in our study might cause a bias towards overestimation of bee stings. Nevertheless, both models of the multivariate analysis in our study population confirmed, similarly to the study by von Moos,23 that living in the village increased the risk of grade IV SRs, regardless of the type of the Hymenoptera insect or the patient’s age.
Severity of reaction
There is no universal classification of anaphylactic reactions. The available 4‑grade classifications of the severity of SRs to IS were established in the 1960s (by Mueller)6 and 1970s (by Ring and Messmer27). More recently, a few authors adapted 3‑grade classifications (Brown28 and Muraro et al29) to evaluate systemic allergic reactions to Hymenoptera venom, but they did not become a standard in clinical practice.14 Most studies that examined ISs used the classifications by Mueller or Ring and Messmer. However, both scales have some limitations: the one by Mueller does not recognize that an isolated cardiovascular shock might be the only sting‑induced allergic manifestation, while the other almost entirely focuses on the cardiovascular collapse, which it considers more severe than respiratory symptoms. We decided to use the Mueller’s classification as it is most common in specialist centers in Poland.
Overall, we believe that our results significantly contribute to the knowledge about a presumed correlation between Hymenoptera stings in the H&N region and severe anaphylaxis. Our analysis showed that there is no such correlation, proving this concept to be another medical myth that should be dispelled, similarly to many other myths surrounding the diagnosis and management of anaphylaxis.30 The implications of our study should be considered when choosing a medical intervention for an IS in the H&N region. An IS in this region should not warrant immediate self‑administration of adrenaline. We believe that a decision whether to use adrenaline should be based on clinical symptoms and not the IS site.18 However, medical interventions were not assessed in our study.
The results of the multivariate analysis concerning the association of grade IV SRs and age are discussed in detail in Supplementary material (Appendix S2).
Limitations of the study
The major limitation of our study is the cross‑sectional design. Our results might be biased because we examined a preselected group of patients, as they all had presented severe reactions to an IS, which made them eligible for VIT. It is possible that the distribution of IS sites in patients with lower severity grades was different than in those with severe SRs, which might have biased our estimation of the odds of grade IV SRs related to a particular body part. In that case, our study provides even more powerful data to confirm that ISs in the H&N region do not increase the risk of severe anaphylaxis regardless of age and sex. A larger study would be needed to estimate the risk of grade IV SRs more precisely.
Conclusions
In patients with HVA with grade II SRs or higher, there is no significant relationship between Hymenoptera sting in the H&N region and subsequent grade IV SRs. Living in the village was identified as a risk factor for grade IV SRs due to ISs. Similarly, adulthood (age ≥30 years) was another independent risk factor of grade IV SRs due to ISs. We did not find any association between age and either the place of residence or the site of Hymenoptera sting; therefore, the correlation between these 2 factors and the severity of an anaphylactic reaction was independent of age.
- Biló BM, Bonifazi F. Epidemiology of insect venom anaphylaxis. Curr Opin Allergy Clin Immunol 2008; 8: 330‑337. | Crossref
- Biló BM, Rueff F, Mosbech H, et al. Diagnosis of Hymenoptera venom allergy. EAACI Interest Group on Insect Venom Hypersensitivity. Allergy. 2005; 60: 1339‑1349.
- Worm M, Moneret‑Vautrin A, Scherer K, et al. First European data from the network of severe allergic reactions (NORA). Allergy. 2014; 69: 1397‑1404. | Crossref
- Worm M, Eckermann O, Dolle S, et al. Triggers and treatment of anaphylaxis: an analysis of 4,000 cases from Germany, Austria and Switzerland. Dtsch Arztebl Int. 2014; 111: 367‑375.
- Worm M, Francuzik W, Renaudin JM, et al. Factors increasing the risk for a severe reaction in anaphylaxis: An analysis of data from The European Anaphylaxis Registry. Allergy. 2018; 73: 1322‑1330. | Crossref
SUPPLEMENTARY MATERIAL
ARTICLE INFORMATION