Tele-cardio-onco AID: a new concept for a coordinated care program in breast cancer (BREAST-AID): rationale and study protocol



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Tele-cardio-onco AID: a new concept for a coordinated care program in breast cancer (BREAST-AID): rationale and study protocol
Introduction
Cardiovascular (CV) disease and cancer constitute the main causes of death in the modern world, and every effort should be made to reduce these negative trends.1,2 Breast cancer (BC) is the most common malignancy in women, both in Poland and across Europe, and remains the leading cause of cancer‑related death. The most significant risk factors for BC include genetic predisposition, exposure to estrogens, ionizing radiation, and low parity. Interestingly, BC also shares significant risk factors with CV disease, such as the Western‑style diet, obesity, age, and alcohol consumption.3
The aim of this study is to develop a cardio‑oncological care program, “ON‑CARDIO,” for patients with BC.4 Specifically, the study aims to investigate: 1) whether the introduction of the “ON‑CARDIO” telemedicine care program will improve the attainment of CV prevention goals as set out in current European guidelines; 2) the type and number of cardio‑oncological interventions; 3) arrhythmia frequency and relationship with oncological therapy (via electrocardiogram [ECG] telemonitoring using the AliveCor Kardia Mobile EKG application [Alive Cor Inc, Mountain View, California, United States]); 4) the relationship between cardio‑oncological interventions, control of CV risk factors, and the rate of CV complications in patients with BC; 5) the influence of cardio‑oncological interventions on various predetermined biochemistry parameters; 6) the influence of oncological therapy in BC on left ventricular function assessed by echocardiography, potential arrhythmia assessed by ECG and 24‑hour Holter monitoring, blood pressure (BP) assessed by office BP measurements and 24‑hour ambulatory BP monitoring (ABPM).
The research hypothesis assumes that the implementation of complex coordinated cardio‑oncological care using the “ON‑CARDIO’’ program will help achieve cardio‑oncological prevention goals, determine the demand for cardio‑oncological interventions, and contribute to the early detection of cardiac complications, including arrhythmias, thus potentially improving prognosis in BC patients.
Patients and methods
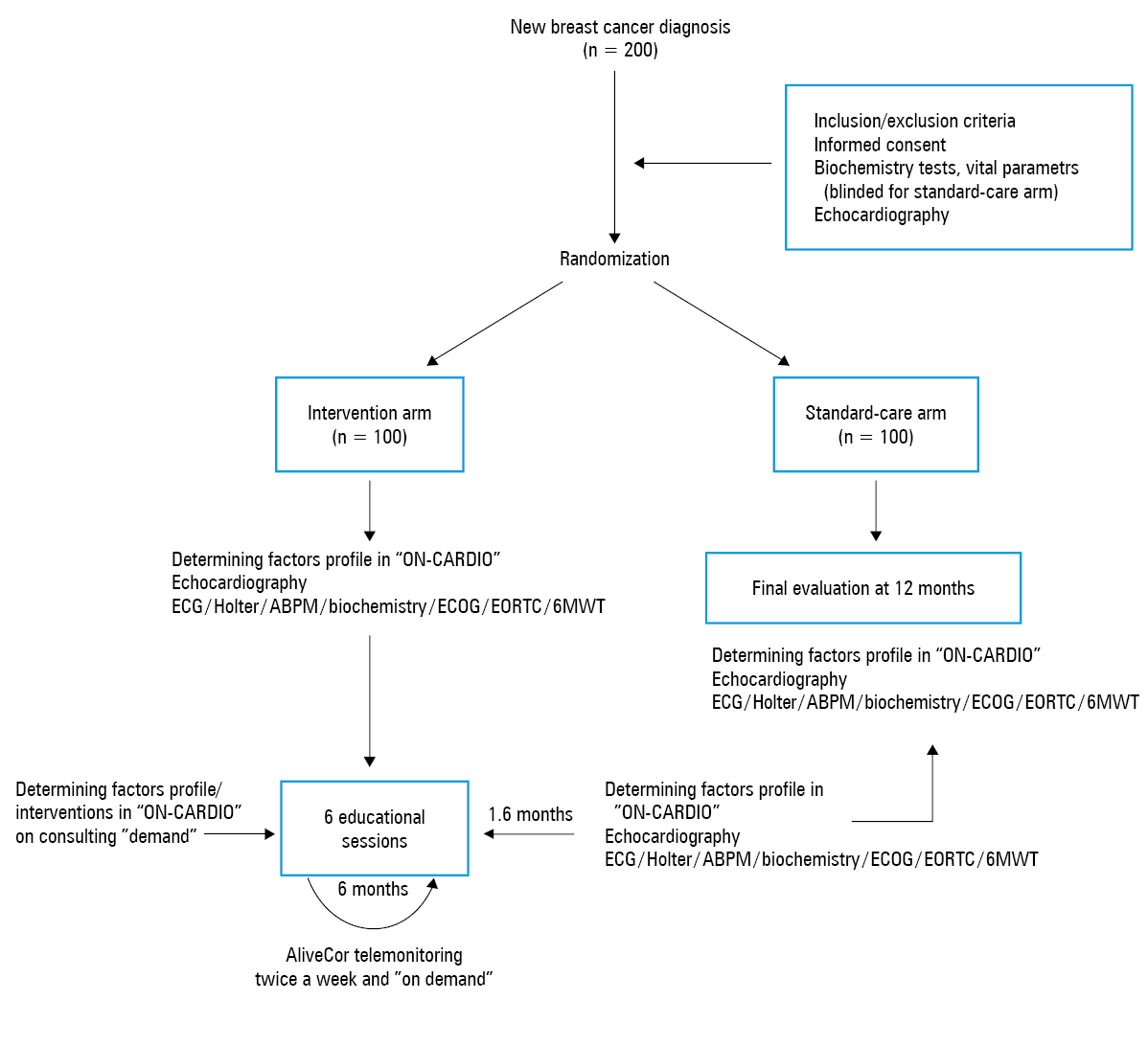
The study group will include 200 patients with newly diagnosed BC, recruited prior to commencing oncological treatment. The follow‑up will last 12 months.
The inclusion criteria are as follows: informed consent, age of 18 years or older, new diagnosis of BC, planned anticancer therapy, life expectancy exceeding 12 months, and stable condition enabling performance of planned tests, regardless of cancer stage. The exclusion criteria include pregnancy, history of atrial fibrillation (AF), and lack of the patient’s or family’s ability to use a smartphone necessary for ECG telemonitoring.
The study was approved by a local bioethics committee. Prior to randomization, each patient will undergo laboratory testing (N‑terminal pro‑B‑type natriuretic peptide, troponin, C‑reactive protein, hemoglobin A1c, lipid profile) and baseline measurements including BP, heart rate, weight, height, waist circumference, and echocardiography. Patients will then be randomized in a 1:1 ratio either to an intervention arm or a standard‑care arm.
Intervention arm
Following enrollment, 15 factors will be assessed and recorded using the “ON‑CARDIO” program, installed on dedicated tablets used for periodic reassessment of the following factors during the study: 1) factors associated with prevention (physical activity, diet, obesity, smoking, alcohol); 2) factors associated with vital parameters (BP, heart rate); and 3) factors associated with treatment (ECG, cardioprotective therapy, anticoagulant therapy, hypoglycemic therapy, lipid‑lowering therapy, psychotherapy, alternative paramedical anticancer therapy, and AliveCor compliance).
Patients in the intervention arm will undergo coordinated cardio‑oncological training that will encompass: 1) participation in 6 educational workshops over the first 6 months, delivered by qualified nurses, dieticians, physiotherapists, and psychologists. They will also be provided with instruction on how to perform home‑based exercises; 2) the following investigations at baseline and at 1, 6, and 12 months: echocardiography, ECG, 24‑hour Holter monitoring, ABPM; assessment of Eastern Cooperative Oncology Group performance status; assessment of the quality of life according to the European Organization for Research and Treatment of Cancer questionnaire; and 6‑minute walk test; 3) participation in ECG telemonitoring over the first 6 months aiming at AF screening (following appropriate training in the use of the Alive Cor application).
Standard‑care arm
Following randomization, patients will remain over 12 months under standard care. At the end of the study period, the groups will be compared regarding the number of received cardio‑oncological interventions, cardiac complications over the last 12 months, and CV test results, as shown in Figure 1.
Statistical analysis
Baseline characteristics of participants will be compared with the χ2 test, Fisher exact test, or t test, as appropriate. The changes in baseline parameters at follow‑up timepoints will be assessed by repeated‑measures analysis of variance with pairwise comparisons. The correlations between continuous variables will be calculated using the Pearson correlation coefficient. The rate of major adverse outcomes and cardio‑oncological consultations will be compared between groups using the Cox regression. A 2‑tailed P value of less than 0.05 will be considered significant. All statistical analyses will be performed using R 3.4 (R Foundation for Statistical Computing, Vienna, Austria).
Discussion
Both preventing CV disease in BC patients and reducing the risk of cardiac complications of anticancer therapy are highly significant goals.1 Published evidence suggests that CV disease is the major cause of competing mortality in women with BC, and that women with BC have higher CV risk than those without.5 However, this increased risk may be partially due to the side effects of anticancer medication, as CV prevention programs are rarely implemented in oncological patients.6 As a result, we know little about the efficacy of risk‑reduction programs in this population. We do know, however, from large European preventive cardiology programs such as EUROACTION, that lifestyle changes and risk factor reduction can have significant positive impact on individuals’ health both in primary and secondary prevention of CV diseases.7 Therefore, we aim to investigate whether similar benefits might be seen in patients diagnosed with BC.
Previous studies have demonstrated an increased prevalence of AF in patients with BC.1,8 Interestingly, the Women’s Health Study indicated that cancer is a significant risk factor for AF, notably in the first 90 days after cancer diagnosis, but not thereafter. The study suggested that acute transient conditions associated with a new cancer diagnosis, such as surgery or cancer‑related complications, may contribute to the development of AF.8 However, data on arrhythmic complications of oncological therapy in BC are limited.1 This may be in part due to imperfect methods used for arrhythmia detection and the asymptomatic or transient nature of these disorders. Yet, ECG telemonitoring, such as that achieved by the AliveCor Kardia Mobile device, may overcome some of these problems.9 To date, ECG telemonitoring has not been used in patients undergoing treatment for BC. However, their disease and the complex nature of their care predisposes them to arrhythmias.
The relationship between BP and BC treatment is complex. Elevated BP is of course a major risk factor for CV disease, and poor BP control may increase the risk of cardiotoxicity from anticancer treatments.1 Data from available studies on the effect of oncological therapy in BC and BP control are extremely limited and frequently lacking due to imperfect methodology.1
In recent years, there has been a significant expansion in the use of telemedicine to improve safety and efficacy of treatment as well as to improve patient education.10 Currently, in oncology, the use of telemedicine is focused on the decision‑making process and on remote monitoring of symptoms in palliative patients.11 We are unaware of any current attempts to use telemedicine in preventive care, such as screening for arrhythmias, in oncological patients, although they have a considerable risk of arrhythmias during oncological therapy.
This BREAST‑AID study will address these unanswered questions and contribute to the development of telemedicine and preventive care in patients with BC.4
The implementation of managed care programs has had notable success in Poland, for example, in patients after myocardial infarction.12 Managed care programs are soon to be implemented also in other areas, such as in patients with heart failure or in oncology. Given the increased incidence of CV risk factors in patients with BC, as well as the evidence indicating increased CV mortality in cancer survivors, we believe this group of patients stand to benefit from coordinated cardio‑oncological care programs. The development of the “ON‑CARDIO” program in BC patients might provide the basis for similar care programs in patients diagnosed with different cancers in the future.
- 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines. Eur Heart J. 2016; 37: 2768‑2801. | Crossref
- Kawecka‑Jaszcz K, Bednarek A, Styczkiewicz K. Management of oncology patients with history of cardiovascular diseases . Onkol Prak Klin. 2009; 5: 83‑91.
- Senkus E, Kyriakides S, Ohno S, et al. Primary breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow‑up. Ann Oncol. 2015; 26: v8‑v30. | Crossref
- Styczkiewicz K, Styczkiewicz M, Medrek S, et al. Breast cancer: tele- cardio- onco aid care programme (BREAST‑AID study). Eur Heart J. 2018; 39. | Crossref
- Khouri MG, Douglas PS, Mackey JR, et al. Cancer therapy‑induced cardiac toxicity in early breast cancer: addressing the unresolved issues. Circulation. 2012; 126: 2749‑2763. | Crossref
ARTICLE INFORMATION