Noninvasive assessment of liver status in adult patients after the Fontan procedure
Key words: adult patients, Fontan procedure, liver stiffness, shear wave elastography



 CC BY-NC-SA 4.0
CC BY-NC-SA 4.0
Noninvasive assessment of liver status in adult patients after the Fontan procedure
Introduction: A hemodynamic derangement in Fontan circulation causes liver pathology known as Fontan‑associated liver disease. Although liver biopsy is a standard for diagnosis of liver fibrosis, noninvasive methods are being developed, including shear wave elastography (SWE).
Objectives: We aimed to evaluate the degree of liver stiffness (LS) using SWE in patients with Fontan circulation in a long‑term follow‑up and to investigate a relationship between patient characteristics and LS.
Patients and methods: The study included 59 patients after the Fontan procedure. Clinical examinations and laboratory tests were performed. According to the stage of LS, patients were divided into 2 subgroups: group 1 (METAVIR stages F1 and F2) and group 2 (METAVIR stages F3 and F4). The ratio of aspartate transaminase to alanine transaminase, aspartate transaminase‑to‑platelet ratio index (APRI), fibrosis‑4 (FIB‑4) score, and Forns index were assessed.
Results: The median LS was 9.1 kPa (interquartile range, 3.9–18.5 kPa). Five patients (9%) demonstrated LS in stage F1; 14 (26%), F2; 28 (52%), F3; and 7 (13%), F4. Group 2 had significantly higher aspartate transaminase and γ-glutamyltranspeptidase levels, APRI, FIB‑4, and Forns index, and lower platelet count than group 1. A canonical correlation analysis indicated that LS and thrombocytopenia were related to time from the Fontan procedure, age at procedure, and single ventricular ejection fraction.
Conclusions: We showed that adult patients after the Fontan procedure develop liver dysfunction. Time from surgery, age at procedure, and single ventricular ejection fraction are related to the degree of LS assessed by SWE. Finally, SWE, APRI, Forns index, and FIB‑4 score may help assess the degree of liver fibrosis.
Introduction
The Fontan procedure was first described over 40 years ago and still remains the standard surgical treatment for patients with a functional single ventricular heart, affecting 35 per 100000 newborns.1-3 It is considered one of the most complex congenital heart diseases. During the procedure, a systemic venous return is directly connected with pulmonary circulation, without a subpulmonary pump.1,4,5 As a result, the circulatory system is hemodynamically less efficient.
Although the Fontan procedure is associated with low mortality, once patients reach adulthood, they can develop various cardiac and extracardiac complications, including plastic bronchitis and kidney or liver dysfunction. These complications influence the patient’s life expectancy and quality of life.6,7
The characteristic hemodynamic derangement in Fontan circulation causing liver abnormalities and pathology is commonly identified as Fontan‑associated liver disease (FALD).2,8 This can lead to nodular hyperplasia, cirrhosis, and hepatocellular carcinoma associated with ascites, variceal bleeding, and encephalopathy. Moreover, it is related with higher late morbidity and mortality in this particular population.8-10
Recent studies have shown that elevated venous pressure (3- to 4‑fold in comparison with normal) affects portal pressure and is common among patients with Fontan circulation. As a consequence, it can drive the activation and transformation of stellate cells into collagen‑depositing myofibroblasts and increase proinflammatory activity, leading to liver fibrosis.2,11,12 However, the pathogenesis of FALD is different and more complex than in other liver diseases, such as chronic hepatitis.12
Although percutaneous liver biopsy is the standard method for the diagnosis and evaluation of liver fibrosis, noninvasive tests (including biochemical tests, shear wave elastography [SWE], and magnetic resonance elastography) have become more clinically relevant and useful, with good sensitivity and specificity in the detection and evaluation of the degree of liver disease among patients with various hepatic disorders, including FALD. Fibrosis scores such as the ratio of aspartate transaminase (AST) to alanine transaminase (ALT) (AST/ALT ratio), AST‑to‑platelet ratio index (APRI), Forns index, and fibrosis‑4 (FIB‑4) score are based on widely used biochemical and clinical parameters.7-9,13,14
Shear wave elastography is the most accurate noninvasive method for the evaluation of liver stiffness (LS)15,16 and shows a positive correlation between histologic liver damage and stiffness.17,18 This technique has been validated for most hepatic diseases and has reduced the number of liver biopsies performed, along with the occurrence of possible complications such as bleeding, abdominal pain, or peritonitis.
Currently, effective methods for the diagnosis of FALD and the main factors influencing the degree of liver fibrosis are popular research areas. The aim of our study was to evaluate, in a long‑term follow‑up, the degree of LS using SWE among adult patients who had undergone the Fontan procedure and to investigate the relationship between patient characteristics (such as medical history, laboratory parameters, and echocardiographic data) and the degree of LS in these patients. Patients were followed for a minimum of 6 months (up to 24 months).
Patients and methods
Patients
This retrospective study included 59 adult patients with Fontan circulation, followed at the Department of Cardiac and Vascular Diseases, Institute of Cardiology in Kraków, Poland, between 2015 and 2017. The exclusion criteria were as follows: current infection, inflammation, major trauma, pregnancy, diabetes, and history of alcohol abuse.
Study protocol
The following information was recorded for each patient in the study: type of cardiac malformation, history of cardiac operations, age at the time of surgical repair, type of systemic ventricle, comorbidities (protein‑losing enteropathy, arrhythmia), laboratory tests, oxygen saturation, New York Heart Association functional class, vital signs, weight, height, echocardiography, and SWE.
The severity of liver disease was assessed using the Child–Pugh scale (including total bilirubin, albumin, international normalized ratio [INR] level, presence of ascites, and encephalopathy), VAST score (including the presence of varices, ascites, splenomegaly, or thrombocytopenia), and Model For End‑stage Liver Disease Excluding INR (MELD‑XI). According to the stage of LS assessed by SWE, patients were divided into 2 subgroups depending on the stage of fibrosis: group 1 (METAVIR stage 1 or 2 [F1, F2]) and group 2 (METAVIR stage 3 or 4 [F3 and F4]).
The study protocol was approved by the local ethics committee (No. 1072.6120.110.2017). Each participant provided informed consent prior to participation in this study.
Laboratory tests
The following laboratory parameters were measured: red blood cell count, hematocrit, hemoglobin, red blood cell distribution width, N‑terminal fragment of the prohormone brain natriuretic peptide (NT‑proBNP), as well as liver function markers including serum protein electrophoresis, ALT, AST, γ-glutamyltranspeptidase (GGTP), alkaline phosphatase (ALP), total bilirubin level, α-fetoprotein, and serologic tests for hepatitis B and C.
Furthermore, the following tests for liver fibrosis assessment were performed, allowing an estimation of several parameters calculated according to specific formulas: platelet count, AST/ALT ratio,11,19,21 APRI,19-21 FIB‑4 score,19,20 Forns index,19,20,22,23 and MELD‑XI score.20,24,25
Echocardiography
Single ventricular ejection fraction (SVEF) and valvular competence were evaluated and semiquantified by 2 experienced cardiologists using echocardiography (Vivid 7 GE Medical System, Chicago, Illinois, United States).
Abdominal ultrasonography, shear wave elastography, and vascular Doppler
Vascular Doppler and SWE were performed using Philips iU22 XMatrix Ultrasound System (Amsterdam, the Netherlands) by an experienced physician. For each patient, 10 measurements were taken for LS estimation. Doppler assessments of the main portal vein (MPV) and splenic vein were performed.
Statistical analysis
Continuous variables were expressed as mean (SD) in the case of normal distribution or as median (interquartile range [IQR]) when the distribution was other than normal. Categorical variables were reported as counts and percentages. The conformity of continuous variables to the normal distribution was analyzed using the Shapiro–Wilk test. The χ2 test, Mann–Whitney test, t test, and Kruskal–Wallis test were used where appropriate. Individual parameters were calculated using the Spearman rank test. The factors determining LS were analyzed using a canonical correlation analysis. Statistical significance was set at a P value of less than 0.05. Statistica version 13 (StatSoft Inc., Tulsa, Oklahoma, United States) was used to analyze the data.
Results
Patient characteristics
A total of 59 adult patients who had undergone the Fontan procedure (median age, 23 years [IQR, 18–46 years]; women, 37%) were included in the study. The median age of patients at the time of surgery was 4 years (IQR, 1–16 years), and the median time after surgery was 18 years (IQR, 7–34 years). Baseline characteristics of patients are presented in Table 1.
Variable | Patients (n = 59) |
Abbreviations: ACEI, angiotensin‑converting enzyme inhibitors; ARB, angiotensin receptor blocker; ASA, acetylsalicylic acid; NYHA, New York Heart Association; MRA, mineralocorticoid receptor antagonist; TGA, transposition of great arteries; VKA, vitamin K antagonist | |
Anatomic diagnosis, n (%) | |
Tricuspid atresia | 14 (35) |
Pulmonary stenosis / TGA | 13 (22) |
Double outlet right ventricle with left ventricular hypoplasia | 2 (3) |
Right ventricular hypoplasia | 39 (64) |
Hypoplastic left heart syndrome | 5 (7) |
Double‑inflow left ventricle | 1 (2) |
Common atrioventricular canal | 1 (2) |
Ventricle type, n (%) | |
Left ventricle | 47 (80) |
Right ventricle | 12 (20) |
Type of Fontan procedure, n (%) | |
Atriopulmonary connection | 4 (7) |
Total cavopulmonary connection | 55 (93) |
NYHA functional class, n (%) | |
I | 10 (17) |
II | 42 (71) |
III | 7 (12) |
IV | 0 |
Saturation, %, mean (SD) | 90.3 (6.5) |
Medications, n (%) | |
ASA | 40 (68) |
VKA | 12 (22) |
Enoxaparin | 6 (10) |
β-Blocker | 8 (14) |
ACEI | 8 (14) |
ARB | 2 (3) |
MRA | 13 (22) |
Diuretics | 6 (10) |
Sildenafil | 6 (10) |
Two patients died during the follow‑up (the first patient due to heart failure, and the second, due to heart failure with concomitant hepatocellular carcinoma).
Echocardiography
The mean SVEF was 51.4% (9.5%). Atrioventricular valve regurgitation was mild in 28 patients (47%); moderate, in 16 (27%); and severe, in 3 (7%). In 11 patients (19%), atrioventricular valve regurgitation was minimal. Fenestration was seen in 30 patients (51%). Other echocardiographic findings included: left ventricular noncompaction (1 patient), coarctation of the aorta (1 patient), coronary right ventricular fistula (1 patient), pericardial effusion (2 patients), aortic aneurysm (1 patient), and aortic valve regurgitation (21 patients: moderate in 9 patients and mild in 12 patients).
Biochemical test results
Laboratory test results are presented in Table 2. Hepatitis serology was positive in 6 patients (4 had chronic hepatitis B and 2 had chronic hepatitis C). Among liver parameters, elevated indirect bilirubin levels were the most frequent abnormality (80% of patients). High GGPT levels and low total platelet count were observed in 68% of patients. The INR was increased in 18 patients (42% of patients who were not receiving therapy with vitamin K antagonists). Reduced total protein levels were observed in 12% of patients, and abnormal albumin levels, in 8%. Protein‑losing enteropathy was observed in 9 patients (15%). Hepatic fibrosis scores, based on laboratory test results such as the AST/ALT ratio, platelet count, APRI score, Forns index, and FIB‑4 score, are also shown in Table 2.
Variable | Total value (n = 59) | METAVIR stage | P value | |||||
F1 and F2 (n = 20) | F3 and F4(n = 34) | |||||||
Data are presented as median (IQR) unless stated otherwise.
Abbreviations: ALP, alkaline phosphatase; ALT, alanine transaminase; APRI, aspartate transaminase‑to‑platelet ratio index; AST, aspartate transaminase; AST/ALT ratio, ratio of aspartate transaminase to alanine transaminase; FIB‑4, fibrosis‑4; GGTP, -glutamyl transpeptidase; MELD‑XI, Model For End‑stage Liver Disease Excluding International Normalized Ratio; MPV, main portal vein; NT‑proBNP, N‑terminal fragment of the prohormone brain natriuretic peptide; RBC, red blood cells; SVEF, single ventricular ejection fraction; Vd, diastolic velocity; Vs, systolic velocity | ||||||||
Clinical features | ||||||||
Age, y | 24.5 (18–46) | 23 (18–46) | 23(18–40) | 0.85 | ||||
Age at procedure, y | 4.9 (1–16) | 4.5 (1–16) | 4 (1–16) | 0.59 | ||||
Time after procedure, y | 18 (7–34) | 18 (7–32) | 18 (11–34) | 0.9 | ||||
Saturation, % | 92 (68–98) | 91 (82–98) | 83 (68–98) | 0.61 | ||||
SVEF, %, mean (SD) | 51.4 (9.5) | 52.1 (11.7) | 50.9 (8.7) | 0.14 | ||||
Hepatitis B, n (%) | 4 (7%) | 1 (5%) | 3 (8%) | – | ||||
Hepatitis C, n (%) | 2 (3%) | 1 (5%) | 1 (3%) | – | ||||
Laboratory parameters | ||||||||
NT‑proBNP, ng/ml | 130 (23–5539) | 119 (23–3184) | 130 (35–1794) | 0.82 | ||||
RBC, × 106/µl, mean (SD) | 5.6 (0.5) | 5.5 (0.7) | 5.7 (0.4) | 0.53 | ||||
Hemoglobin, g/dl, mean (SD) | 16.4 (1.8) | 16.3 (1.9) | 16.8 (1.7) | 0.39 | ||||
Hematocrit, %, mean (SD) | 48.6 (4.7) | 48 (5) | 49.6 (4.3) | 0.30 | ||||
Platelets, × 103/µl | 154.5 (59–322) | 173 (102–281) | 137 (59–322) | 0.02 | ||||
AST, IU/l | 25.4 (16–60) | 22 (16–60) | 28.5 (16–41) | 0.005 | ||||
ALT, IU/l | 27 (11–67) | 24.5 (11–67) | 28.5 (11–51) | 0.08 | ||||
GGTP, IU/l | 78 (25–255) | 59 (25–170) | 84 (28–255) | 0.008 | ||||
Total bilirubin, µmol/l | 20.5 (3.5–135) | 19.7 (9.5–61.6) | 20.5 (3.5–135) | 0.35 | ||||
α-Fetoprotein, ng/ml | 2.5 (0.8–18.6) | 2.5 (1–13) | 2.9 (0.8–18.6) | 0.68 | ||||
ALP, IU/l | 84 (38–364) | 79 (38–121) | 83 (47–364) | 0.75 | ||||
Total protein, g/l, mean (SD) | 72.8 (9.9) | 72.7 (8.1) | 72.4 (11.4) | 0.69 | ||||
Albumin, g/l | 43.1(20.5–50.2) | 43 (31.5–50) | 43 (20.5–48.7) | 0.72 | ||||
Liver fibrosis scores | ||||||||
AST/ALT ratio | 0.95 (0.5–2) | 0.9 (0.5–2) | 1 (0.6–1.7) | 0.84 | ||||
APRI | 0.4 (0.2–1.5) | 0.3 (0.2–0.6) | 0.5 (0.2–1.5) | 0.003 | ||||
Forns index, mean (SD) | 4.5 (1.9) | 3.9 (1.6) | 4.8 (1.9) | 0.048 | ||||
FIB‑4 score | 0.8 (0.3–3.2) | 0.6 (0.3–1.8) | 0.9 (0.3–3.2) | 0.02 | ||||
MELD‑XI score | 9.7 (1–19) | 9.1 (1–15) | 10 (1.1–19) | 0.13 | ||||
Vascular Doppler | ||||||||
MPV diameter, mm, mean (SD) | 10 (1.9) | 10.8 (1.9) | 10.7 (1.9) | 0.99 | ||||
Splenic vein diameter, mm | 8 (5–13) | 8 (6–10) | 8 (5–12) | 0.56 | ||||
Vd, cm/s, mean (SD) | 16 (5.4) | 14.2 (4.1) | 17 (5.9) | 0.12 | ||||
Vs, cm/s | 30 (18–47) | 30 (18–47) | 30 (19.8–42) | 0.30 | ||||
Vs/Vd | 2 (1.2–4) | 2 (1.6–2.7) | 2 (1.2–4) | 0.52 | ||||
Liver disease severity
Thirteen patients underwent an upper endoscopy, of whom 7 patients (54%) had varices and 7 (54%) had gastric or duodenal erosions or features of portal gastropathy. Furthermore, at least 16 patients (30%) had features of portal hypertension according to the VAST scale (score ≥2) (Table 3). According to the Child–Pugh scale of liver cirrhosis severity, 40 patients (78%) were in class A; 10 patients (20%), in class B; and 1 patient (2%) in class C. The median MELD‑XI score was 9.7 (IQR, 1–19). Moreover, 2 patients were diagnosed with hepatocellular carcinoma.
VAST scale | Number/total number (%) of patients |
Varices | 7/13 (54) |
Ascites | 6/59 (10) |
Splenomegaly | 21/44 (48) |
Thrombocytopenia, <150 × 103/µl | 25/59 (42) |
Abdominal ultrasonography
Abdominal ultrasonography was performed in 44 patients. Hepatomegaly was present in 17 patients (43%), and splenomegaly, in 21 (48%). Increased echogenicity was observed in 14 patients (32%), and liver surface nodularity, in 19 (44%). In 11 patients (25%), liver heterogeneity was shown.
Shear wave elastography of the liver
Shear wave elastography was performed in 54 patients. The median LS was 9.1 kPa (IQR, 3.9–18.5 kPa). Five of these patients (9%) had LS stage 1 (F1); 14 (26%), stage 2 (F2); 28 (52%), stage 3 (F3); and 7 (13%), stage 4 (F4).
The analysis of laboratory parameters in terms of LS (group 1 vs group 2) showed that patients with stages F3 and F4 had higher AST levels compared with patients with stages F1 and F2 (P = 0.01). Also, GGTP levels and platelet count were different between groups (P = 0.01 and P = 0.02, respectively). The comparison of other common liver parameters (ALT, ALP, total bilirubin, α-fetoprotein, and total protein and albumin), hematologic parameters (red blood cell count, hemoglobin, hematocrit), creatinine, and NT‑proBNP, did not show significant differences between groups. We also assessed the differences in liver fibrosis scores (AST/ALT ratio, APRI, FIB‑4, score, and Forns index) between groups 1 and 2 (Table 2). The APRI, FIB‑4 score, and Forns index were significantly higher in group 2 than in group 1 (Table 2).
Vascular Doppler
Vascular Doppler was performed in 41 patients. The mean (SD) MPV diameter was 10 (1.9) mm, and the median splenic vein diameter was 8 mm (IQR, 5–13 mm). The median systolic‑to‑diastolic velocity ratio was 2.0 (1.2–4). The MPV and splenic vein diameters did not differ between groups. Three patients (7%) had a planar spectrum of the MPV flow.
We did not reveal any correlations between LS and splenic and MPV diameters. In addition, no correlation was observed between the MPV diameter and systolic‑to‑diastolic velocity ratio. The splenic vein diameter negatively correlated with the platelet count (rs = –0.5). No significant correlation was seen between vascular Doppler parameters and other clinical features (type of surgery, ventricular morphology, time after the Fontan procedure, age at surgery, SVEF, or atrioventricular valve regurgitation).
Correlation between liver stiffness and biochemical findings
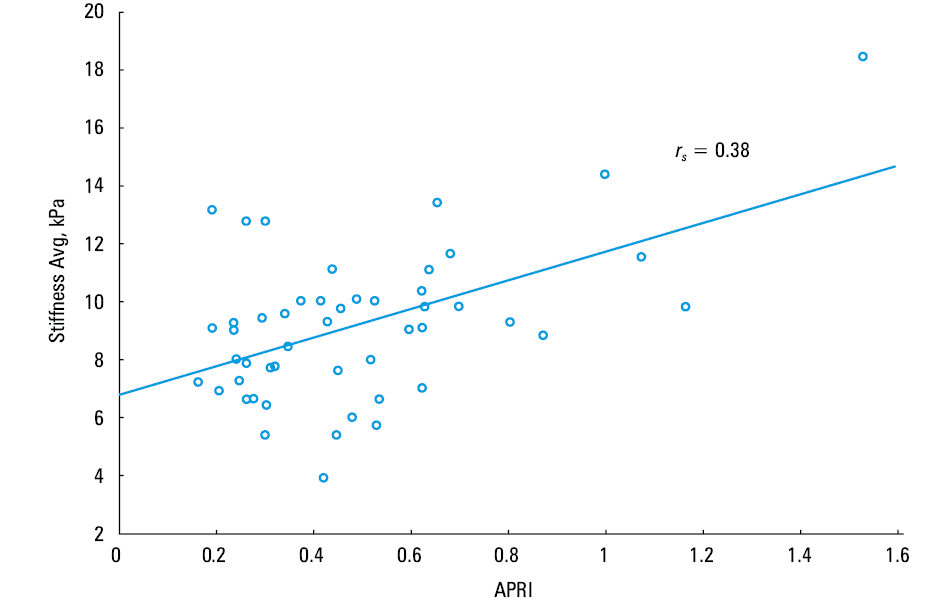
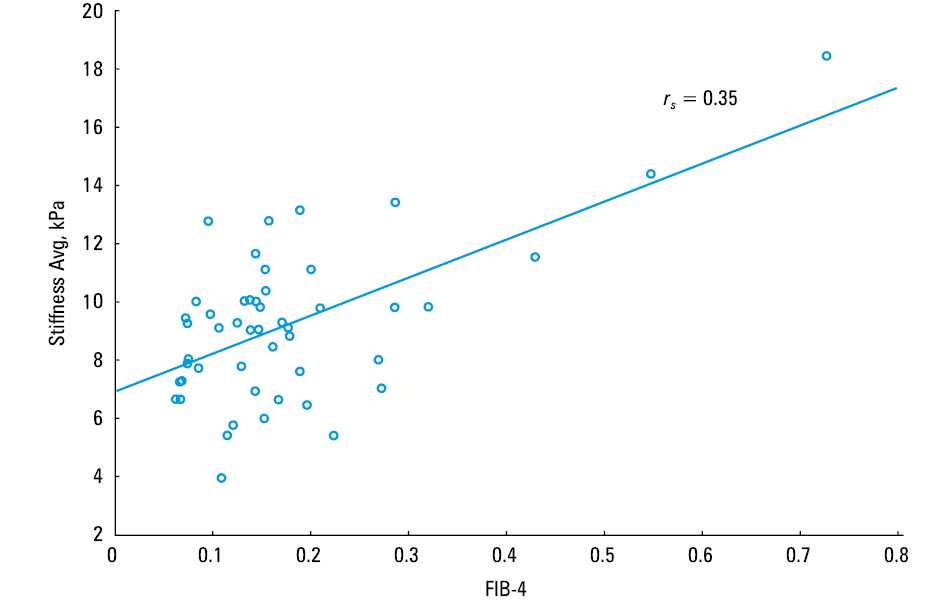
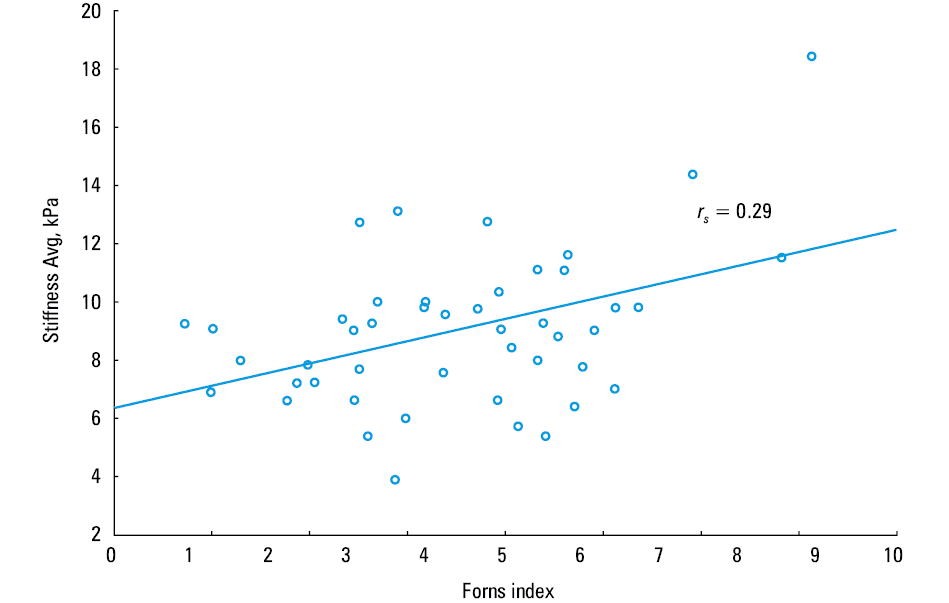
The degree of LS correlated with the platelet count (rs = –0.33), GGTP levels (rs = 0.37), and AST levels (rs = 0.33). Furthermore, LS was associated with higher APRI (rs = 0.38), FIB‑4 score (rs = 0.35), and Forns index (rs = 0.29). The correlations are presented in Figures 1–3. Other clinical parameters, including age, age at procedure, time after the Fontan procedure, single ventricular morphology, SVEF, degree of atrioventricular valve regurgitation, and biochemical liver test results did not correlate with LS as assessed by SWE.
The canonical correlation analysis was used to assess the effect of individual factors on LS and thrombocytopenia. We established a significant model that included age of the patient at the time of the Fontan procedure, time after Fontan procedure, and SVEF. The analysis indicated that LS and thrombocytopenia were strongly related to time after the Fontan procedure, with a loading vector of 0.797. Increased LS and thrombocytopenia were associated with age at the Fontan procedure, with a loading vector of –0.434, and SVEF, with a loading vector of –0.49.
Discussion
Our study was designed to evaluate liver status and the degree of LS, using noninvasive methods in 59 adult patients after the Fontan procedure. One of the most important findings is that all patients who had undergone the Fontan procedure had developed various stages of LS in a long‑term follow‑up, as assessed by SWE. Furthermore, 65% of patients with stages F3 or F4 of fibrosis had an advanced stage of LS 20 years after the procedure, as compared with 35% of patients with stages F1 or F2. Moreover, 13% of patients were diagnosed with hepatic cirrhosis, while 2 patients, with hepatocellular carcinoma. Pundi et al10 reported that the 1‑year survival rate of patients with liver cirrhosis was 57%, and the 5‑year survival rate, 35%. Considering that hepatocellular carcinoma is associated with high mortality, FALD may be one of the major determinants of mortality in adult patients after the Fontan procedure.
Time after the Fontan procedure was reported as a possible factor influencing the degree of liver fibrosis.8,12,26 This is supported by our current study, which showed that LS and liver fibrosis are strongly related to time after the Fontan procedure. These findings are in line with previous observations by Goldberg et al.12 Our study also showed that the patient age at the time of the Fontan procedure is another possible factor influencing liver fibrosis. Duorsola et al27 demonstrated that LS increased rapidly after total cavopulmonary connection. This could be a result of the new hemodynamic status immediately after the total cavopulmonary connection, with a disproportion between liver outflow and portal flow, which is not proportionally reduced.
Of note, our findings disagree with those of Johnson et al,28 who showed that increased patient age at the time of the Fontan procedure correlated with a higher grade of sinusoidal fibrosis. It has to be stated, however, that their study was a retrospective postmortem analysis, with a median interval of 14 days from the Fontan procedure to death, limited to a small group of patients who underwent the Fontan procedure at an advanced age and who had predominantly atriopulmonary Fontan connections. On the other hand, several studies demonstrated that LS increases even before the Fontan procedure, after the Glenn procedure, or directly after the Fontan procedure.29,30 The chronic low preload of a univentricular heart results in remodeling, reduced compliance with increasing diastolic pressure, low ventricular filling leading to cardiac output decrease, and liver hypoperfusion.31 This is in line with our findings, as we demonstrated that the SVEF is another significant factor related to the stage of LS.
The diagnosis and assessment of FALD is difficult, because the disease frequently remains asymptomatic over a long period of time. Moreover, our study showed that most of the biochemical markers commonly used in clinical practice did not correlate with LS, with the exception of AST, GGTP, and platelet count. Recent studies have reported that patients with Fontan circulation have abnormal liver parameters and coagulation factors.26,32 According to some authors, FALD is mostly associated with normal or only mildly increased levels of liver parameters.11,33 A multicenter study by Carter‑Kent et al34 revealed that elevated AST levels were the only biochemical parameter associated with the degree of liver fibrosis. A study by Lindsay et al9 showed that AST levels were significantly higher in patients with adverse liver outcomes (including symptomatic synthetic hepatic dysfunction, hepatocellular carcinoma or adenomatosis, and hepatorenal syndrome requiring liver transplant), when compared with the subgroup without adverse liver outcome.
A platelet count of less than 150 × 103/µl is a hallmark of hypersplenism, usually the first and sometimes the only feature of portal hypertension. Furthermore, a serial decrease in platelet count may correlate with hepatic fibrosis, and even a slight decrease in platelet count may be significant enough to diagnose liver fibrosis and hypersplenism.4,35 In our study, thrombocytopenia strongly correlated with time after the Fontan procedure and SVEF.
In our study, 16 patients (30%) had features of portal hypertension according to the VAST scale. As described by Elder et al,13 patients with features of portal hypertension, such as varices and ascites, have a 9‑fold higher risk of adverse events such as death, requirement for transplantation, or hepatocellular carcinoma.
Due to the invasiveness of liver biopsies, a number of fibrosis scores were created as a noninvasive method for liver fibrosis assessment. They are currently used in clinical practice to diagnose and assess liver fibrosis in adult patients with hepatitis B and C, alcoholic fatty disease, and nonalcoholic fatty liver disease.19,36 Fibrosis scores are based on biochemical and clinical parameters widely used in clinical practice, such as the AST/ALT ratio, APRI, Forns index, and FIB‑4 score. Although these parameters have not yet been validated in patients with FALD, there are several studies documenting the use of novel hepatic fibrosis scores.13,18,37 However, most of those studies were conducted on a pediatric population. Our study showed that the stage of LS, as measured by SWE, is associated with higher liver fibrosis scores. Patients with higher LS (stage F3 or F4) had significantly higher APRI, FIB‑4 score, and Forns index, when compared with patients in stages F1 and F2. Interestingly, Téllez et al18 demonstrated that the Forns index is the best predictor of advanced liver damage. Additionally, the MELD‑XI score can be used to assess eligibility for liver transplant.18 In our study, patients with an advanced stage of hepatic fibrosis (F3, F4) had higher MELD‑XI scores than patients with stages F1 and F2; however, the difference was not significant.
Indications for heart transplantation alone or a combined heart and liver transplant are currently widely debated. Recent studies have suggested that a combined heart and liver transplant can be considered in the treatment of patients with failing Fontan circulation. Furthermore, advanced liver fibrosis and cirrhosis should not be a contraindication to heart transplant in these patients.38 Conversely, Lin et al21 reported that double transplant in patients with compensated liver disease may be too aggressive. Importantly, other studies documented the possibility of liver function improvement or even liver fibrosis resolution when heart function is restored (after heart transplant) in patients with a cardiac origin of fibrosis.39
Further studies in a population with functionally univentricular heart are needed to better select candidates for heart transplant or combined heart and liver transplant. Moreover, a personalized approach with innovative surgical and medical methods is required to provide optimal care to this patient group.40
Study limitations
Our study has several limitations. The study group was limited, and the population was heterogeneous regarding their initial diagnoses and the type of Fontan surgery. Furthermore, the study was performed in a single center; however, to the best of our knowledge, the study includes the largest number of adult patients after the Fontan procedure in Polish population. Finally, the liver fibrosis stage was assessed noninvasively only due to the high risk of liver biopsy complications. Only 2 patients in our cohort with a suspicion of hepatocellular carcinoma underwent liver biopsy. In our study, we used SWE to estimate the LS and liver fibrosis degree as well as to validate the utility of LS scores derived from the available clinical parameters. We proved the usefulness of these scores as noninvasive markers of the liver status in routine follow‑up. It has been widely recognized, however, that the noninvasive methods for LS estimation have their inherent limitations. For example, transient elastography in FALD is problematic because of other causes of hepatic stiffness, for example, vascular congestion. Nevertheless, a real‑time 2‑dimensional SWE can monitor liver fibrosis by measuring tissue elasticity (ie, elastic modulus). Moreover, SWE is more accurate than transient elastography in detection of significant fibrosis. Finally, Kutty et al19 reported that SWE showed a positive correlation between histological liver damage and rigidity.
Conclusions
Our study revealed that adult patients after the Fontan procedure tend to develop liver dysfunction in a long‑term follow‑up. The pathomechanism of liver impairment is complex and multifactorial. Time after surgery, age at the time of the procedure, and SVEF are strongly related to the degree of LS as assessed by SWE. Moreover, SWE and liver fibrosis scales based on biochemical and clinical parameters such as the APRI, Forns index, and FIB‑4 score may be helpful in assessing the severity of liver fibrosis. Therefore, they should be considered in regular noninvasive hepatic monitoring to diagnose FALD and initiate early treatment in patients with functionally univentricular heart.
- de Leval MR, Deanfield JE. Four decades of Fontan palliation. Nat Rev Cardiol. 2010; 7: 520‑527.
- Rychik J, Veldtman G, Rand E, et al. The precarious state of the liver after a Fontan operation: summary of a multidisciplinary symposium. Pediatr Cardiol. 2012; 33: 1001‑1012.
- Fontan F, Baudet E. Surgical repair of tricuspid atresia. Thorax. 1971; 26: 240‑248.
- Daniels CJ, Bradley EA, Landzberg MJ, et al. Fontan‑Associated Liver Disease: proceedings from the American College of Cardiology Stakeholders Meeting, October 1 to 2, 2015, Washington DC. J Am Coll Cardiol. 2017; 70: 3173‑3194.
- Pająk JW, Buczyński M, Stanek P, et al. Early results of aortic arch reconstruction and bilateral pulmonary artery banding: modification of the Norwood operation for treatment of hypoplastic left heart syndrome. Kardiol Pol. 2018; 76: 770‑775.
ARTICLE INFORMATION